(UroToday.com) The 2025 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Xinan Sheng discussing the phase II RC48-C017 trial assessing neoadjuvant treatment with disitamab vedotin plus perioperative toripalimab in patients with muscle-invasive bladder cancer with HER2 expression.
Cisplatin-based neoadjuvant chemotherapy followed by radical cystectomy is recommended for the cisplatin-eligible patients with muscle invasive bladder cancer. Immunotherapy based neoadjuvant therapy has a significant impact on the treatment of most cancers. For example, the NIAGARA study demonstrated that neoadjuvant durvalumab + chemotherapy significantly improved event free survival and overall survival in operable muscle invasive bladder cancer. There are several clinical trials that combine immunotherapy with antibody drug conjugates in the neoadjuvant setting that are ongoing. However, none of these trials have yet to publish their findings.
HER-2 targeting antibody drug conjugates such as disitamab vedotin and trastuzumab deruxtecan have emerged as effective treatment options for HER2 positive metastatic urothelial carcinoma who failed chemotherapy and immunotherapy. Disitamab vedotin + toripalimab (an anti-PD-1 inhibitor) has shown encouraging efficacy (confirmed objective response rate: 76.3%) in patients with HER-2 expression (IHC 1+, 2+, or 3+) in a phase 1b/2 trial (RC48-C014). RC48-C017 is a single-arm phase II trial conducted to evaluate the efficacy and safety of neoadjuvant disitamab vedotin + perioperative toripalimab in muscle invasive bladder cancer patients with HER2 expression. Presented at the ASCO 2024 annual meeting, the preliminary results showed promising efficacy and acceptable safety with neoadjuvant treatment with disitamab vedotin + toripalimab in patients with HER2-expressing muscle invasive bladder cancer.
Key eligibility criteria included previously untreated muscle invasive bladder cancer (cT2-4aN0-1M0) with HER2 expression (IHC ≥1+ by local test), and eligible for curative-intent radical cystectomy and pelvic lymph node dissection. Patients received disitamab vedotin (2 mg/kg) + toripalimab (3 mg/kg) every 2 weeks for 6 cycles in the neoadjuvant phase. After radical cystectomy and pelvic lymph node dissection, patients received adjuvant toripalimab (3 mg/kg every 2 weeks) for up to 20 cycles: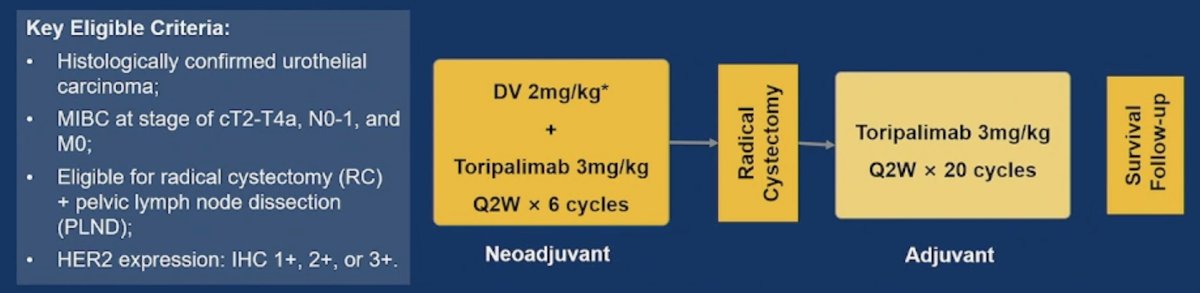
The primary endpoint was pathological complete response (ypT0N0) rate assessed by the investigators, and secondary endpoints included pathological response rate (≤ypT1N0M0), overall survival, and safety. At GU ASCO 2025, Dr. Sheng and colleagues presented the updated efficacy and safety results, as well as a post-hoc event-free survival analysis with a data cutoff date of September 2024.
As of the data cutoff, patient enrollment was completed with 47 patients enrolled and treated, including 10.6% patients with HER2 IHC 1+, 57.4% with HER2 IHC 2+, and 31.9% with HER2 IHC 3+. Overall, 83.0% patients at baseline had T2-4N0M0 disease, and 17.0% had cT2-4aN1M0: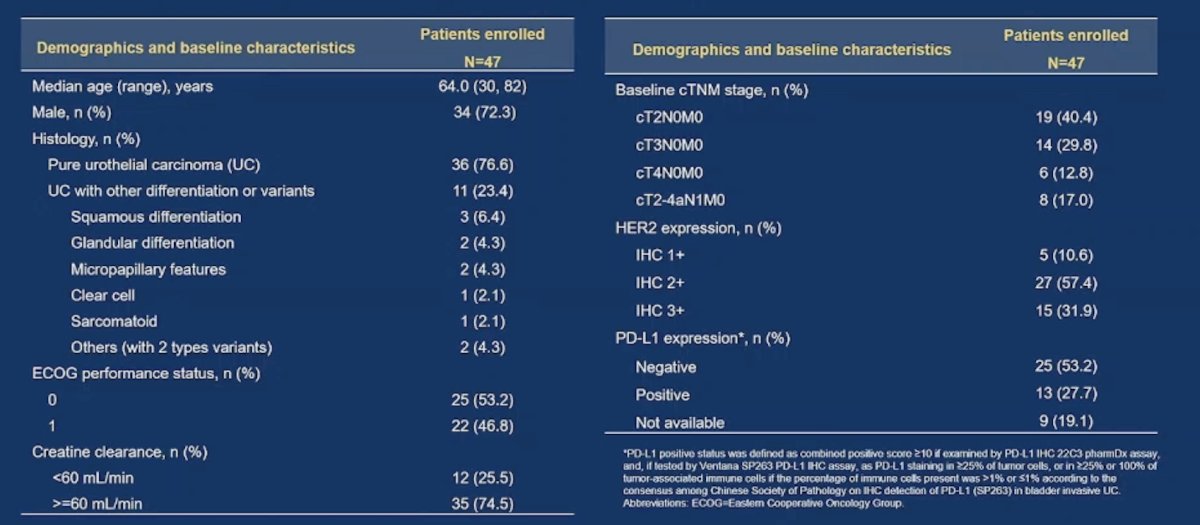
Radical cystectomy and pelvic lymph node dissection was performed in 33 (70.2%) patients, with the following demographics and baseline characteristics: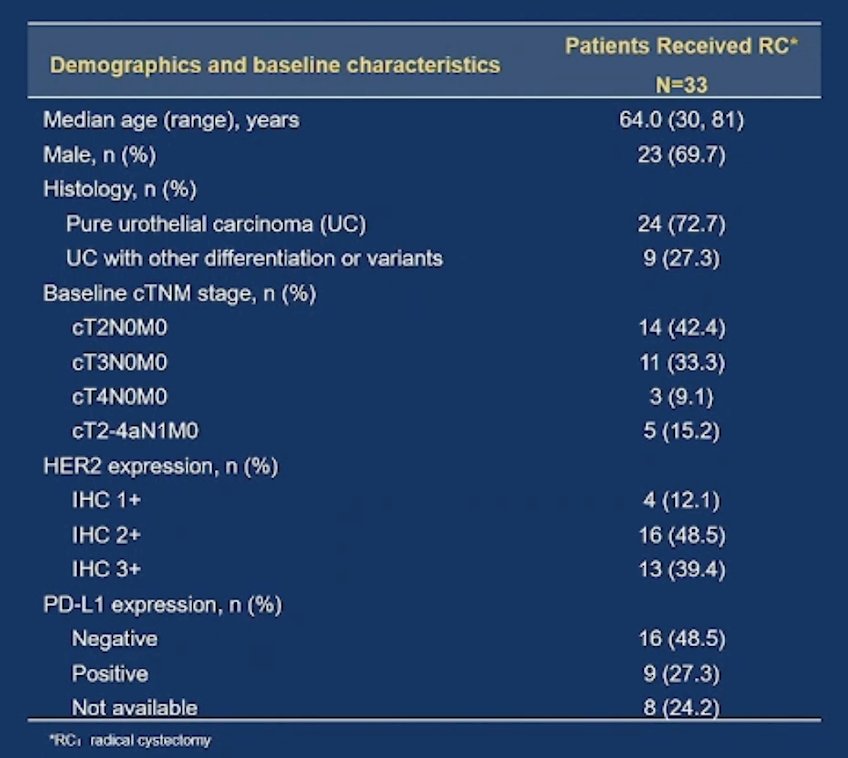
The median time from the end of neoadjuvant treatment to radical cystectomy was 5.0 weeks (range: 2.6-13.1), and the pathological complete response rate was 63.6% (95% CI 45.1%-79.6%), with a pathological response rate of 75.8% (95% CI: 57.7%-88.9%):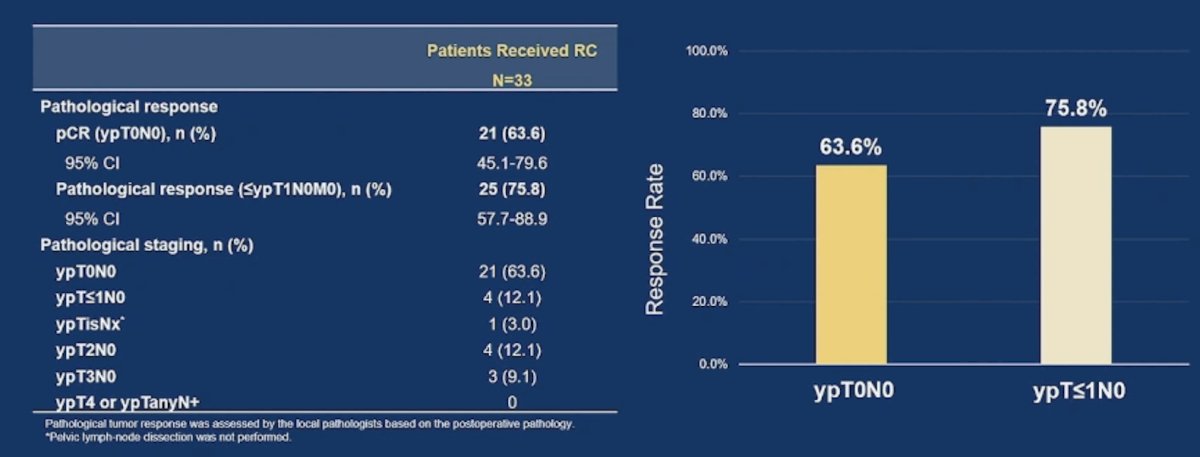
A higher pathological complete response rate of 84.6% was observed in patients with HER2 IHC 3+. The pathological complete response rate for the T2N0 patients appeared to be higher than those for the other subgroups, and rates were generally consistent between patients with pure urothelial carcinoma and patients with urothelial carcinoma with other differentiation or variants:
The 1-year event-free survival rate was 92.5% (95% CI: 72.8%-98.1%) and the 18 month rate was 85.9% (95% CI 60.5%-95.5%):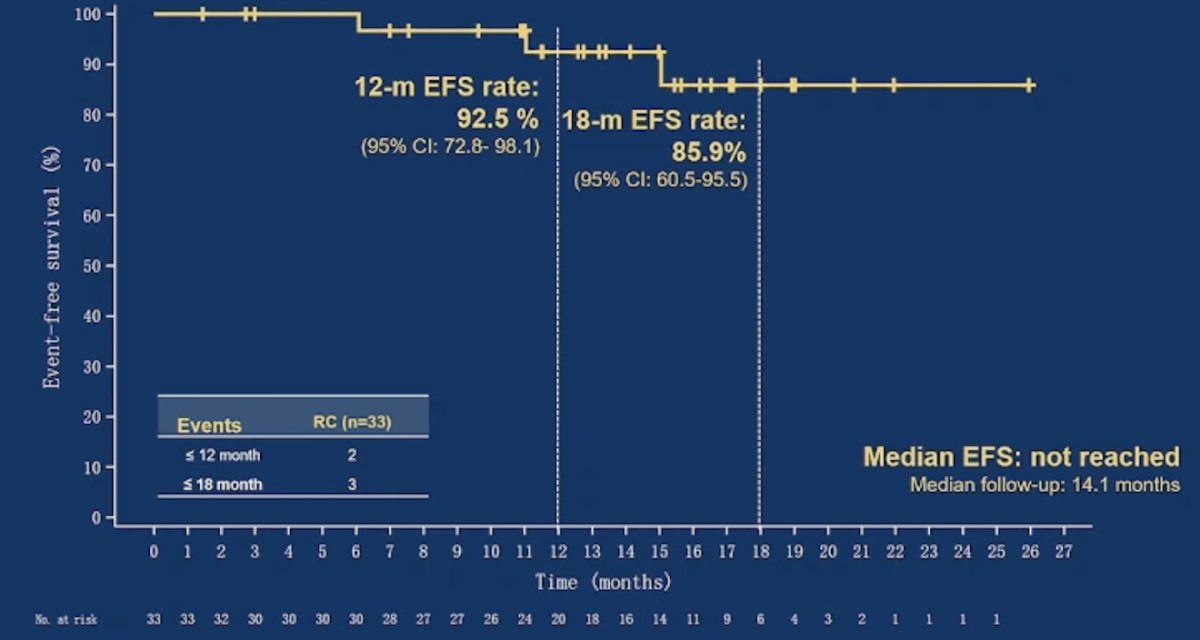
Over a median follow-up of 17.9 months, the median overall survival was not reached, and the 12 month overall survival rate was 95.5% (95% CI 83.3%-98.9%):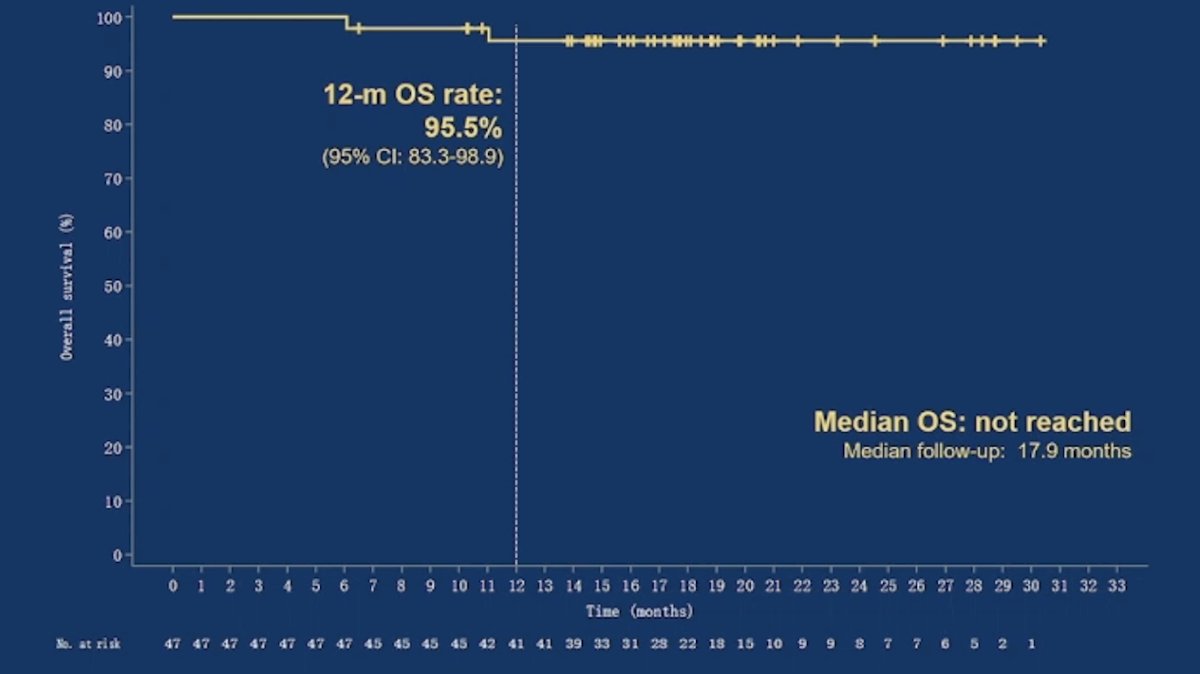
The most common Clavien-Dindo post-operative complication was grade II (15.2%) and the most common type of complication was stoma site infection (15.2%):
In the ITT population, the rate of grade 3+ treatment emergent adverse events was 27.7%, with 17% of patients having an event that led to discontinuation of study treatment:
Dr. Sheng concluded this presentation discussing the phase II RC48-C017 trial assessing neoadjuvant treatment with disitamab vedotin plus perioperative toripalimab in patients with muscle-invasive bladder cancer with HER2 expression with the following take-home points:
- This trial is the first prospective study showing that an antibody drug conjugate in combination with a PD-1 inhibitor as perioperative treatment provided prominent outcomes in operable muscle invasive bladder cancer
- Neoadjuvant disitamab vedotin + toripalimab did not delay radical cystectomy or impact the patient’s ability to undergo surgery. The safety profile was manageable with no new safety signals
- These results indicate that neoadjuvant disitamab vedotin + perioperative toripalimab had promising efficacy and acceptable safety in patients with HER2-expressing muscle invasive bladder cancer, warranting further investigation
Presented by: Xinan Sheng, Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education/Beijing), Department of Genitourinary Oncology, Peking University Cancer Hospital & Institute, Beijing, China
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
Related content: Phase II Trial Results of Disitamab Vedotin and Toripalimab Combination for Muscle-Invasive Bladder Cancer - Xinan Sheng