(UroToday.com) The 2025 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Priyanka Chablani discussing a survey-based study of treatment sequencing after first line enfortumab vedotin + pembrolizumab in the evolving landscape of locally advanced/metastatic urothelial cancer. Enfortumab vedotin + pembrolizumab is a preferred first line option for patients with locally advanced or metastatic urothelial cancer based on the EV-302 trial.1 In this study, Dr. Chablani and colleagues sought to understand how genitourinary medical oncologists in the US treat patients who progress on first line enfortumab vedotin + pembrolizumab, and their comfort level with immune checkpoint inhibitor rechallenge after prior immune checkpoint inhibitor exposure.
The investigators convened a bladder cancer working group comprised of 11 expert locally advanced or metastatic urothelial cancer genitourinary oncologists. This group created an 11-question survey addressing key questions regarding treatment sequencing, including treatment after first line enfortumab vedotin + pembrolizumab. The survey was emailed to 227 US genitourinary oncologists from May 2024 to Aug 2024. Genitourinary oncologists in the Bladder Cancer Advocacy Network and those with a known genitourinary-focus in academic and community practices were selected. At the GU ASCO 2025 annual meeting, Dr. Chablani presented results regarding second line treatment after first line enfortumab vedotin + pembrolizumab.
This survey-based study received 78/227 responses (34%), of which 72% report seeing > 25 patients with locally advanced or metastatic urothelial cancer/year and 21% see 11-25 patients/year. Overall, 30% were in practice 0-5 years post fellowship and 17% were in practice >20 years. There were 71 (31%) oncologists that completed the second line treatment question: “If a patient has progression on first line enfortumab vedotin + pembrolizumab, how likely are you to give each of the following options as second line treatment?”
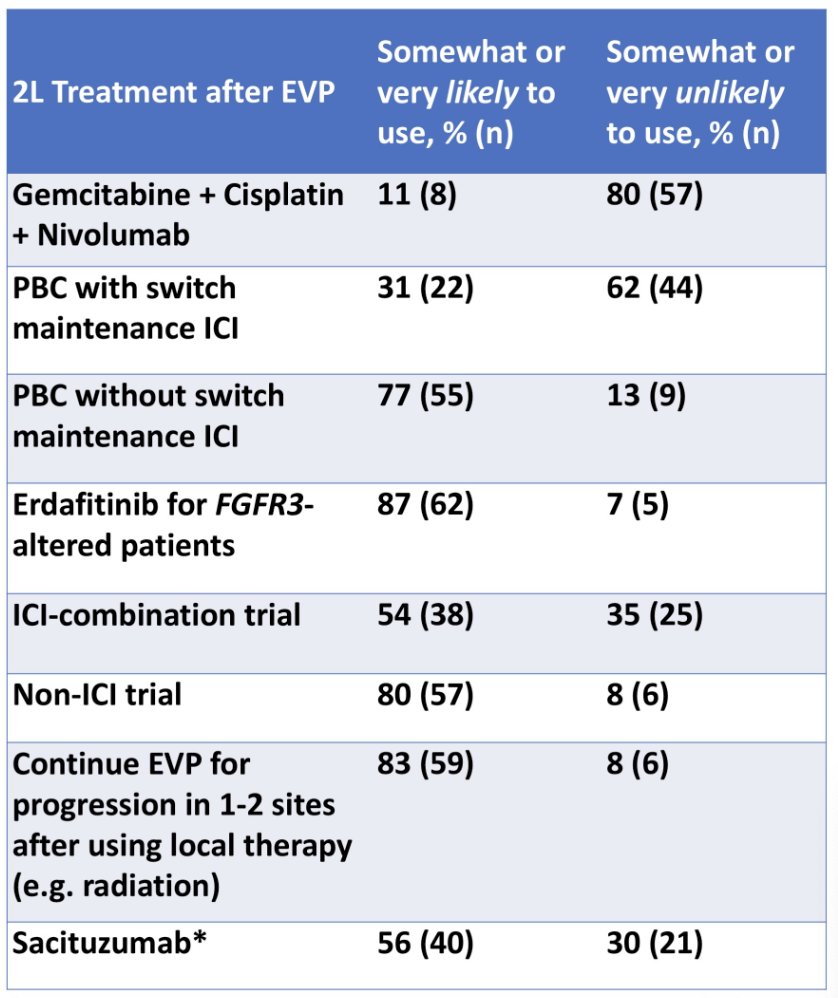
After progression on enfortumab vedotin + pembrolizumab, 77% were somewhat/very likely to give platinum-based chemotherapy, 80% would not include nivolumab with gemcitabine + cisplatin in the second line, and 62% were somewhat/very unlikely to give switch maintenance immune checkpoint inhibitor after second line platinum-based chemotherapy. For other second line options, 87% were somewhat/very likely to give erdafitinib in patients with FGFR3 alterations, and 56% were somewhat/very likely to give sacituzumab govitecan. Sacituzumab govitecan use before and after the TROPiCS-04 trial press release on May 30, 2024 shifted from 63% to 48% somewhat/very likely to use sacituzumab govitecan (and 21% to 39% somewhat/very unlikely to use). Regarding clinical trials after first line enfortumab vedotin + pembrolizumab, 80% were somewhat/very likely to recommend a non-immune checkpoint inhibitor containing trial. The limitations of this study include selection bias and a lack of clinical outcomes.
Dr. Chablani concluded her presentation discussing a survey-based study of treatment sequencing after first-line enfortumab vedotin/pembrolizumab in the evolving landscape of locally advanced/metastatic urothelial cancer with the following take-home points:
- After progression on enfortumab vedotin + pembrolizumab, most genitourinary oncologists favor platinum-based chemotherapy without combination immune checkpoint inhibitor, platinum-based chemotherapy without immune checkpoint inhibitor switch maintenance, or erdafitinib (in FGFR3-alterations) as second line therapies
- For clinical trials in the second line, more oncologists favor a non-immune checkpoint inhibitor containing regimen
- Additional data, including the impact of residual toxicity from first line enfortumab vedotin + pembrolizumab on second line treatment selection, and treatment of patients with HER-2 IHC3+ tumors, are needed to better understand treatment sequencing for patients with locally advanced or metastatic urothelial cancer
Presented by: Priyanka V. Chablani, MD, Division of Hematology/Oncology, University of Pittsburgh School of Medicine, Pittsburgh, PA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References: