(UroToday.com) The 2026 ASCO annual meeting featured a bladder cancer rapid abstract session and a presentation by Dr. Emanuele Crupi discussing a phase II study of frontline gemcitabine, 5-fluorouracil/leucovorin, and cisplatin in advanced urachal and non-urachal urinary tract adenocarcinoma. Urinary tract adenocarcinoma is a very rare disease with no standard of care for frontline therapy in the advanced setting. Evidence has largely been retrospective, although fluropyrimidine-based regimens have shown activity. More recently, the ULTIMA trial reported promising prospective activity of modified FOLFIRINOX in advanced urachal cancer.
This was a prospective, single-arm, phase II study (NCT00082706) conducted at MD Anderson Cancer Center. Between 2005 and 2010, patients aged ≥18 years with ECOG performance status 0–2 and metastatic or unresectable urachal or non-urachal adenocarcinoma received frontline GemFLP (5-fluorouracil 200 mg/m² continuous infusion × 5 days with leucovorin 23 mg IV daily × 5; cisplatin 20 mg/m² IV daily × 5; gemcitabine 200 mg/m² IV on days 1 and 5):
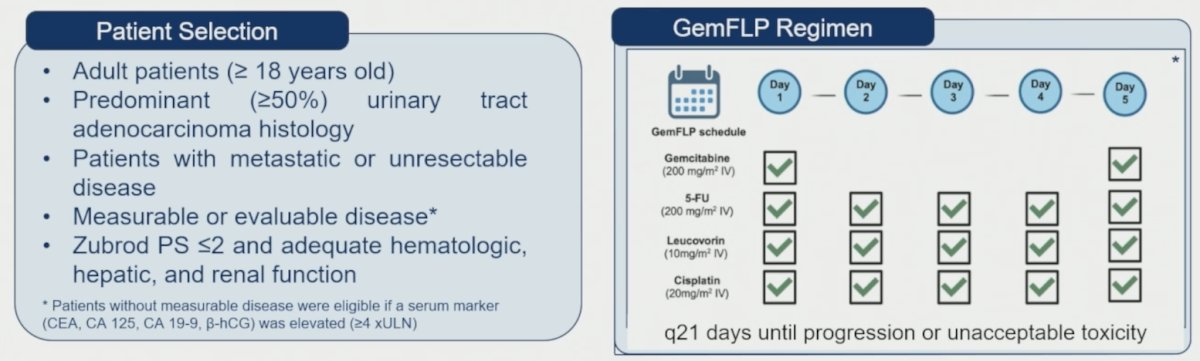
The best overall response was assessed by imaging. The primary endpoints were objective response rate and overall survival, and the secondary endpoint was toxicity. Progression-free survival was calculated from treatment initiation and duration of response from first complete response/partial response to progression or death, and time to event endpoints were estimated by Kaplan-Meier. Post hoc analyses evaluated baseline tumor markers (CEA, CA19-9, CA125, β-hCG), and treatment-related adverse events were graded per CTCAE v5.
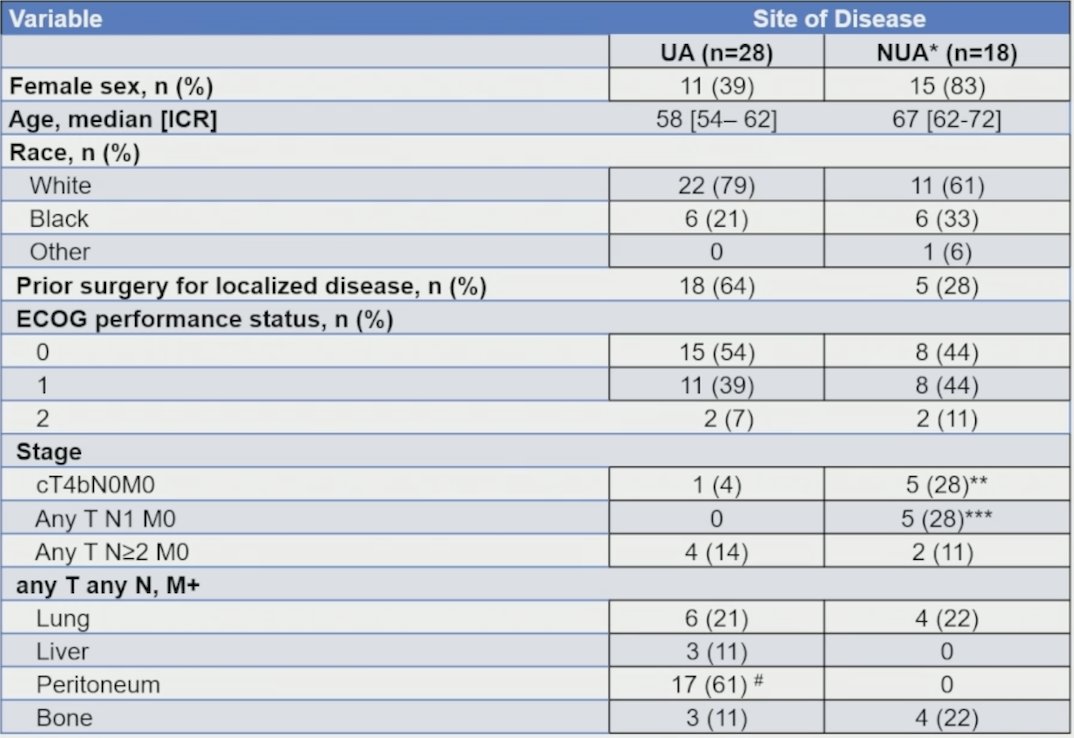
There were 46 patients enrolled (28 unresectable urachal, 18 non-urachal adenocarcinoma). Among patients with non-urachal adenocarcinoma, 9/18 (50%) had tumors originating from the urethra. The median age was 58 years, 41% were de novo metastatic, and 78% had visceral metastases:
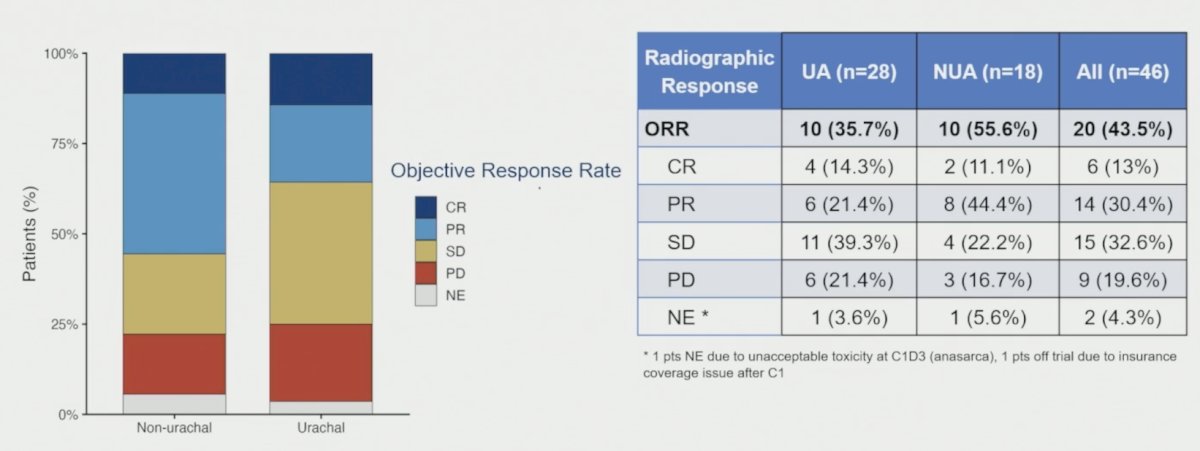
The objective response rate was 44% (20/46), and among responders, the median duration of response was 8.6 months (95% CI 4.6–30.8). There were 6 (13%) of patients who had a complete response, and 14 (30.4%) of patients who had a partial response:
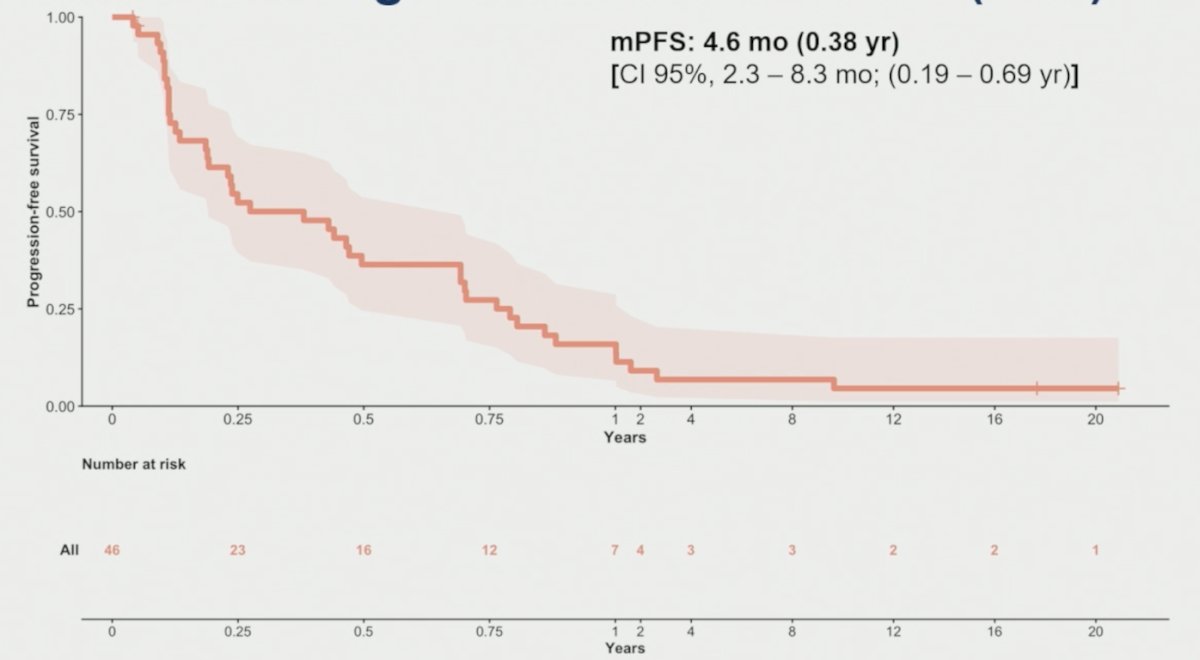
The median progression-free survival was 4.6 months (95% CI 2.3–8.3):
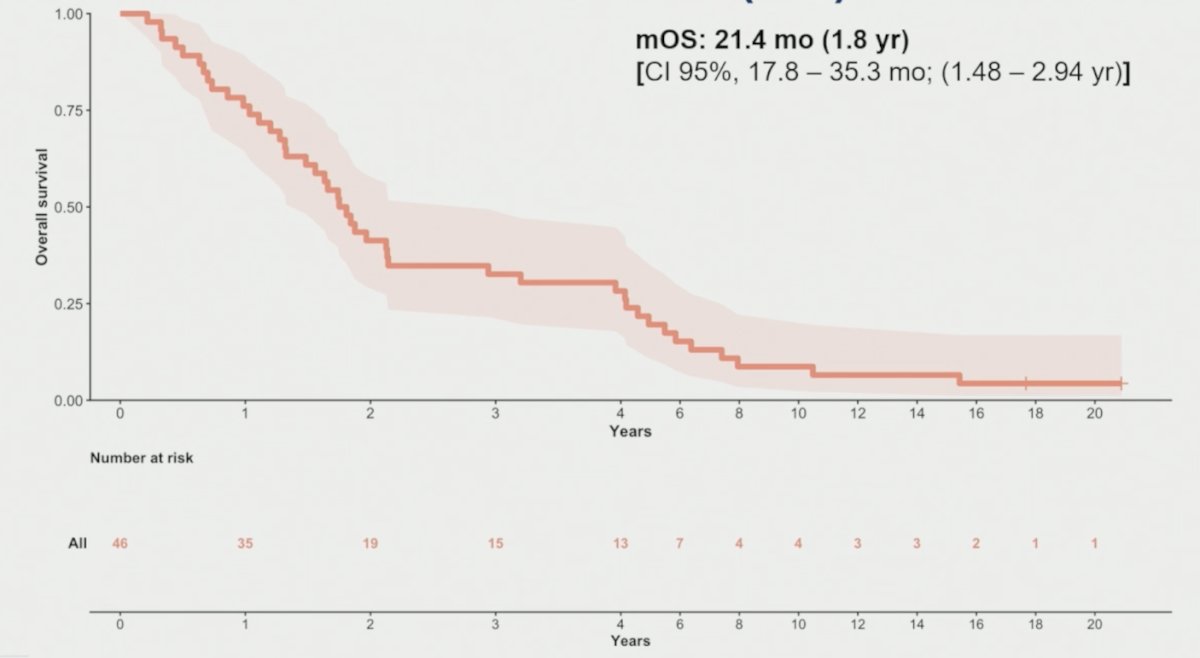
The median overall survival was 21.4 months (95% CI 17.8–35.3):
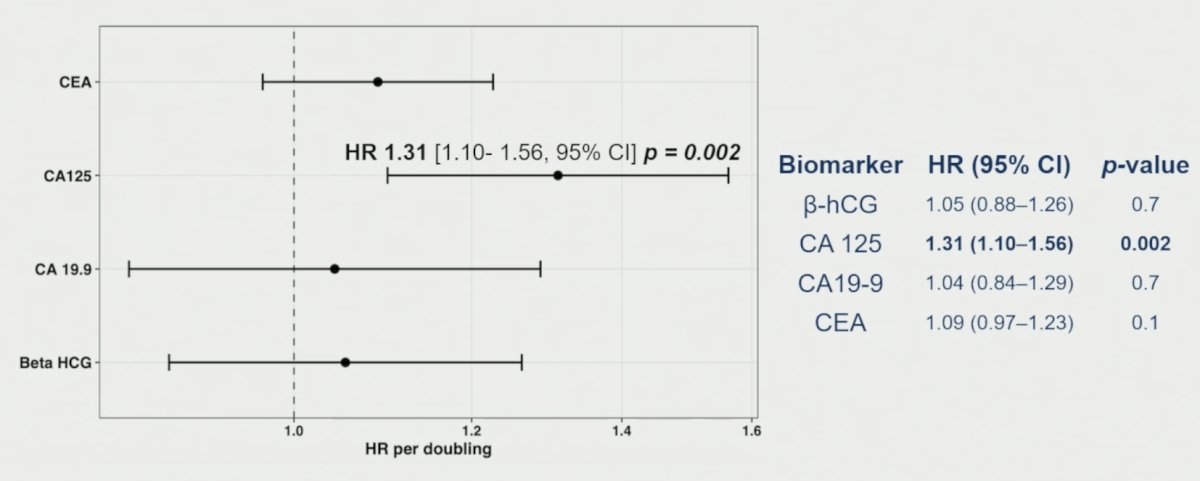
There was no difference in progression-free survival (p = 0.39) or overall survival (p = 0.99) between unresectable urachal and non-urachal adenocarcinoma. Baseline CEA, CA19-9, CA125, and β-hCG were not associated with objective response rate or progression-free survival. However, higher baseline CA125 was associated with inferior overall survival (HR 1.31, 95% CI 1.10–1.56; p = 0.002):
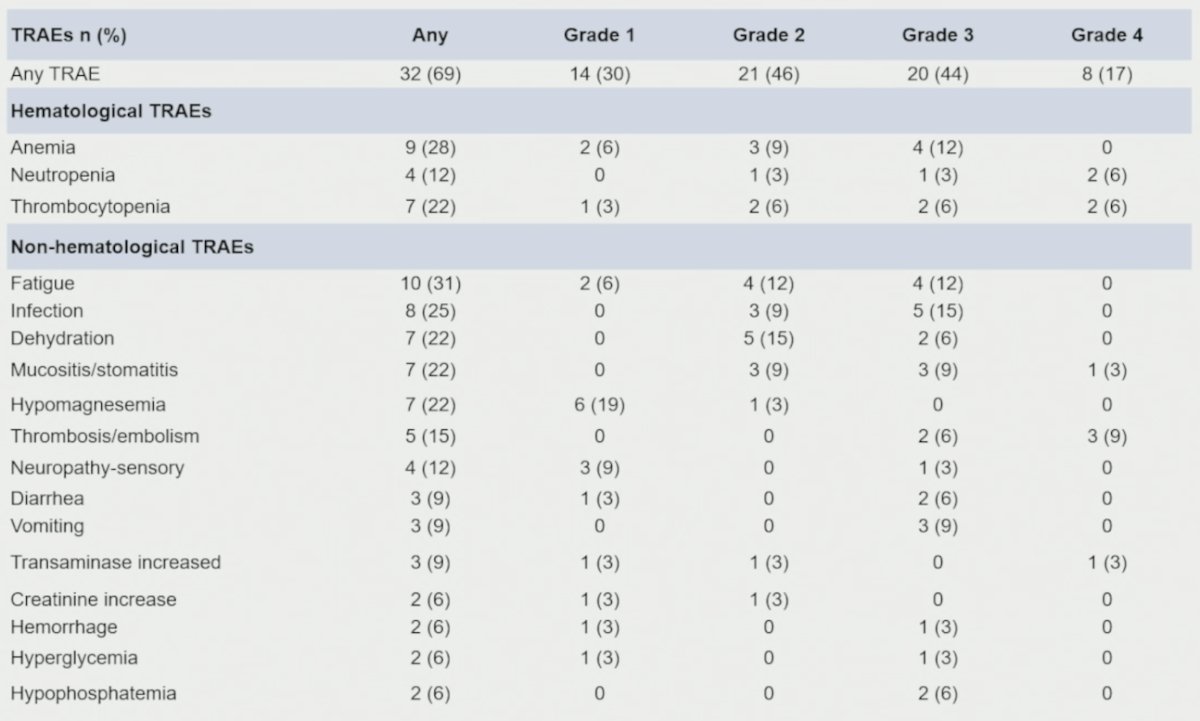
Subsequent systemic therapy was administered to 28 patients (60.9%), and the median number of subsequent treatment lines was 2 (range 1–5). The most common hematologic treatment-related adverse events were anemia (28.1%; grade ≥3 12.5%), thrombocytopenia (21.9%; grade ≥3 12.5%), and neutropenia (12.5%; grade ≥3 9.4%). The most frequent non-hematologic treatment-related adverse events were dehydration (21.9%; grade ≥3 6.2%), diarrhea (9.4%; grade ≥3 6.2%), and catheter-related thrombosis (9.4%; grade ≥3 9.4%). No grade 5 events occurred:
There were several limitations from this trial, including (i) the single-arm design, (ii) the small sample size (n = 46), but in an inherently rare disease, limiting subgroup analyses, and (iii) biomarker analyses were exploratory and require independent validation.
Dr. Crupi concluded this presentation discussing a phase II study of frontline GemFLP in advanced urachal and non-urachal urinary tract adenocarcinoma with the following take-home points:
- GemFLP achieved a 44% objective response rate and 21.4-month median overall survival in advanced urachal and non-urachal urinary tract adenocarcinoma
- GemFLP was safe and manageable, with no grade 5 events; the main toxicities were anemia, dehydration, thrombocytopenia, and neutropenia
- Baseline CA 125 was associated with worse overall survival, but this finding requires validation in larger independent prospective cohorts
- Clinical Implication: In the absence of a standard of care, GemFLP provides a prospective reference regimen for future studies and a reasonable current option in appropriately selected patients
Presented by: Emanuele Crupi, MD, The University of Texas MD Anderson Cancer Center, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026