(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA between February 13–15, 2025 was host to a urothelial carcinoma rapid oral abstract session. Dr. Thomas Powles presented an updated analysis from the phase III global study of enfortumab vedotin in combination with pembrolizumab (EV+P) vs chemotherapy in previously untreated locally advanced or metastatic urothelial carcinoma (la/mUC).
In the primary analysis of EV-302 (KEYNOTE-A39), the combination of EV+P nearly doubled median progression-free (PFS) and overall survival (OS) versus platinum-based chemotherapy, in patients with previously untreated la/mUC. The median PFS was 12.5 months with EV+P versus 6.3 months with platinum-based chemotherapy. Significantly, the median OS improved from 16.1 months with platinum-based chemotherapy to 31.5 months with EV+P.1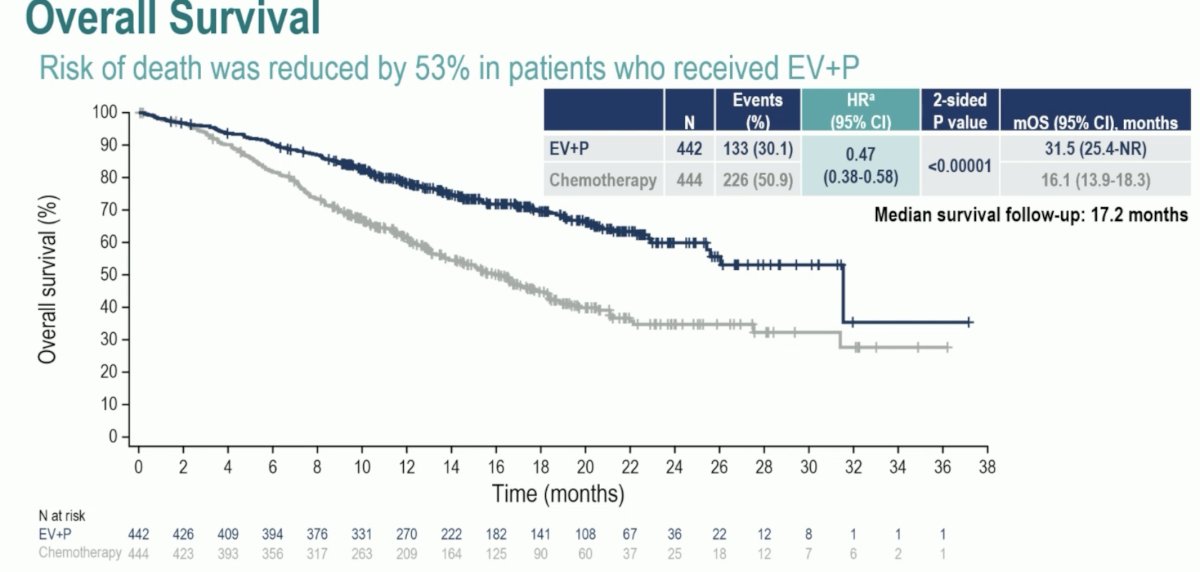
Based on these results, EV+P received approvals in many countries globally and is now considered the standard of care (SOC) in global treatment guidelines for patients with untreated la/mUC.
In this report, Dr. Powles presented 1 year of additional follow-up for EV-302 (~2.5 years of median follow-up) and an exploratory analysis of patients with confirmed complete response.
Patients in this trial were randomized in a 1:1 fashion, stratified by cisplatin eligibility, PD-L1 expression, and presence/absence of liver metastases, to EV+P (continued until disease progression per blinded independent central review [BICR], clinical progression, unacceptable toxicity, or completion of maximum cycles [35 for pembrolizumab]) versus gemcitabine + cisplatin or carboplatin for a maximum of 6 cycles. The dual primary endpoints were PFS by BICR and OS.
![Patients in this trial were randomized in a 1:1 fashion, stratified by cisplatin eligibility, PD-L1 expression, and presence/absence of liver metastases, to EV+P (continued until disease progression per blinded independent central review [BICR], clinical progression, unacceptable toxicity, or completion of maximum cycles [35 for pembrolizumab]) versus gemcitabine + cisplatin or carboplatin for a maximum of 6 cycles. The dual primary endpoints were PFS by BICR and OS.](/images/com-doc-importer/190-asco-gu-2025/asco-gu-2025-ev-302-updated-analysis-from-the-phase-3-global-study-of-enfortumab-vedotin-in-combination-with-pembrolizumab-ev-p-vs-chemotherapy-chemo-in-previously-untreated-locally-advanced-or-metastatic-urothelial-carcinoma-la-muc/image-1.jpg)
With 29.1 months (95% Cl: 28.5–29.9) of median follow-up:
- 54 (12%) patients remained on EV+P treatment and no patients remained on chemotherapy
- 218 (49%) patients in the EV+P arm and 131 (30%) patients in the chemotherapy arm remained on study
The PFS benefit with EV+P was maintained with 1 additional year of follow-up (median: 12.5 versus 6.3 months; HR: 0.48, p<0.00001).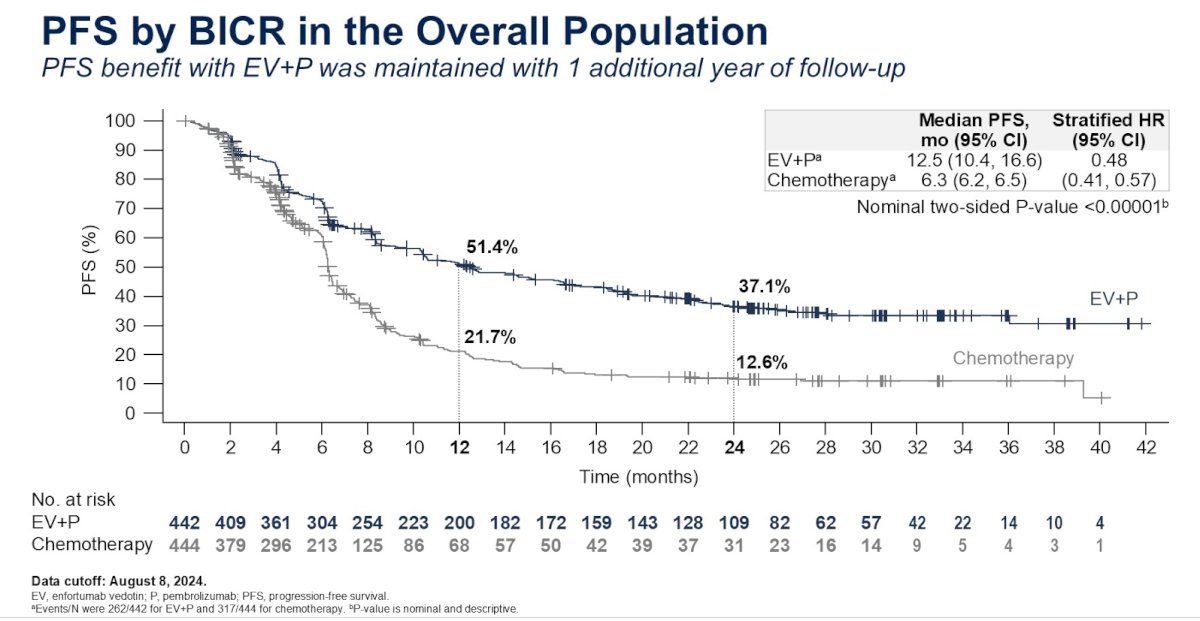
The PFS benefit was observed across all evaluable subgroups: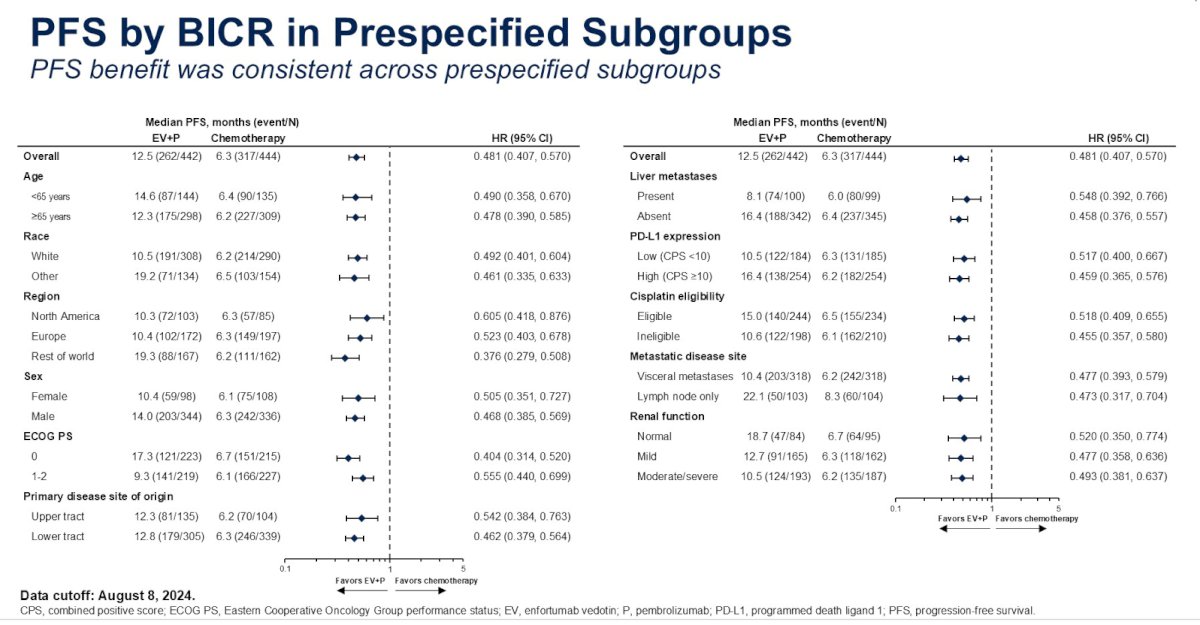
The risk of death was reduced by almost 50% in the EV+P arm (median 33.8 versus 15.9 months; HR: 0.51, 95% CI: 0.43–0.61, p<0.00001).
Subgroup analyses demonstrated consistent OS benefits across all evaluable subgroups:
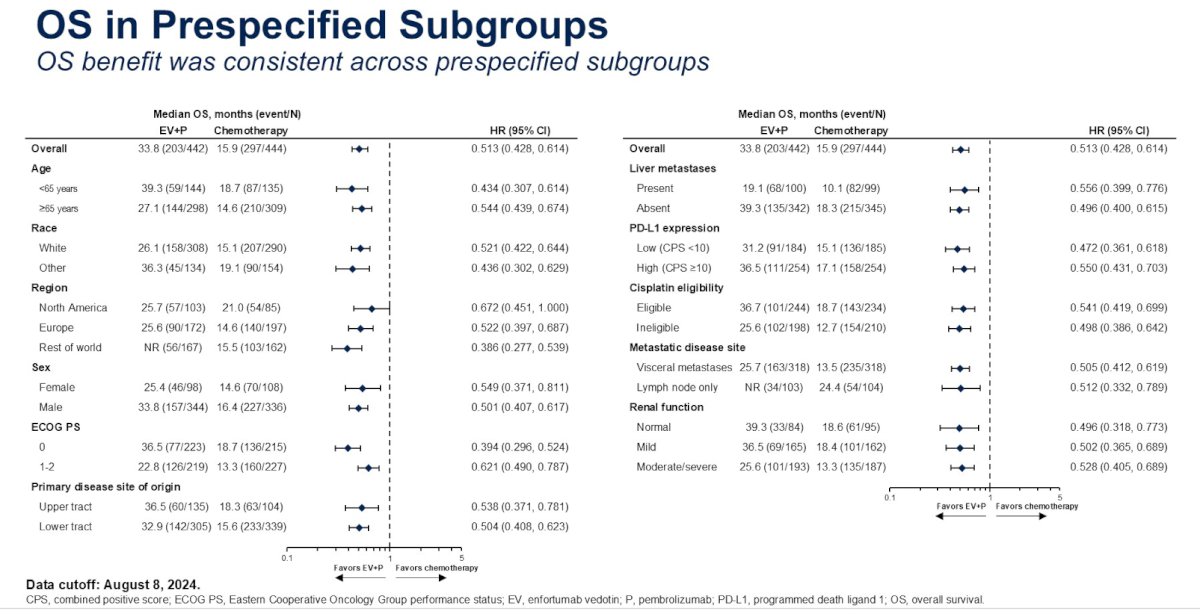
Importantly, a strong OS advantage for EV+P was observed in both cisplatin eligible (median: 36.7 versus 18.7 months) and ineligible patients (median: 25.6 versus 12.7 months).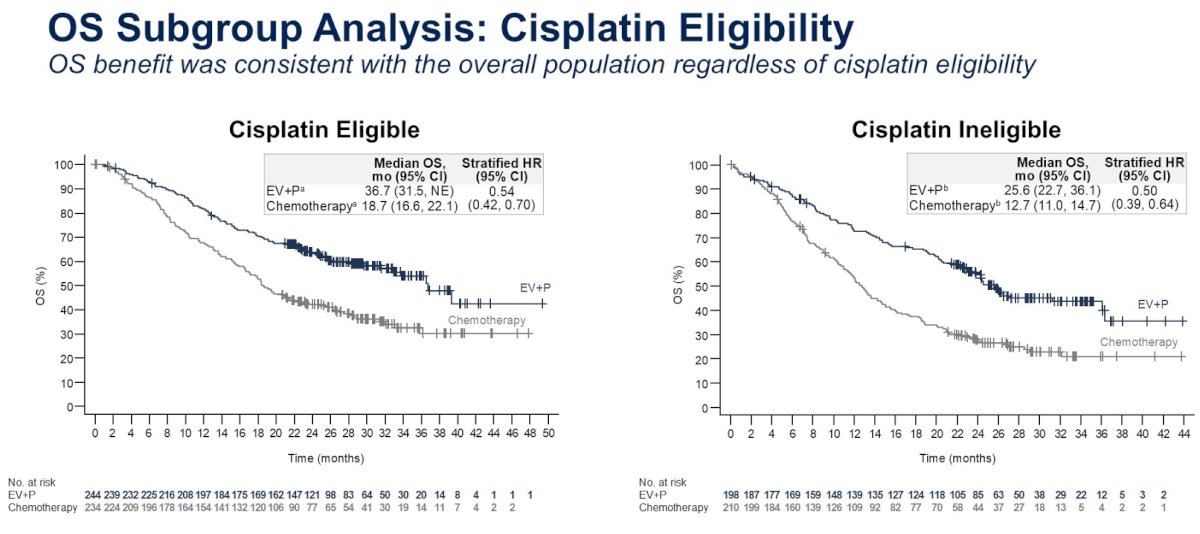
Among responders, the probability of maintaining a response at 1 and 2 years was 67.5% and 50%, respectively. The median duration of response was 23.3 months for EV+P responders, versus 7 months in the chemotherapy arm.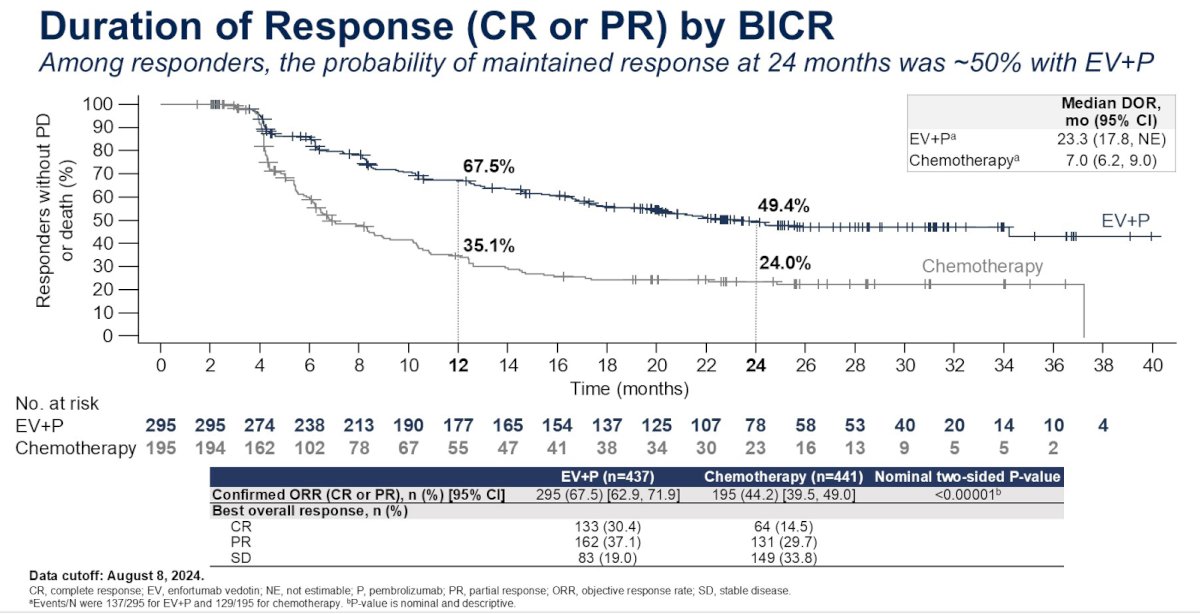
A complete response was observed in 30% of EV+P-treated patients, versus 14.5% of chemotherapy-treated patients. The probability of maintaining a complete response at 2 years with EV+P was 74%. For patients with a confirmed complete response, the 2-year PFS and OS rates were 78% and 95% in the EV+P arm, respectively, versus 54% and 86% in the chemotherapy arm, respectively.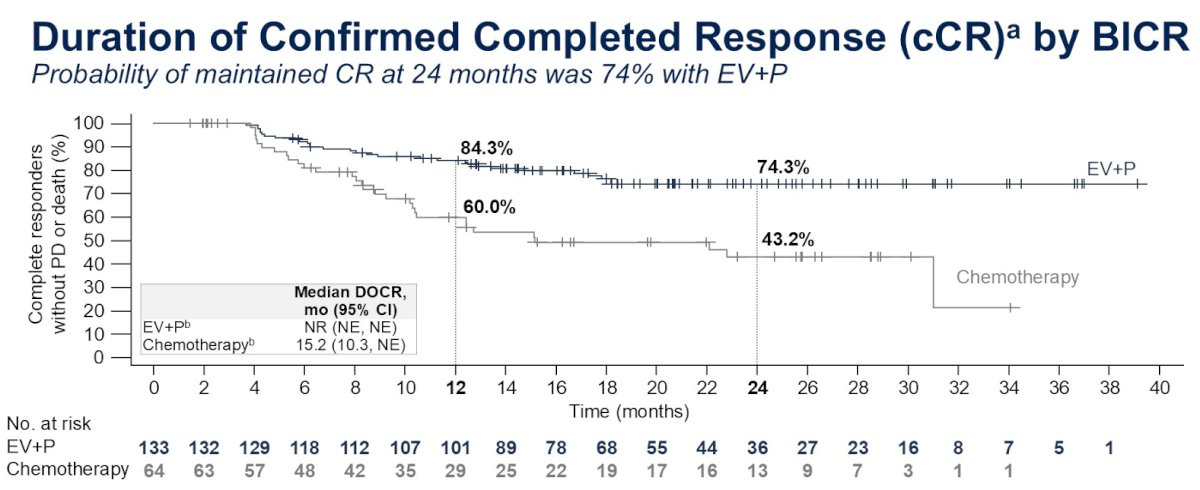
No new safety signals were seen with EV+P after an additional 1 year of follow-up. The frequency and grade of TRAEs remained consistent with the primary analysis. The rates of treatment-emergent AEs of special interest for each of EV and pembrolizumab were consistent with the previously reported primary analysis.1
Dr. Powles concluded as follows:
- After ~2.5 years of median follow-up, the compelling benefit of EV+P was maintained; the median OS with EV+P was more than 2.5 years
- PFS and OS benefit was observed across prespecified subgroups, including the cisplatin-eligible and -ineligible populations
- The response to EV+P was durable, with a median duration of response of nearly 2 years; there was also a 74% probability of remaining in confirmed complete response at 24 months with EV+P
- The frequency and grade of treatment-related AEs and AEs of special interest in the EV+P arm remained consistent with the previously reported primary analysis, with no new safety signals
- These data reinforce EV+P as the SOC for the first-line treatment of patients with la/mUC
Presented by: Thomas Powles, MBBS, MRCP, MD, Professor of Genitourinary Oncology, Director, Barts Cancer Centre at St. Bartholomew's Hospital, London, UK
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
Related content: Enfortumab Vedotin and Pembrolizumab Demonstrate Durable Responses in Advanced Bladder Cancer - Thomas Powles
- Powles T, Valderrama BP, Gupta S, et al. Enfortumab vedotin and pembrolizumab in untreated advanced urothelial carcinoma. N Engl J Med. 2024; 390(10):875-88.