(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA was host to the Case-Based Session: Non-Muscle Invasive Bladder Cancer: Exploring Therapies Beyond Bacillus Calmette-Guérin Session. Drs. Christopher Baumann, Mark Tyson, Girish Kulkarni, and Tracy Rose discussed NMIBC cases and gave their insights from a multidisciplinary panel perspective.

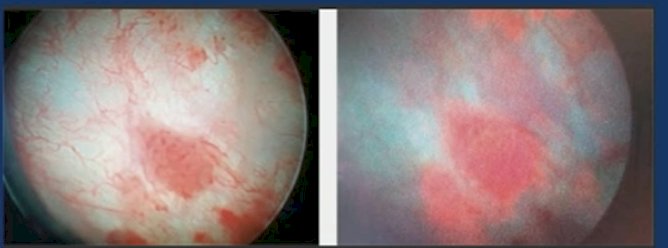
At the three-month follow-up, cystoscopy was normal, and cytology was benign, allowing the patient to proceed with maintenance BCG for three doses. However, at six months, cystoscopy revealed red patches, prompting a blue-light guided TURBT. Pathology confirmed the presence of CIS.
Dr. Schmidt posed a question to the audience: "What would you plan to do next?" The audience favored clinical trial enrollment (32%), followed by re-induction with BCG (30%).
Dr. Girish Kulkarni discussed the rationale for considering BCG re-induction. He emphasized that he follows the FDA guidance on BCG-unresponsive disease, which applies to this patient. In his practice at the Princess Margaret Cancer Centre, he would not offer BCG in this setting unless no other options were available. Instead, he would recommend Gemcitabine/Docetaxel or clinical trial enrollment. However, he noted that paradoxically, some of these patients may still respond to BCG. If no clinical trial is available, Gemcitabine/Docetaxel is not an option, and the patient declines radical cystectomy, BCG may still be considered.
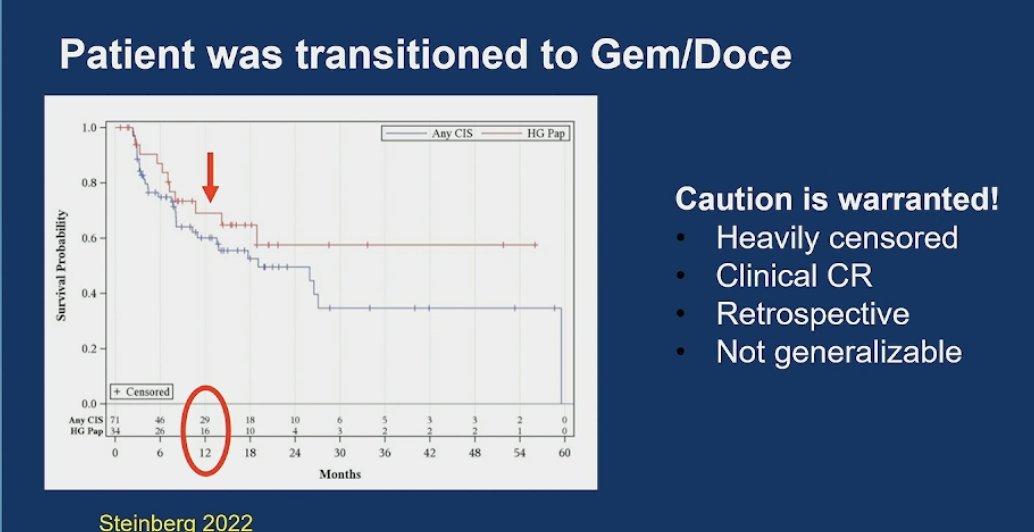
Dr. Tyson discussed the data supporting Gemcitabine/Docetaxel (GEM/Doce) in BCG-unresponsive disease. He presented updated and promising results, showing a 50% complete response (CR) rate with GEM/Doce, with comparable recurrence-free survival (RFS) at 12 months in both the CIS and papillary cohorts. However, he noted significant limitations, including heavy censoring, retrospective design, and reliance on clinical CR, making the findings less generalizable.1
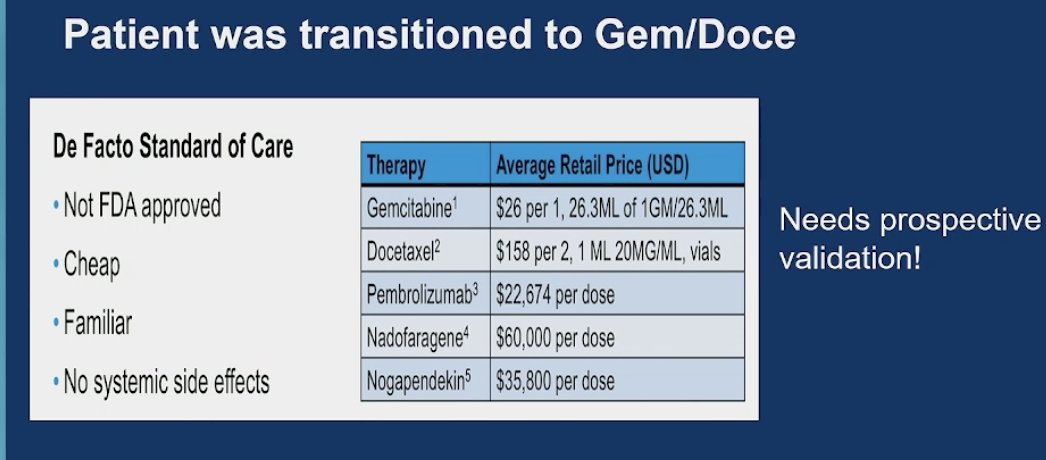
Dr. Tyson discussed another study that circulated at SUO, noting that 45-50% of his SUO colleagues reported difficulties administering GEM/Doce due to the need for approval from the chemotherapy pharmacy and a chemotherapy-licensed nurse. While not FDA-approved, GEM/Doce is cheap (Table below), well-known, and lacks systemic side effects. However, for this case, he stated that he would not proceed with cystectomy and would lean toward enrolling the patient in a clinical trial.
Moving on with this case, the patient was transitioned to GEM/Doce and again the 6-month follow-up cystoscopy was abnormal. He underwent TURBT in the OR and pathology revealed a 3cm T1 (high grade), no LVI, + CIS. The audience responded they would favor next radical cystectomy (59%), followed by Pembrolizumab (26%).
Dr. Tracy Ross discussed the FDA-approved immune checkpoint inhibitor pembrolizumab, which was tested in BCG-unresponsive high-risk NMIBC. The study included two cohorts: Cohort A (CIS with or without papillary disease) and Cohort B (papillary disease [HG Ta or any T1] without CIS). Patients received pembrolizumab 200 mg IV every three weeks for up to two years, with treatment discontinuation if high-risk NMIBC was detected. The study schema is outlined below.2
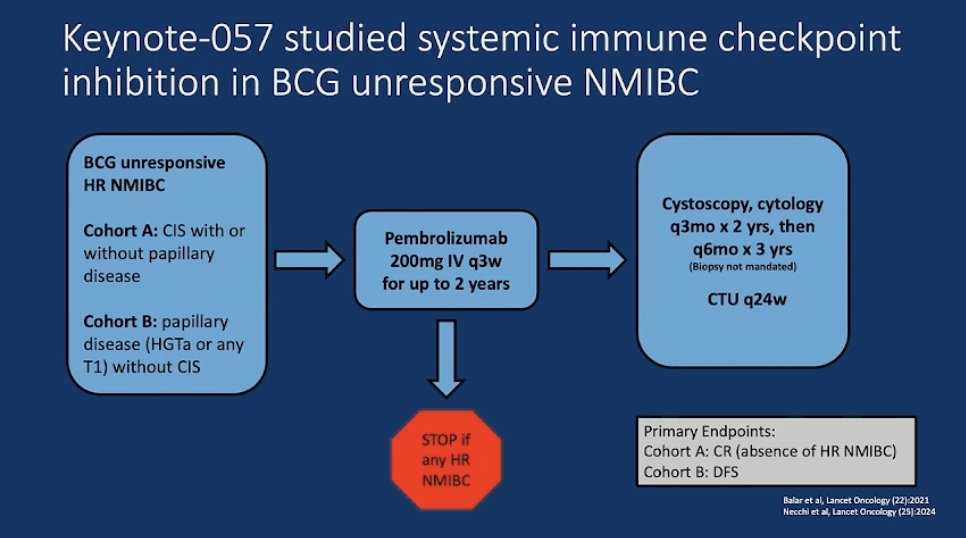
The FDA approved pembrolizumab for BCG-unresponsive disease based on results from Cohort A, where 41% of patients achieved a complete response (CR) at 3 months. The median duration of response was 16 months, with 46% maintaining a durable response at 12 months. At 12 months, the CR rate was 19% (18/96), meaning approximately 1 in 5 patients remained disease-free at one year. Similarly, in Cohort B, the 12-month disease-free survival (DFS) rate was over 43%, with a median DFS of 8 months.2
The SWOG 1605 study evaluated atezolizumab in a similar patient population, design, and treatment approach as the pembrolizumab trial, with patients receiving atezolizumab for up to one year and stopping treatment upon any recurrence of HR NMIBC. The trial had a sequential co-primary endpoint: CR at 6 months in CIS patients (confirmed by biopsy) and event-free survival (EFS) in all patients. However, an interim futility analysis after the first 25 patients led to early trial termination due to limited efficacy, with only 5 CRs among 25 patients. Among 129 evaluable patients, the CIS cohort had a 6-month CR rate of 27% (with 43% at 3 months), and the median duration of response was 17 months. In the Ta/T1 cohort, the 18-month EFS rate was 49%, with a median EFS of 15 months. Despite similar outcomes to pembrolizumab, the trial was considered negative.3
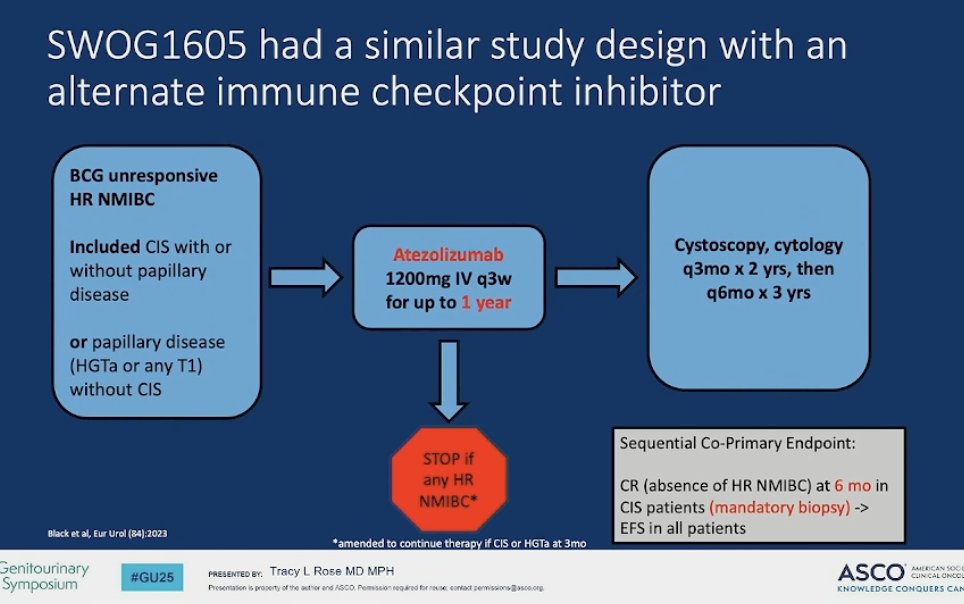
The data from both studies (pembrolizumab and atezolizumab) are fairly similar, with comparable CR rates at 3 months, 12 months, and similar EFS. Notably, consensus meetings established a benchmark of 50% CR at 6 months as an appropriate threshold for efficacy. Interestingly, despite pembrolizumab not meeting this benchmark (CR at 6 months was below 50%), it remains widely discussed and is FDA-approved for BCG-unresponsive NMIBC, while atezolizumab was considered a negative study.

In the KEYNOTE-057 trial, treatment-related grade 3-4 adverse events occurred in 13-14% of patients, with 7-8% requiring steroids for immune-related toxicities. Despite this, 79% of patients had stable or improved FACT-G physical well-being scores from baseline, as expected with systemic therapy. While most adverse events were reversible, a substantial percentage of certain immune related adverse events develop into subacute/chronic toxicity. It is important to counsel patients that there is a 1 in 5 chance of being disease-free at one year at expense of the TRAEs of the systemic therapy.
Dr. Mark Tyson discussed that he would favor the option of cystectomy, which was supported by 60% of the audience. However, for patients who refuse surgery, he suggested considering Nadofaragene Firadenovec, an FDA-approved treatment since December 2022. This non-replicating adenoviral vector-based gene therapy encodes the human IFNα2b gene and is combined with Syn, an excipient that enhances adenoviral vector attachment to the bladder uroepithelium. The localized expression of IFNα2b exerts both direct and indirect tumor-inhibitory effects within the uroepithelium. Notably, this therapy is administered intravesically, is well tolerated as monotherapy, and requires dosing only once every three months.
The approval of Nadofaragene Firadenovec was based on data demonstrating a 53% complete response (CR) at three months and a 25% CR at 12 months (Figure below) in the intent-to-treat (ITT) population. Additionally, real-world data from a multicenter study presented at GU ASCO confirmed that the durability of response observed in clinical trials holds well in post-marketing settings.
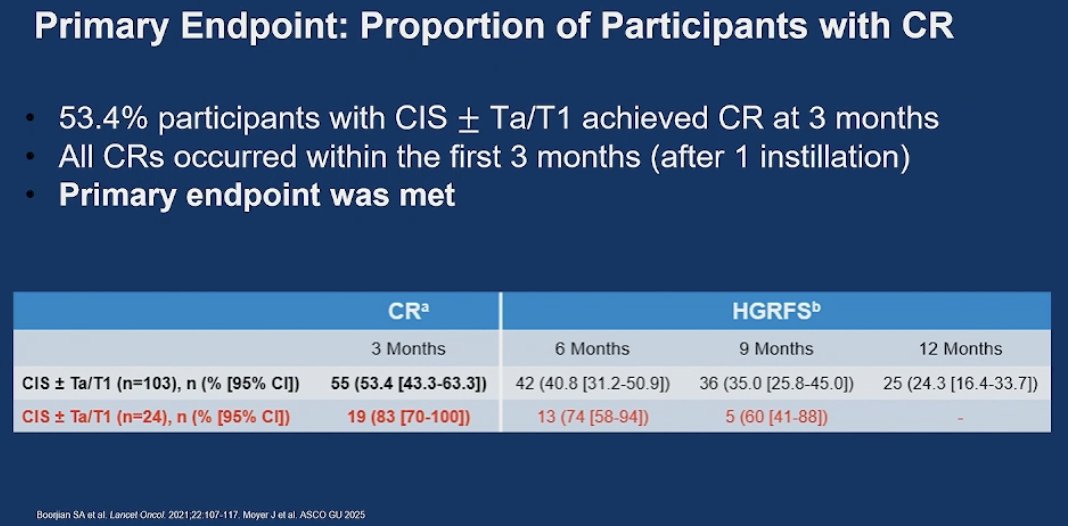
Among participants with CIS + Ta/T1 who achieved a CR at three months, the median duration of response was 9.72 months. Real-world data presented at GU ASCO reported a similar median duration of response of nine months in both CIS and papillary patients. From a urologist’s perspective, Nadofaragene Firadenovec is an attractive option for patients seeking to avoid the systemic side effects of immunotherapy. However, as with other intravesical therapies, there is a concern that cumulative toxicities may emerge over time with repeated treatments.

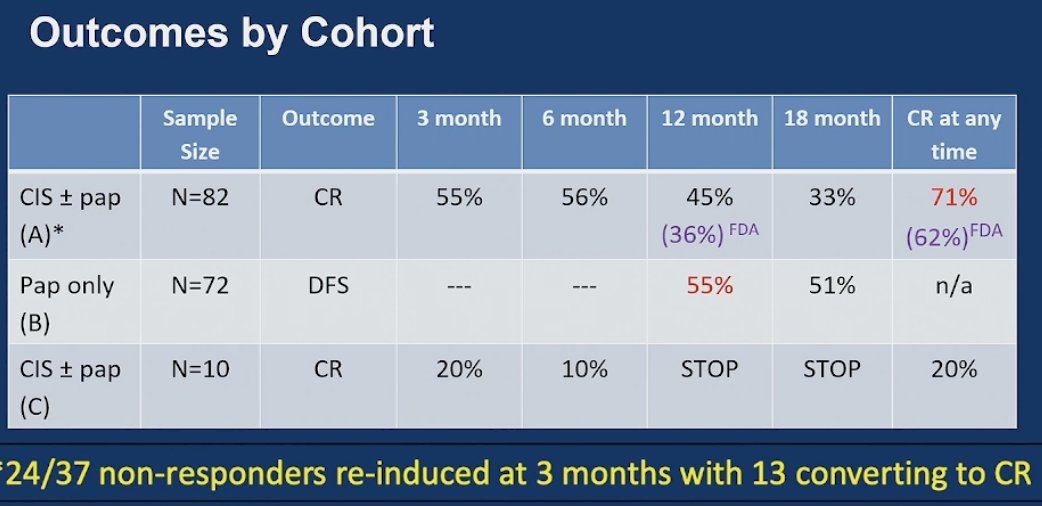
Dr. Kulkarni discussed the third FDA-approved agent, Nogapendekin alfa inbakicept (NAI, N803), an IL-15 superagonist that recruits and activates cytotoxic and NK cells, driving them to the tumor. This therapy is administered intravesically alongside BCG, with a six-week induction phase followed by maintenance for up to three years.
The study included three cohorts:
- Cohort A (BCG + N803): Primary endpoint—CR at any time (CIS cohort).
- Cohort B (BCG + N803): Primary endpoint—DFS at 12 months (papillary only).
- Cohort C (N803 alone): Primary endpoint—CR at any time (CIS cohort).
A mandatory three-month biopsy was required, and notably, re-induction at three months was allowed, this did not happen in the Keynote057 trial or the nadofaragene firadenovec trial.4
Dr. Kulkarni mentioned that in Cohort A, the CR rate at 1 year was 45%, but the FDA’s analysis adjusted it downward to 36%. The CR rate at any time was initially reported as 71%, which the FDA revised to 62%. A key caveat was that treatment re-induction was allowed in this cohort. Cohort B also demonstrated a CR, while Cohort C was stopped early, with only one patient achieving a CR.
Dr. Baumann discussed chemoradiation or trimodality therapy (TURBT and chemoRT) for recurrent high-grade T1 BCG-unresponsive disease. A recent retrospective study in Lancet Oncology found similar oncologic outcomes for trimodality therapy and radical cystectomy in T2-T4N0M0 MIBC, with overall survival favoring trimodality therapy (5-year OS: 77% vs. 72%, p<0.01) on propensity analysis.5
If trimodality therapy is as effective as cystectomy for appropriately selected patients with MIBC, why not consider it for T1 patients, where SUO/AUA guidelines recommend cystectomy, to provide an opportunity for bladder preservation? The reason this approach hasn’t been widely adopted is the lack of sufficient data.
However, recently, the NRG/RTOG 0926 trial, a single-arm study of 37 patients with recurrent high-grade T1 disease who would have been eligible for cystectomy off-trial, evaluated treatment with TURBT and concurrent chemoRT. The study demonstrated excellent disease control with favorable toxicity. The primary endpoint, 3-year freedom from cystectomy, was achieved in 88% of patients, highlighting its potential as a promising alternative to cystectomy. Since its publication, trimodality therapy has been listed as an option in the NCCN guidelines for T1 disease.6
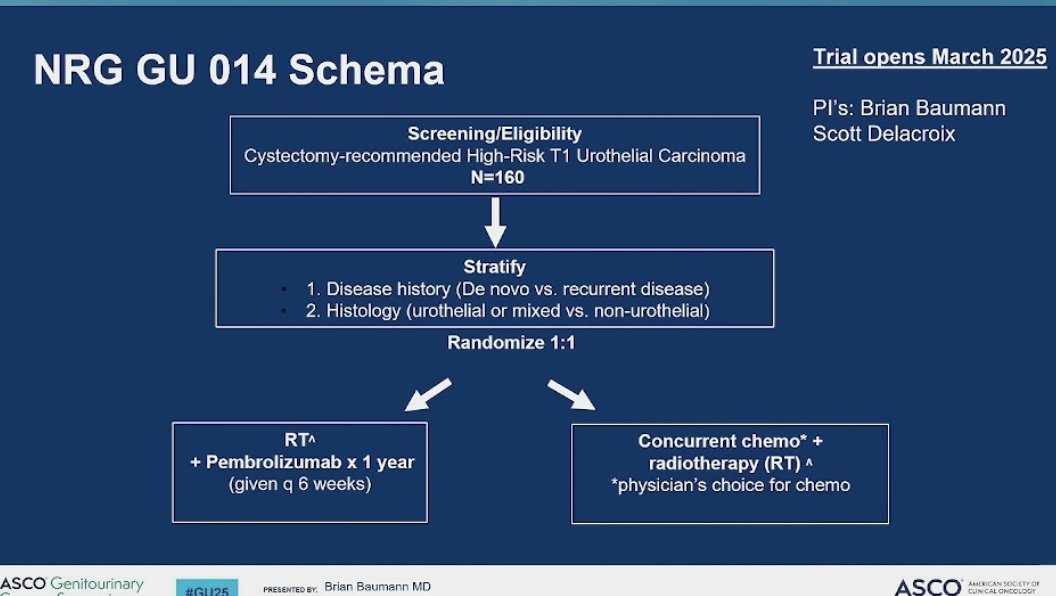
They wanted to do a follow-up trial, NRG GU014, (Opens March 2025) evaluating chemoRT versus RT + pembrolizumab for high-grade T1 bladder cancer. The hypothesis is that RT + pembrolizumab will improve bladder-intact event-free survival (BI-EFS) at 3 years compared to chemoRT. BI-EFS events include high-grade recurrent T1, MIBC, N+, M+, cystectomy, or death. The trial opened 15 years ago, but bladder-sparing treatments have since evolved.
Eligibility criteria include histologically confirmed high-grade cT1N0M0 bladder cancer meeting cystectomy criteria off-trial and one of the following:
- Recurrent high-grade T1 disease after TURBT + at least one induction course of intravesical therapy (BCG or chemotherapy if BCG unavailable).
- Persistent high-grade T1 disease at repeat TURBT (+/- focal CIS).
- High-risk features at initial or repeat TURBT (LVI or variant histology: micropapillary, sarcomatoid, plasmacytoid) with no muscle-invasive disease.
Dr. Kulkarni discussed the numerous ongoing clinical trials and presented a summary of BCG-unresponsive trials from the BCAN site. He highlighted several FDA breakthrough therapy designations and discussed these emerging treatments.

He discussed the SUNRISE-1 trial and the TARIS system, a novel drug delivery method. This system consists of 224 mg of gemcitabine within a semipermeable polymer shaped like a pretzel. The polymer contains osmotic tablets that dissolve as urine penetrates, slowly releasing gemcitabine over three weeks. This extended-release approach contrasts with conventional intravesical chemotherapy, where drug contact with the urothelium lasts only one to two hours.7
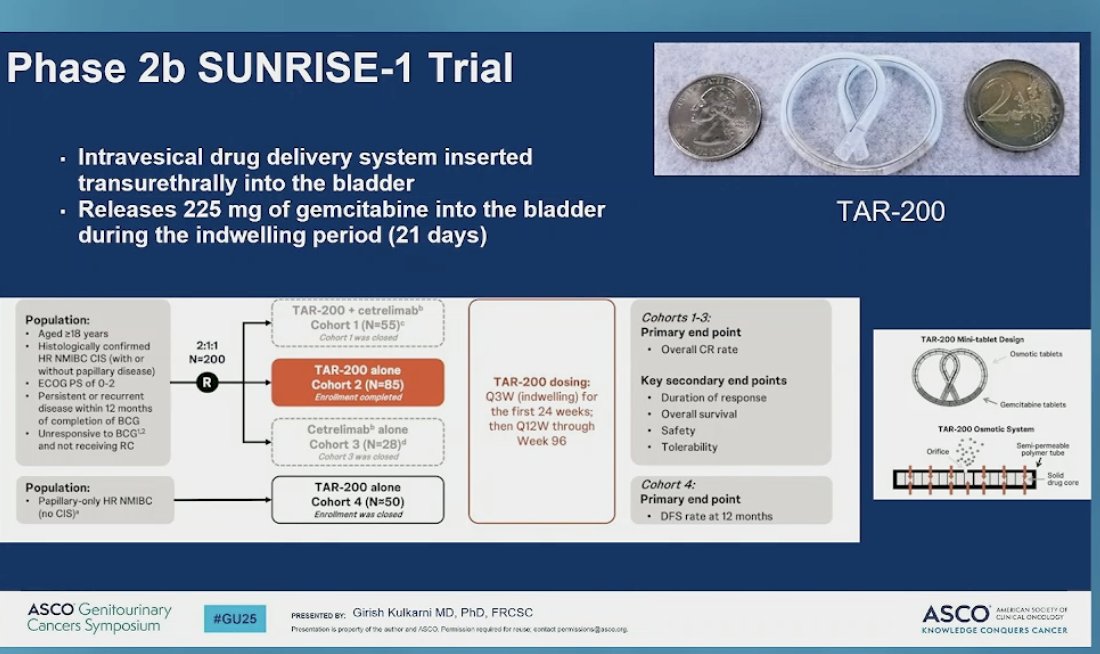
The study reported an estimated 12-month CR rate of 57.4% with TAR-200 alone, 22.8% with Cetrilimab alone, and 56.7% with the combination of TAR-200 and Cetrilimab.

The TARIS system was well tolerated, with only 9% of patients experiencing TRAEs ≥ grade 3. The most common adverse events included pollakiuria, dysuria, and urinary tract infections, all manageable by urologists. However, the device requires frequent cystoscopic exchanges—weekly for the first eight weeks, then every 12 weeks for six cycles.
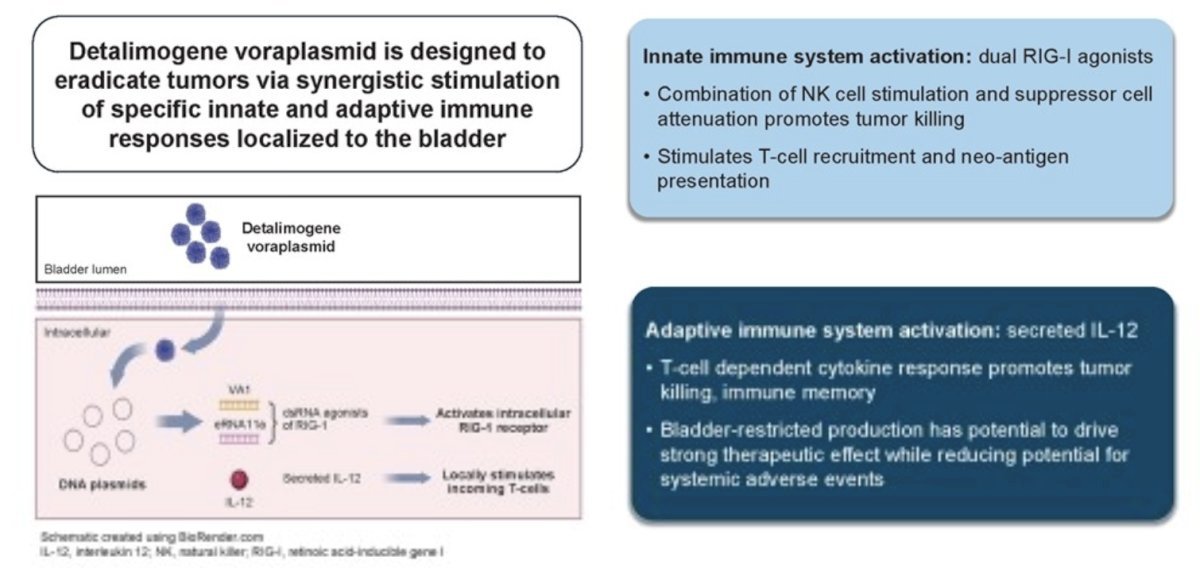
Dr. Kulkarni briefly discussed Detalimogene Voraplasmid (EG-70), an intravesical gene therapy that elicits local stimulation of anti-tumor immune responses in the bladder currently being studied in the LEGEND Phase 1/2 trial. The therapy demonstrated a 68% CR at three months in early data. The ongoing Phase II trial focuses on BCG-unresponsive CIS, and the treatment has received FDA breakthrough therapy designation.
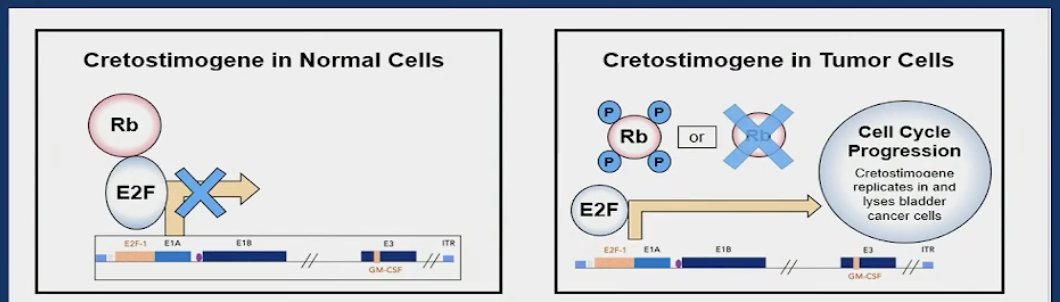
Dr. Tyson discussed Cretostimogene grenadenorepvec, an adenovirus-based replicating virus administered intravesically. It targets cancers with alterations in the Rb-E2F pathway, where the loss of Rb function leads to unregulated E2F activity, promoting selective cancer cell lysis and death.
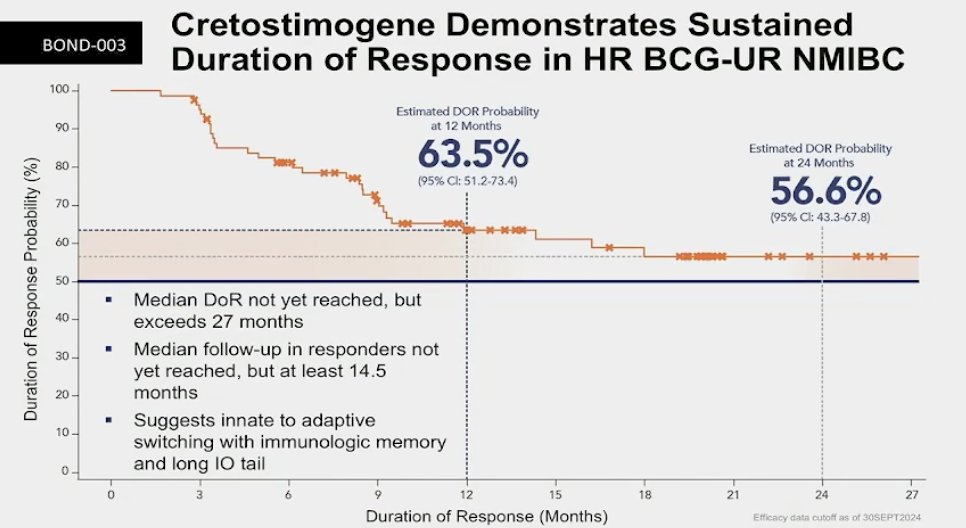
The BOND-003 study presented at SUO demonstrated promising initial results for cretostimogene grenadenorepvec, an adenovirus-based replicating virus targeting Rb-E2F pathway-altered cancers. The study reported an overall CR rate of 74.5%, with a CR rate of 46% at 12 months, though 24-month data is not yet available. At 12 months, 97.3% of patients remained free from progression to MIBC, and 90.0% had cystectomy-free survival. The CR rate was consistent across patient subgroups, with all responses centrally confirmed. These results represent some of the most compelling immunotherapy monotherapy data in this setting.
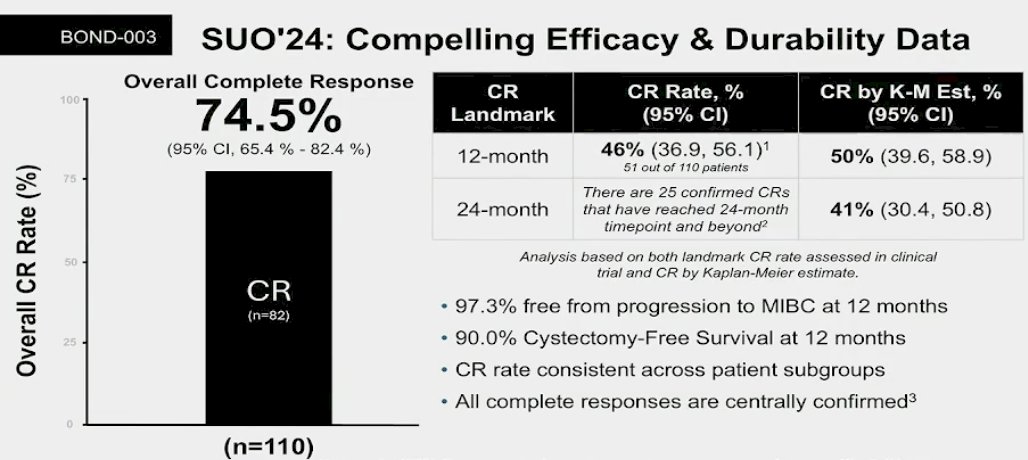
Notably, the estimated duration of response probability is 63.5% at 12 months and 56.6% at 24 months. The median duration of response has not yet been reached but exceeds 27 months. (Figure below)
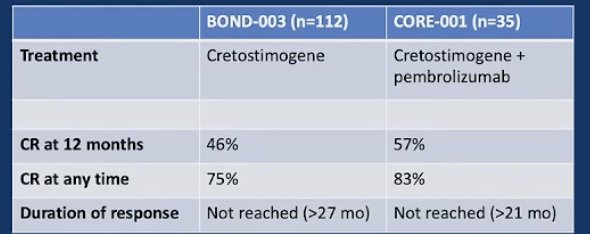
Dr. Rose moved on to discuss combination therapies, beginning with the study of CG0070 (Cretostimogene) given in combination with pembrolizumab in non-muscle invasive bladder cancer unresponsive to Bacillus Calmette-Guérin (CORE-001). The primary endpoint of the study was complete response (CR) at 12 months.

They treated 35 patients with the combination in the CORE-001 trial, which demonstrated a CR rate of 57% at 12 months and 83% at any time—an improvement compared to the monotherapy in the BOND-003 trial. Notably, 14% of grade 3 treatment-related adverse events were attributed to systemic therapy.
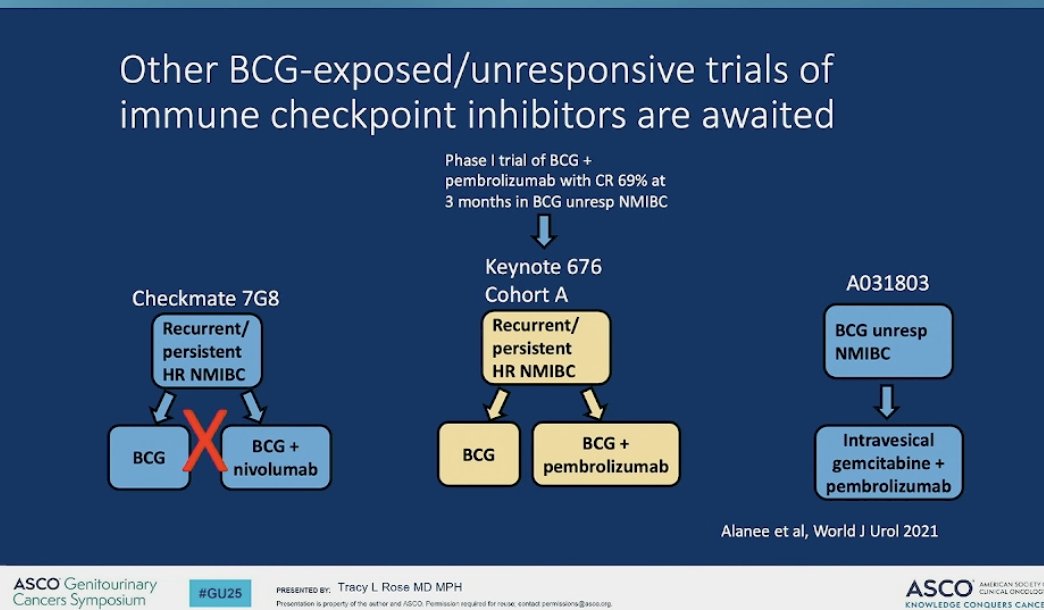
There are trials going on in both the BCG expose, and unresponsive setting. She highlighted 3 studies shown below.
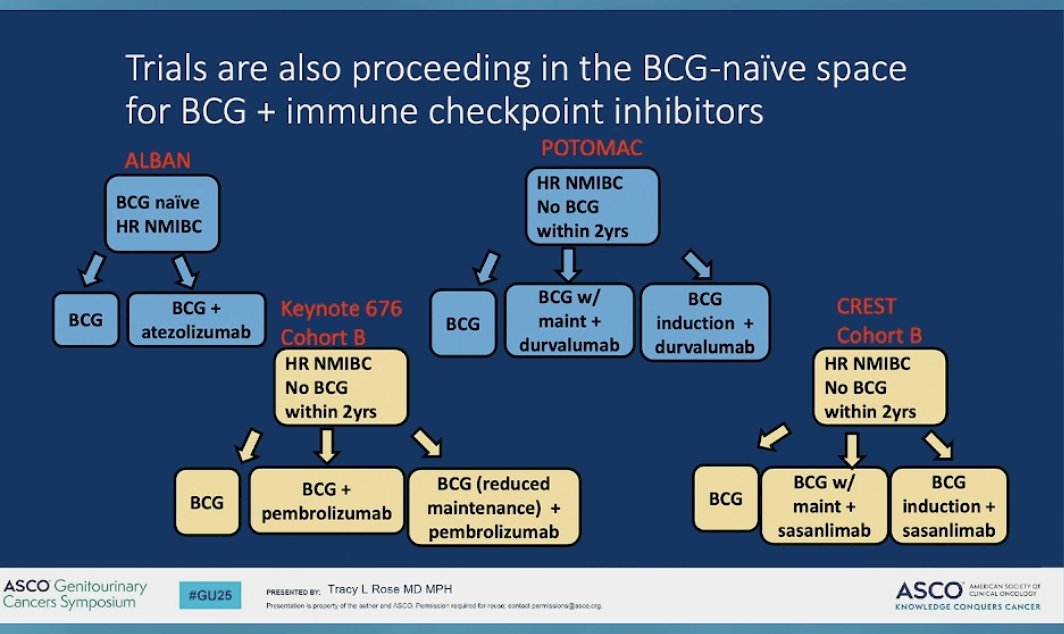
In the BCG-naïve space, she briefly touched on four studies, with their designs illustrated below. We await the results to determine if these approaches can achieve synergistic effects.
Returning to our patient: a 69-year-old man with NMIBC who has undergone four TURBTs, BCG induction with maintenance, and Gemcitabine/Docetaxel induction, now presenting with BCG-refractory high-grade T1 (following re-resection) with CIS but no LVI. The audience favored radical cystectomy as the preferred approach (54%).
Dr. Rose emphasized that radical cystectomy should be the standard treatment, given the patient's multiple intravesical therapies and high-risk NMIBC. If the patient declines, selecting an alternative therapy becomes increasingly difficult. Dr. Kulkarni also expressed concern about bladder-sparing approaches in this scenario and would prioritize radical cystectomy as the standard approach considering the biology of this disease. He noted, that he wouldn’t even re-resect this patient, since the only value is if you believe the patient has occult MIBC and it would miss the added value of neoadjuvant chemotherapy. Dr. Baumann said if the patient does not agree with radical cystectomy, it could be a good candidate for the NRG GU014 trial.
Presented by:
- Brian Christopher Baumann, MD, Radiation Oncologist at Springfield Clinic. Springfield, IL, United States.
- Mark Tyson II, MD, MPH, Urologic Oncologist at Mayo Clinic in Arizona, AZ, United States.
- Girish S. Kulkarni, MD, PhD, Urologic Oncologist at Princess Margaret Cancer Center, University Health Network, Toronto, ON, Canada.
- Tracy L. Rose, MD, MPH, Medical Oncologist at The University of North Carolina at Chapel Hill, NC, United States.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- Steinberg RL, Packiam VT, Thomas LJ, Brooks N, Vitale A, Mott SL, Crump T, Wang J, DeWolf WC, Lamm DL, Kates M, Hyndman ME, Kamat AM, Bivalacqua TJ, Nepple KG, O'Donnell MA. Intravesical sequential gemcitabine and docetaxel versus bacillus calmette-guerin (BCG) plus interferon in patients with recurrent non-muscle invasive bladder cancer following a single induction course of BCG. Urol Oncol. 2022 Jan;40(1):9.e1-9.e7. doi: 10.1016/j.urolonc.2021.03.024. Epub 2021 Jun 4. PMID: 34092482.
- Necchi A, Roumiguié M, Kamat AM, Shore ND, Boormans JL, Esen AA, Lebret T, Kandori S, Bajorin DF, Krieger LEM, Niglio SA, Uchio EM, Seo HK, de Wit R, Singer EA, Grivas P, Nishiyama H, Li H, Baranwal P, Van den Sigtenhorst-Fijlstra M, Kapadia E, Kulkarni GS. Pembrolizumab monotherapy for high-risk non-muscle-invasive bladder cancer without carcinoma in situ and unresponsive to BCG (KEYNOTE-057): a single-arm, multicentre, phase 2 trial. Lancet Oncol. 2024 Jun;25(6):720-730. doi: 10.1016/S1470-2045(24)00178-5. Epub 2024 May 10. PMID: 38740030.
- Black PC, Tangen CM, Singh P, McConkey DJ, Lucia MS, Lowrance WT, Koshkin VS, Stratton KL, Bivalacqua TJ, Kassouf W, Porten SP, Bangs R, Plets M, Thompson IM Jr, Lerner SP. Phase 2 Trial of Atezolizumab in Bacillus Calmette-Guérin-unresponsive High-risk Non-muscle-invasive Bladder Cancer: SWOG S1605. Eur Urol. 2023 Dec;84(6):536-544. doi: 10.1016/j.eururo.2023.08.004. Epub 2023 Aug 16. PMID: 37596191; PMCID: PMC10869634.
- Chamie K, Chang SS, Kramolowsky E, Gonzalgo ML, Agarwal PK, Bassett JC, Bjurlin M, Cher ML, Clark W, Cowan BE, David R, Goldfischer E, Guru K, Jalkut MW, Kaffenberger SD, Kaminetsky J, Katz AE, Koo AS, Sexton WJ, Tikhonenkov SN, Trabulsi EJ, Trainer AF, Spilman P, Huang M, Bhar P, Taha SA, Sender L, Reddy S, Soon-Shiong P. IL-15 Superagonist NAI in BCG-Unresponsive Non-Muscle-Invasive Bladder Cancer. NEJM Evid. 2023 Jan;2(1):EVIDoa2200167. doi: 10.1056/EVIDoa2200167. Epub 2022 Nov 10. PMID: 38320011.
- Zlotta AR, Ballas LK, Niemierko A, Lajkosz K, Kuk C, Miranda G, Drumm M, Mari A, Thio E, Fleshner NE, Kulkarni GS, Jewett MAS, Bristow RG, Catton C, Berlin A, Sridhar SS, Schuckman A, Feldman AS, Wszolek M, Dahl DM, Lee RJ, Saylor PJ, Michaelson MD, Miyamoto DT, Zietman A, Shipley W, Chung P, Daneshmand S, Efstathiou JA. Radical cystectomy versus trimodality therapy for muscle-invasive bladder cancer: a multi-institutional propensity score matched and weighted analysis. Lancet Oncol. 2023 Jun;24(6):669-681. doi: 10.1016/S1470-2045(23)00170-5. Epub 2023 May 12. PMID: 37187202.
- Dahl DM, Rodgers JP, Shipley WU, Michaelson MD, Wu CL, Parker W, Jani AB, Cury FL, Hudes RS, Michalski JM, Hartford AC, Song D, Citrin DE, Karrison TG, Sandler HM, Feng FY, Efstathiou JA. Bladder-Preserving Trimodality Treatment for High-Grade T1 Bladder Cancer: Results From Phase II Protocol NRG Oncology/RTOG 0926. J Clin Oncol. 2024 Dec;42(34):4095-4102. doi: 10.1200/JCO.23.02510. Epub 2024 Sep 3. PMID: 39226514.
- Michiel van der Heijden. LBA85 - TAR-200 +/- cetrelimab (CET) and CET alone in patients (pts) with bacillus Calmette-Guérin-unresponsive (BCG UR) high-risk non-muscle-invasive bladder cancer (HR NMIBC): Updated results from SunRISe-1 (SR-1). Annals of Oncology (2024) 35 (suppl_2): 1-72. 10.1016/annonc/annonc1623