(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA was host to a urothelial carcinoma poster session. Dr. John Gore presented the results of a real-world study evaluating the clinical characteristics and treatment patterns of muscle invasive bladder cancer (MIBC) patients.
Radical cystectomy remains a standard of care for MIBC, with neoadjuvant cisplatin-based-combination chemotherapy recommended for patients who are eligible for cisplatin.1,2 In the post-cystectomy adjuvant therapy setting post-cystectomy, cisplatin-based-combination chemotherapy is only recommended for patients who do not receive it in the neoadjuvant setting and who have high-risk pathologic features for recurrence after surgery (pT3/4 or positive nodes/margins following resection).1,2 However, the treatment landscape for MIBC is rapidly evolving, with immunotherapy, either as monotherapy or in combination with chemotherapy and/or other targeted agents, being investigated in the neoadjuvant and adjuvant therapy settings.3
This was a non-interventional, retrospective cohort study using data from the Inovalon Insights Payer-Sourced® claims dataset of patients with MIBC who underwent a cystectomy and were followed from the index date (first day of cystectomy or neoadjuvant systemic therapy) until the end of the study, loss of follow-up, diagnosis of metastasis, or end of enrollment in their medical or pharmacy health plan, whichever occurred first.
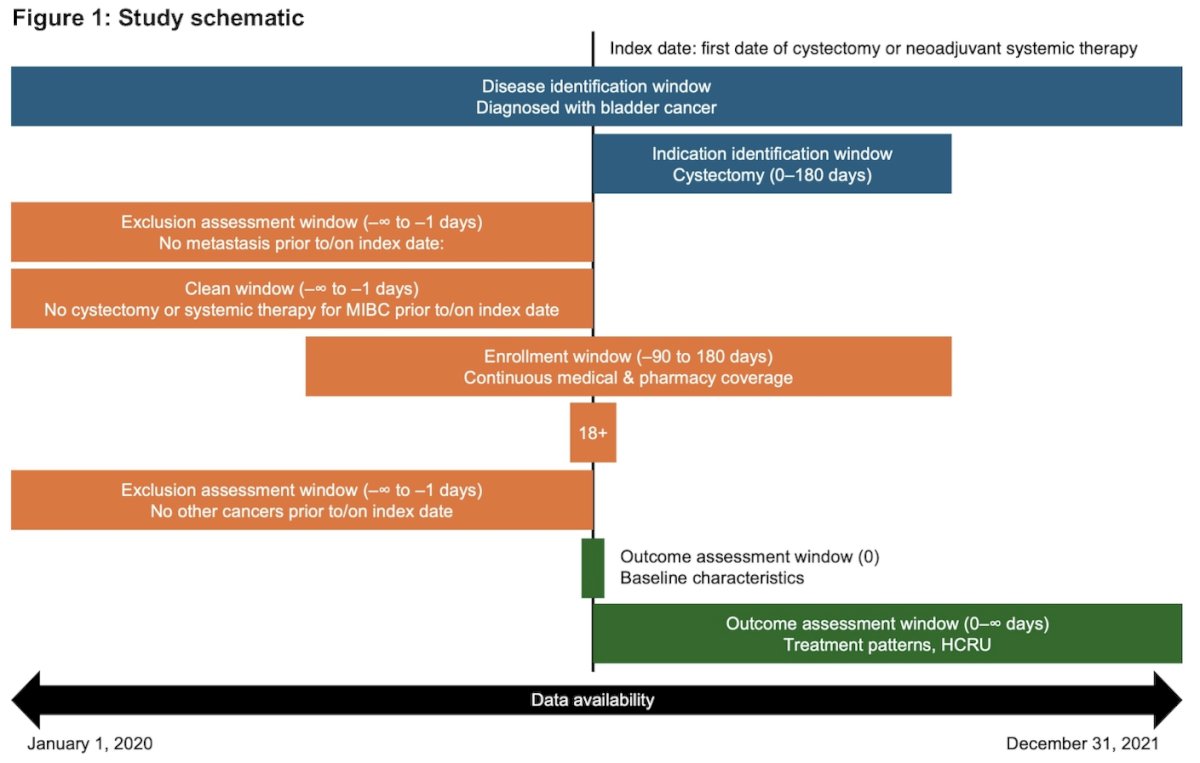
Data were extracted from January 1, 2020, to December 31, 2021. A modified version of a previously published algorithm was used to identify patients with MIBC who were stratified by entry therapy:
- Neoadjuvant therapy: patients indexed on neoadjuvant systemic therapy with a claim for a cystectomy within 6 months
- No neoadjuvant therapy: patients indexed on cystectomy with no prior systemic therapy for MIBC
The following study definitions were employed:
- Adjuvant systemic therapy was defined as systemic therapy that was initiated within 3 months of cystectomy without a gap of ≥60 days between the chemotherapy cycles.
- First subsequent therapy was defined as the first systemic therapy initiated after completion of adjuvant therapy or initiated >3 months post-cystectomy.
- Patients were considered to receive the next treatment if they added any new systemic agent that was not used within the first 45-day period of the existing treatment regimen or if they re-initiated the same systemic therapy after a 60-day gap from the end of the prior treatment regimen.
Results are presented for the entire study sample and for patients who received neoadjuvant and/or adjuvant therapy by treatment type.
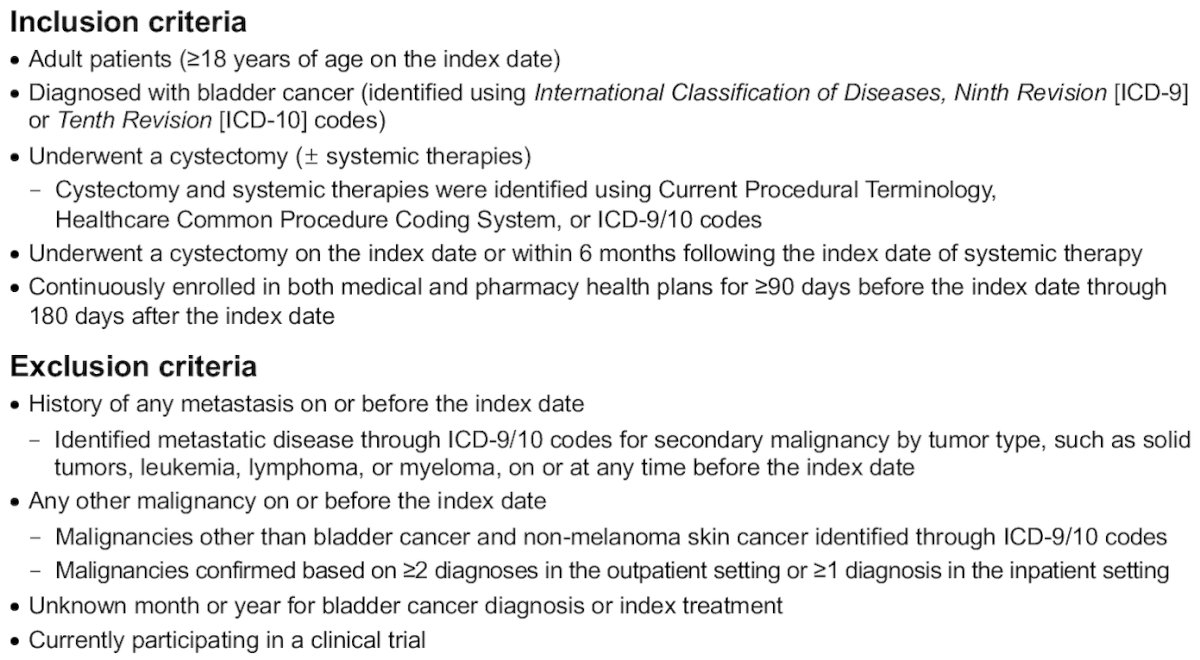
The inclusion and exclusion criteria are summarized below:
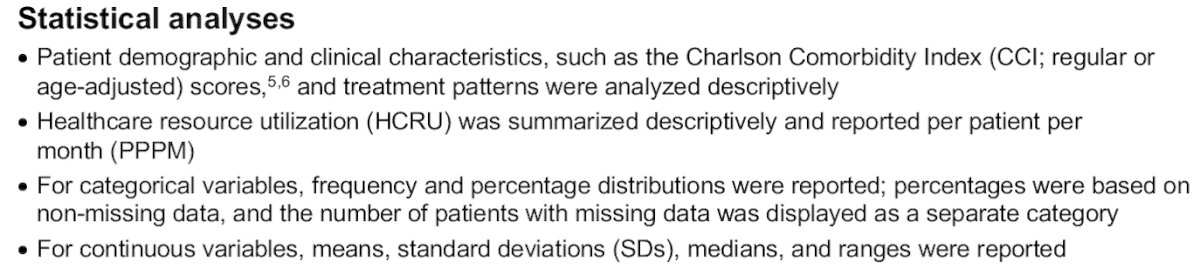
The statistical analytical plan is summarized below:
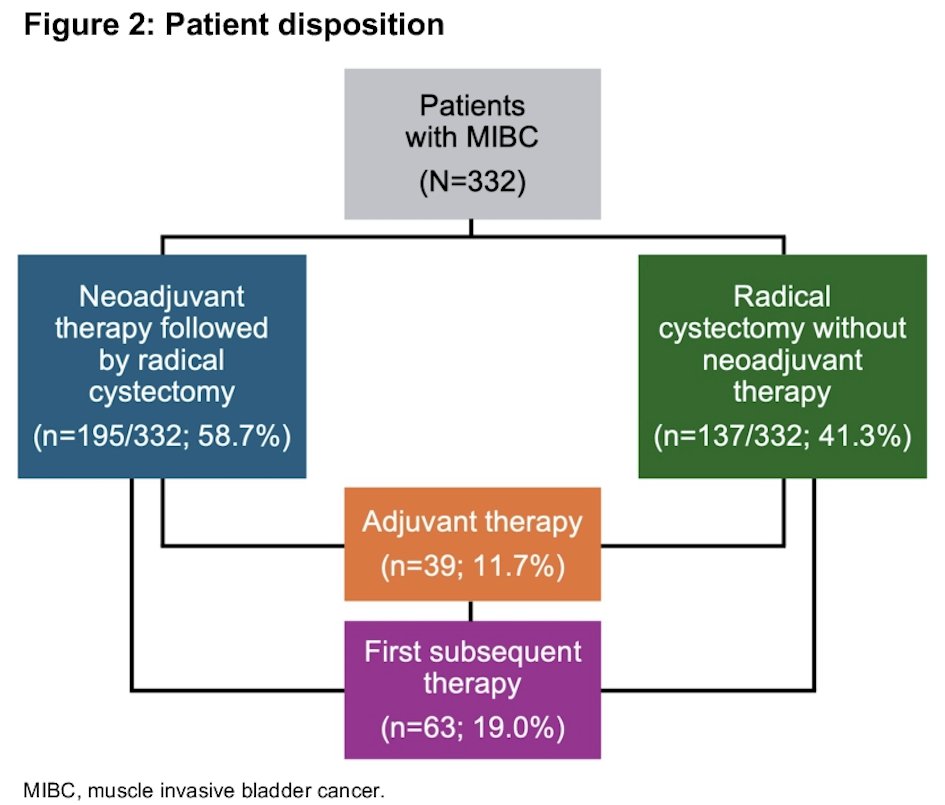
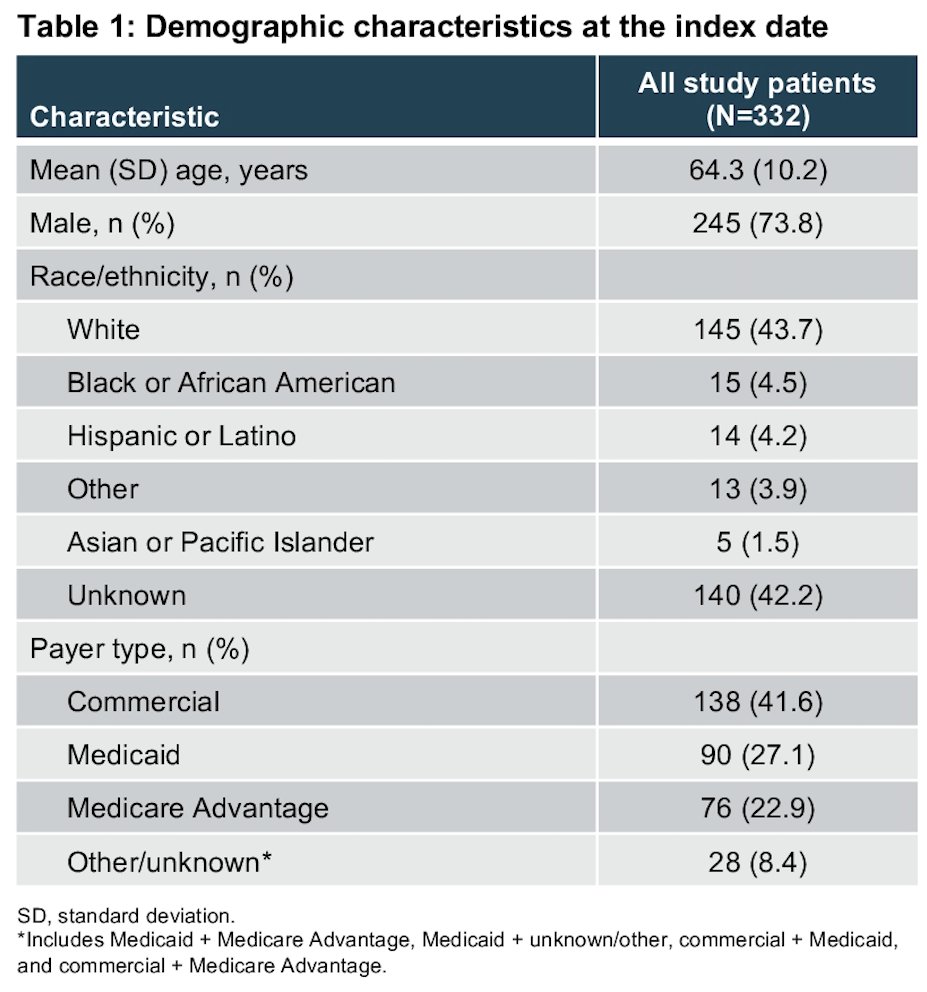
332 patients met the study eligibility criteria, of which 41.3% entered the cohort via cystectomy, and 58.7% entered via neoadjuvant therapy.
Among the 332 study patients, the mean age was 64.3 years, 74% were male, and 44% were White. The mean age-adjusted CCI score was 6.3. Common comorbidities reported were:
- Hypertension (60%)
- Urinary tract infection (28%)
- Diabetes without chronic complications (26.5%)

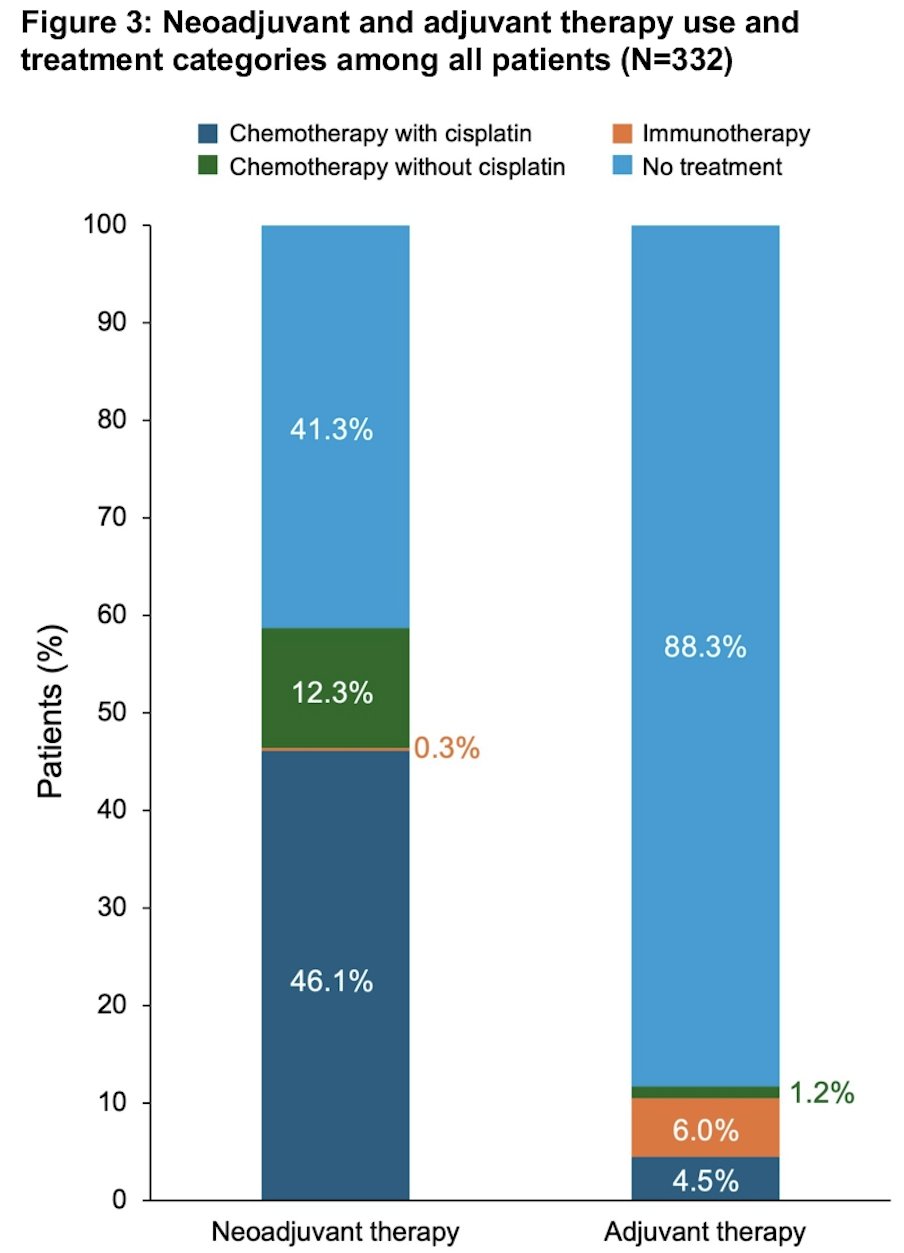
A large proportion of patients (41%) did not receive neoadjuvant therapy. Among the 195/332 (59%) patients who received neoadjuvant therapy, 153/195 (78.5%) received chemotherapy with cisplatin. The most common regimens were:
- Cisplatin + gemcitabine (76/195; 39%)
- Cisplatin + doxorubicin + methotrexate + vinblastine (56/195; 29%)
41/195 (21%) patients received chemotherapy without cisplatin. The most common agents were mitomycin (17/195; 8.7%) and gemcitabine (14/195; 7.2%). One patient (0.5%) received immunotherapy (pembrolizumab).
Most patients (88%) did not receive adjuvant therapy. Among the 39/332 (12%) patients who received adjuvant therapy, 51% (20/39) received immunotherapy. The most common treatment was nivolumab (10/39; 26%). All of these patients received neoadjuvant therapy. 15/39 (38.5%) patients received chemotherapy with cisplatin. The most common regimen was cisplatin + gemcitabine (n=10/39; 25.6%). Seven of these patients received neoadjuvant therapy. 4/39 (10%) patients received chemotherapy without cisplatin. The most common treatment was carboplatin (2/39; 5%). None of these patients received neoadjuvant therapy.
The rate of adjuvant therapy use was similar between patients with and without neoadjuvant therapy (14% and 9%. respectively).
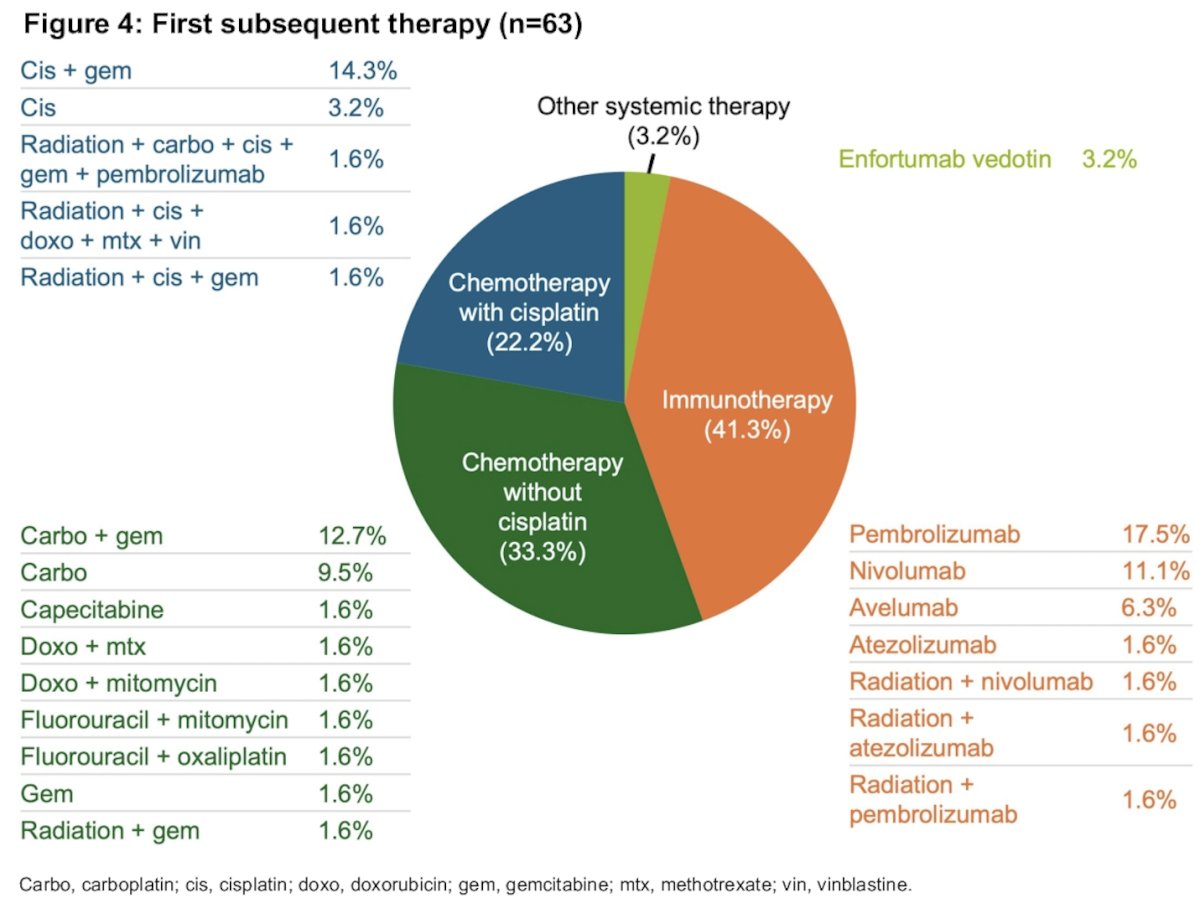
A total of 63/332 (19%) patients received a first subsequent therapy. Of the 63 patients, 26 (41%) patients received immunotherapy. The most common agent was pembrolizumab (11/63; 17.5%).
21/63 (33.3%) patients received chemotherapy without cisplatin. The most common regimen was carboplatin + gemcitabine (8/63; 13%). 14/63 (22%) patients received chemotherapy with cisplatin. The most common regimen was cisplatin + gemcitabine (n=9/63; 14%). 2/63 (3.2%) patients received other systemic therapy.
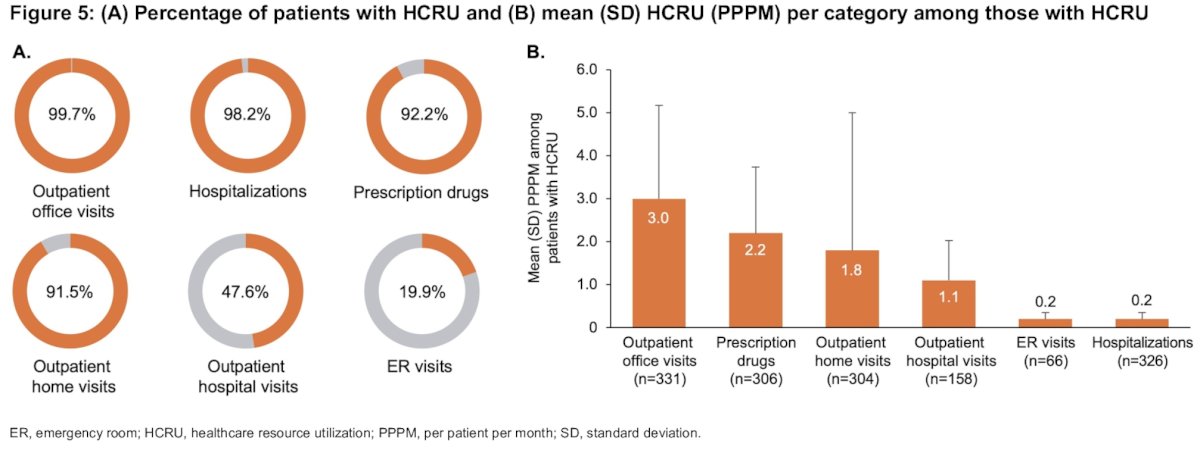
Among patients with healthcare resource utilization. the most common setting of care for patients was outpatient office visits (99.7% of patients) followed by hospitalizations (98.2% of patients). The highest intensity of utilization was for outpatient office visits (mean per patient per month: 3.0) followed by prescription drugs (mean: 2.2).
Dr. Gore noted that study limitations included the following:
- Patients were identified using a modified version of a published algorithm and not a single specific ICD code
- This algorithm does not reflect treatment patterns/healthcare resource utilization for patients who chose to pursue a bladder-sparing approach
- Claims record diagnostic and procedure codes for reimbursement purposes and may be subject to coding errors, or data omission
- Claims data do not provide direct information on disease severity/progression, or cisplatin eligibility
- Because the time period of this study was from January 1, 2020, to December 31, 2021, the availability of data on the utilization of nivolumab. which was approved to treat MIBC by the US Food and Drug Administration in August 2021 may have been limited
Dr. Gore concluded as follows:
- The majority of patients with MIBC were older, male, White, and had ≥3 comorbidities
- Many patients underwent radical cystectomy without neoadjuvant or adjuvant therapy
- In the neoadjuvant therapy setting, 78.5% of patients received cisplatin-based therapy, most commonly cisplatin + gemcitabine
- Among patients who received adjuvant therapy, the most commonly used treatment was immunotherapy followed by chemotherapy with cisplatin
- For the first subsequent therapy after the adjuvant therapy period, the most commonly used class was immunotherapy, with pembrolizumab being the most common treatment
- The most common setting of health care resource utilization for patients was outpatient office visits followed by hospitalizations
- The highest intensity of use per month (per patient per month; PPPM) was for outpatient office visits followed by prescription drugs
- Further evaluation of treatment patterns is needed as the landscape evolves
Presented by: John Gore, MD, MS, Professor, Department of Urology, University of Washington, Seattle, WA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:
- Witjes JA, Bruins HM, Carrion A, et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2023 Guidelines. Eur Urol. 2024; 85(1):17-31.
- Holzbeierlein JM, Bixler BR, Buckley DI, et al. Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer: AUA/SUO Guideline: 2024 Amendment. J Urol. 2024; 211(4):533-8.
- Lopez-Beltran A, Cookson MS, Guercio BJ, Cheng L. Advances in diagnosis and treatment of bladder cancer. BMJ. 2024; 384:076743.