(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL, was host to the Prostate, Testicular, and Penile Cancer - Oral Abstracts. Dr. Lucia Nappi presented Abstract LBA5003: First Interim Analysis of SWOG S1823/GCC.1: Operating Characteristics of Circulating microRNA 371a-3p (miR371) in Predicting Active Germ Cell Malignancy (aGCM) in Patients (pts) With Early-Stage Testicular Cancer.
Dr. Nappi began by highlighting that germ cell tumors represent the most common solid malignancy affecting young men, with clinical stage I (CSI) disease representing the most frequent presentation following orchiectomy. She noted that active surveillance remains the most commonly utilized management strategy for these patients, allowing avoidance of overtreatment while maintaining excellent oncologic outcomes. However, this approach requires intensive longitudinal monitoring with serial CT imaging and serum tumor marker assessment, including β-HCG, LDH, and AFP. Dr. Nappi emphasized that despite being considered the current standard of care, existing surveillance tools remain imperfect, particularly for the early detection of relapse.
She subsequently reviewed the limitations of current surveillance strategies, highlighting that CT imaging demonstrates limited diagnostic accuracy for retroperitoneal lymph nodes smaller than 2 cm and may be particularly challenging in seminoma. Similarly, conventional serum tumor markers exhibit suboptimal performance characteristics, with reported specificity ranging from 50-60% and sensitivity varying between 15-60%. She also emphasized the cumulative radiation exposure associated with repeated CT imaging in this typically young patient population undergoing prolonged surveillance schedules. In contrast, Dr. Nappi discussed miR371 as a highly promising biomarker that is highly specific for non-teratoma germ cell tumors and demonstrates strong expression in peripheral blood. Retrospective studies have consistently demonstrated excellent diagnostic performance, with an area under the curve exceeding 0.90, while requiring only small plasma or serum volumes ranging from 50-400 μL. She concluded that prospective validation studies evaluating miR371 in early-stage germ cell tumors are critically needed to reduce reliance on serial imaging and improve relapse detection during active surveillance.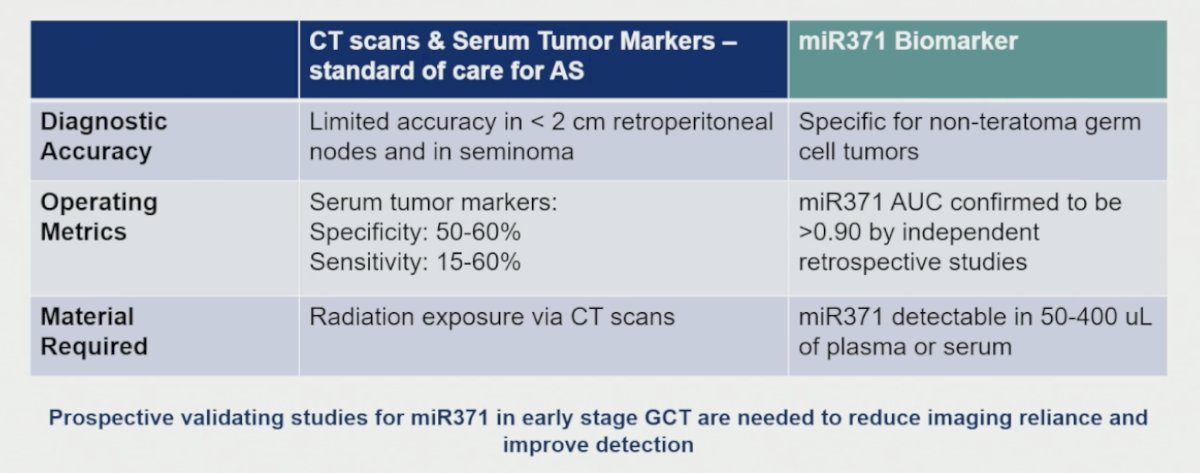
Dr. Nappi subsequently reviewed the design of the SWOG S1823/GCC.1 study, a collaborative effort conducted through SWOG and the Canadian Cancer Trials Group, evaluating the clinical utility of miR371 in patients with germ cell tumors managed with active surveillance. Eligible patients were enrolled within 56 days of orchiectomy, underwent consent and registration procedures, and provided baseline blood specimens prior to assignment into risk cohorts based on their estimated pre-test probability of relapse. The primary endpoint of the study was to evaluate the operating characteristics of miR371 at the time of clinical relapse diagnosis among patients with CSI and CSIIA disease undergoing active surveillance within the low- and moderate-risk cohorts. The study design is shown below.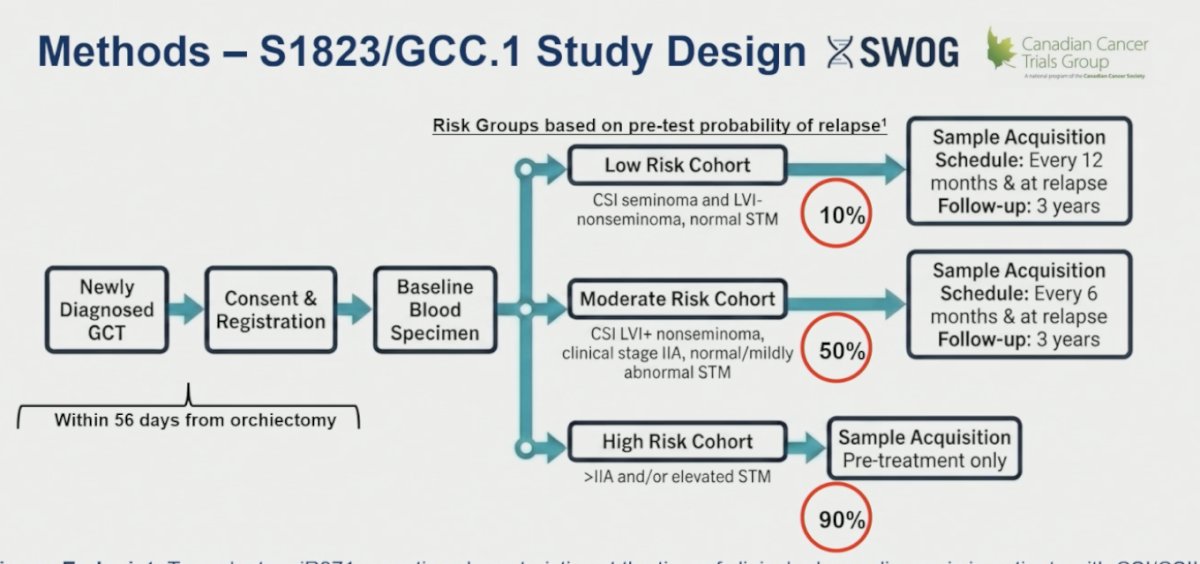
Dr. Nappi highlighted that patients with CSI seminoma and LVI-negative nonseminoma with normal serum tumor markers were categorized into the low-risk cohort, which carried an estimated relapse risk of approximately 10%. These patients underwent blood sample acquisition every 12 months and at relapse, with planned follow-up for 3 years. The moderate-risk cohort included patients with CSI LVI-positive nonseminoma, CSIIA disease, or mildly abnormal serum tumor markers, corresponding to an estimated relapse risk of approximately 50%. In this group, blood samples were obtained every 6 months and at relapse, also with 3 years of follow-up. Lastly, the high-risk cohort included patients with stage >IIA disease and/or elevated serum tumor markers, with an estimated relapse risk approaching 90%; however, these patients underwent only pre-treatment sample acquisition and did not contribute to the primary endpoint analysis of the study.
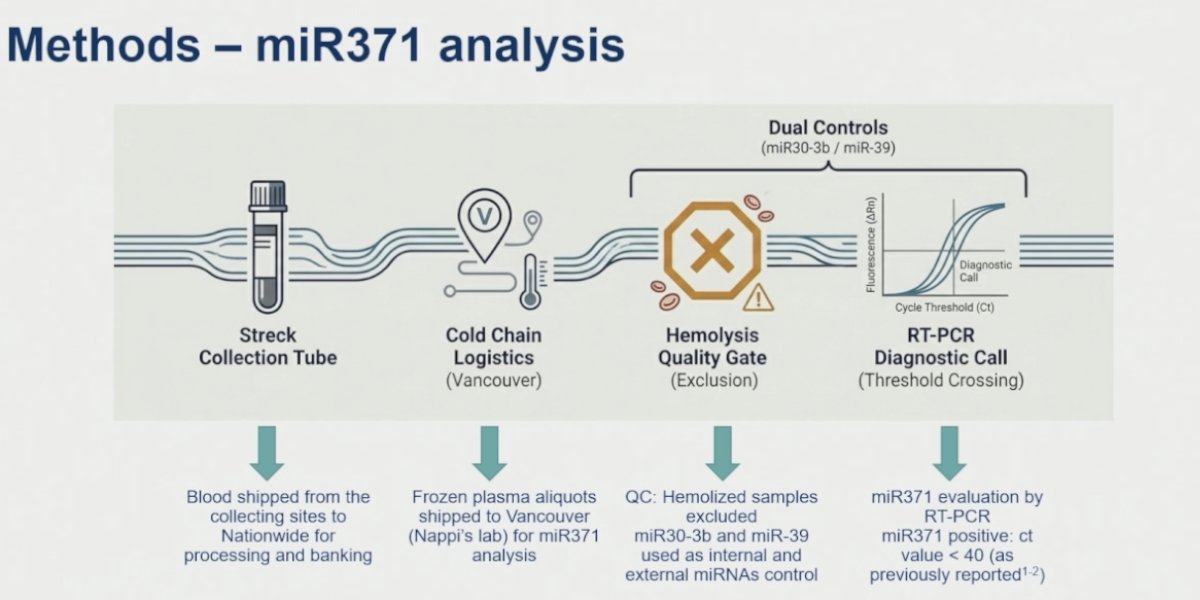
For miR371 analysis, blood samples were collected using Streck collection tubes at participating sites nationwide and subsequently processed and banked prior to shipment. Frozen plasma aliquots were then shipped under controlled cold-chain logistics to Dr. Nappi’s laboratory in Vancouver for centralized miR371 analysis. Quality control procedures included exclusion of hemolyzed samples, while miR30-3b and miR39 were used as internal and external miRNA controls. Dr. Nappi noted that miR371 expression was evaluated using RT-PCR, with results interpreted qualitatively as positive or negative based on a predefined cycle threshold cutoff value of <40, consistent with previously published studies.
Dr. Nappi noted that the statistical design for the primary endpoint focused specifically on patients with CSI and CSIIA disease managed with active surveillance, with the study targeting a total of 150 relapse events, including 100 relapses in patients with nonseminoma and 50 in seminoma. The planned enrollment included approximately 806 patients overall, including 333 patients with seminoma and 400 with nonseminoma. She explained that the current analysis represented the first planned interim analysis, which was initially designed as a futility assessment after the occurrence of 80 relapse events, evenly distributed between seminoma and nonseminoma cohorts. Cases and controls were matched in a 2:1 fashion according to histology and risk group, and specimens collected closest to the time of relapse were selected for analysis. Importantly, all clinical relapse events underwent blinded validation through principal investigator record review prior to miR371 biomarker analysis.
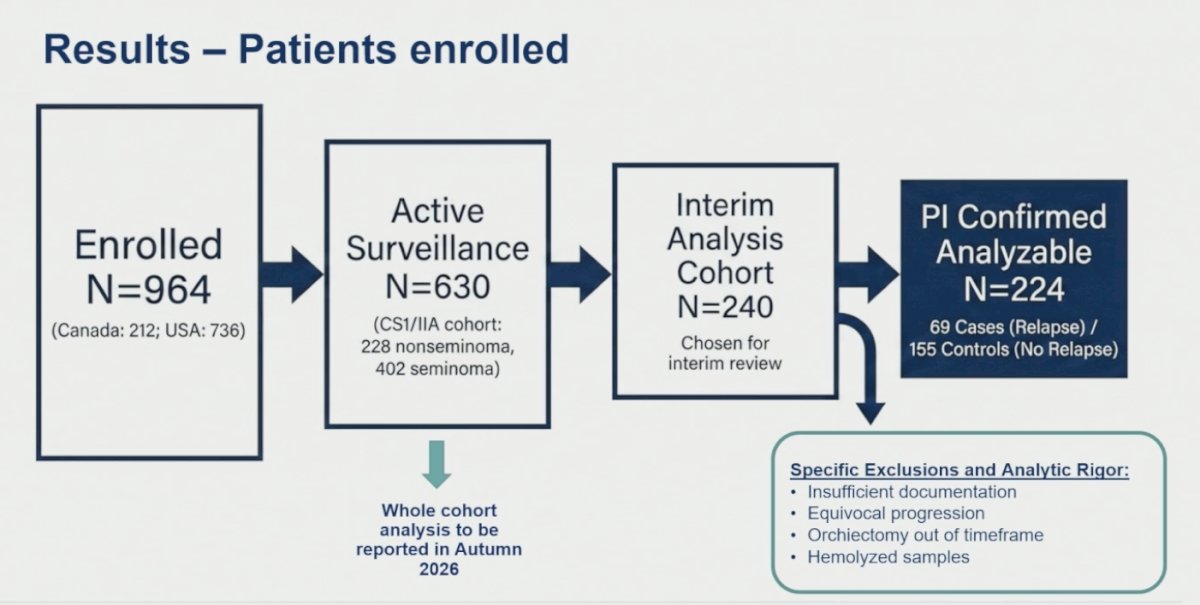
Dr. Nappi noted that the study enrolled a total of 964 patients across participating centers in Canada and the United States. Among these, 630 patients with CSI or CSIIA disease were managed with active surveillance and comprised the primary surveillance cohort, including 228 patients with nonseminoma and 402 with seminoma. For the current interim analysis, 240 patients were selected for review, ultimately resulting in 224 principal investigator-confirmed analyzable cases after exclusion of patients with insufficient documentation, equivocal progression events, orchiectomy outside the predefined timeframe, or hemolyzed samples. The final interim cohort included 69 relapse cases and 155 matched controls without relapse.
The overall relapse rate of the overall cohort was 14.63% following orchiectomy. Median time to relapse was 5.8 months overall, occurring somewhat earlier in patients with nonseminoma compared with seminoma (5.3 vs 7.4 months, respectively). Relapse timing also differed according to risk group, with moderate-risk patients relapsing earlier than low-risk patients, with median times to relapse of 4.1 and 6.6 months, respectively. Cumulative incidence analyses further demonstrated substantially higher relapse rates among moderate-risk patients, reaching 24% at 6 months, 33.3% at 12 months, and 34.7% at 24 months, compared with corresponding relapse rates of 4%, 9.1%, and 12% in the low-risk cohort.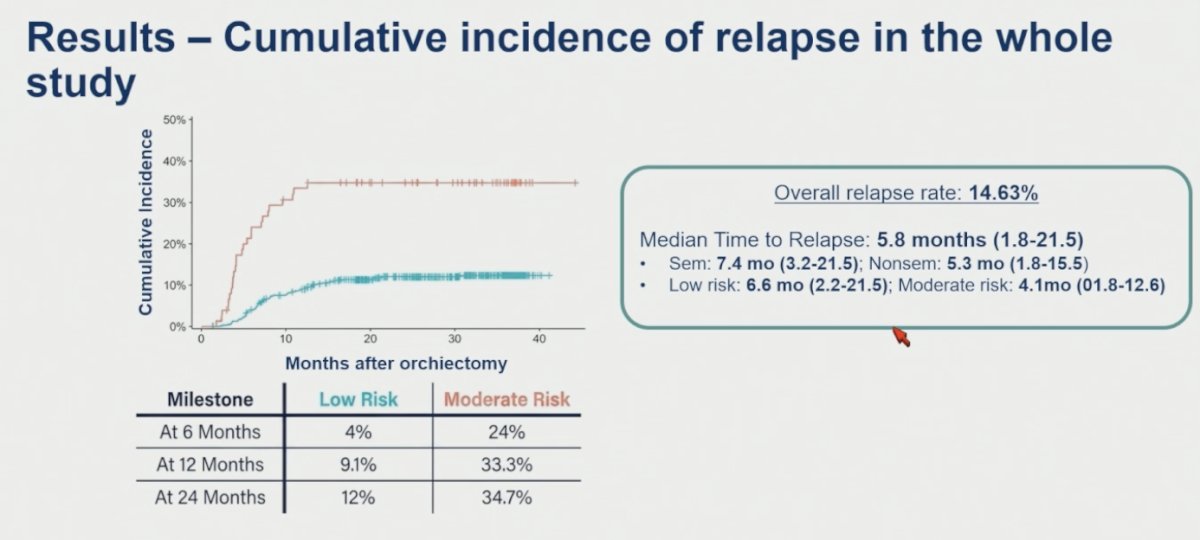
Baseline patient characteristics demonstrated that the majority of relapse cases occurred within the low-risk cohort, which accounted for 70% of relapse events, while 30% occurred among moderate-risk patients. Histologic distribution was balanced between seminoma and nonseminoma across cases and controls, and nearly all patients had stage I disease at registration. Dr. Nappi also highlighted that the median follow-up among controls was 35.1 months, notably exceeding the observed median time to relapse, supporting the adequacy of surveillance duration and event capture within the study cohort.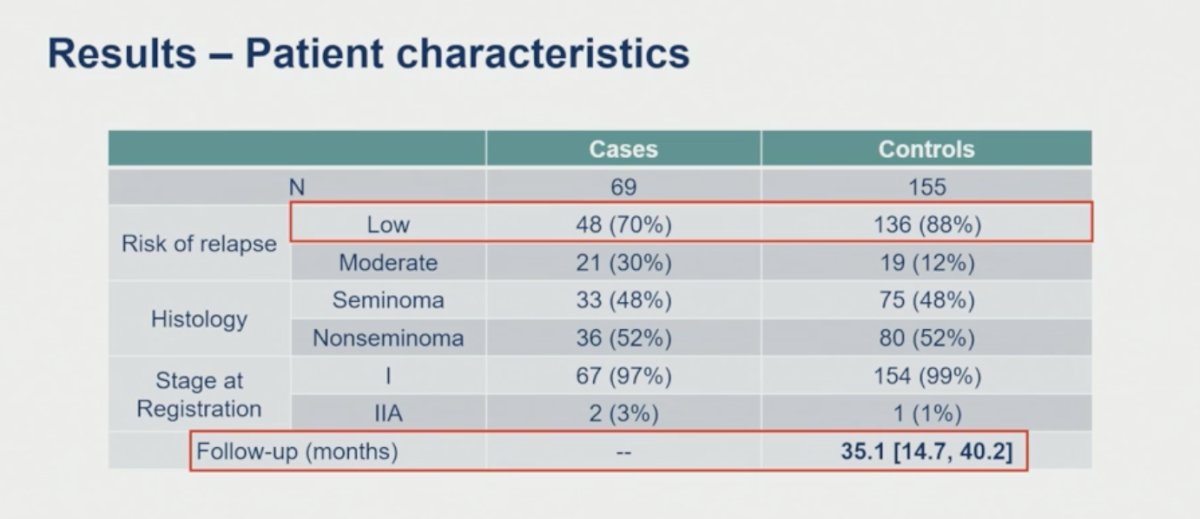
At the time of clinical relapse, miR371 demonstrated strong operating characteristics within the overall cohort, achieving a specificity of 0.94 (95% CI 0.90-0.97) and a negative predictive value of 0.90 (95% CI 0.88-0.92). Sensitivity was 0.54 (95% CI 0.42-0.65), while the positive predictive value reached 0.65 (95% CI 0.51-0.80). Overall diagnostic performance was supported by an area under the curve of 0.75 (p<0.001). Dr. Nappi also noted that most blood samples were collected very close to the time of relapse detection, with 14% obtained 1-2 months prior to relapse and 80% collected within 0-1 months following clinical relapse diagnosis.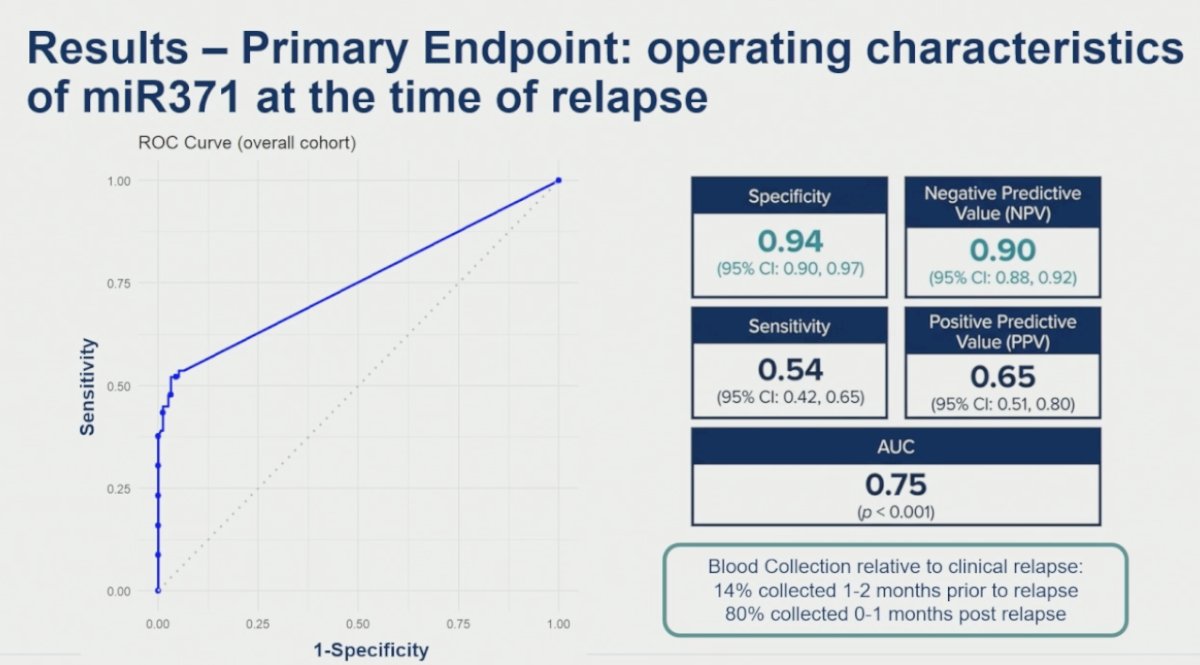
The sensitivity of miR371 increased with a higher stage of relapse. Sensitivity was 39% for stage IIA relapse, increased to 57% for stage IIB disease, and reached 69% among patients with stage II/III relapse. She highlighted that approximately two-thirds of relapse events detected using conventional CT imaging and serum tumor markers occurred at stage IIB or higher, suggesting that miR371 performance improves in the setting of greater disease burden.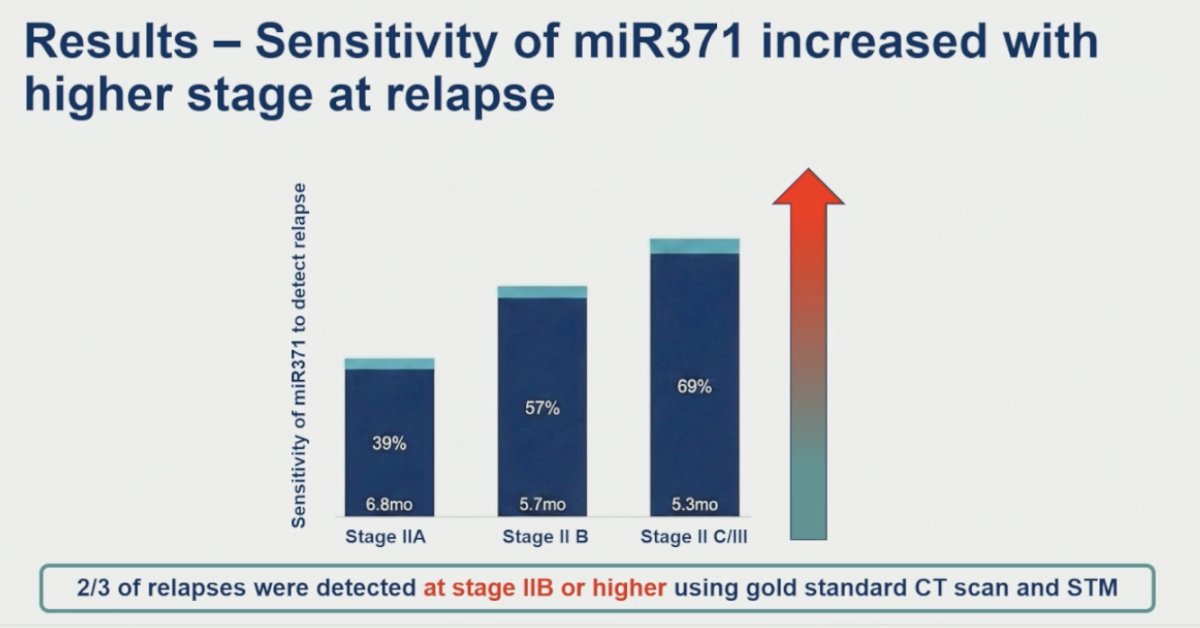
Among the 51 patients who ultimately relapsed and had available baseline miR371 samples, Dr. Nappi demonstrated that miR371 positivity increased substantially from baseline to the time of relapse. Overall, only 22% of patients were miR371-positive at baseline, compared with 57% at relapse. This pattern was observed across histologies and risk groups. Among patients with nonseminoma, positivity increased from 17% at baseline to 63% at relapse, while in seminoma, positivity increased from 26% to 52%. Similarly, among low-risk patients, miR371 positivity rose from 19% at baseline to 56% at relapse, whereas moderate-risk patients demonstrated positivity rates increasing from 36% to 58%. Median time to relapse remained similar between groups, approximately 6 months.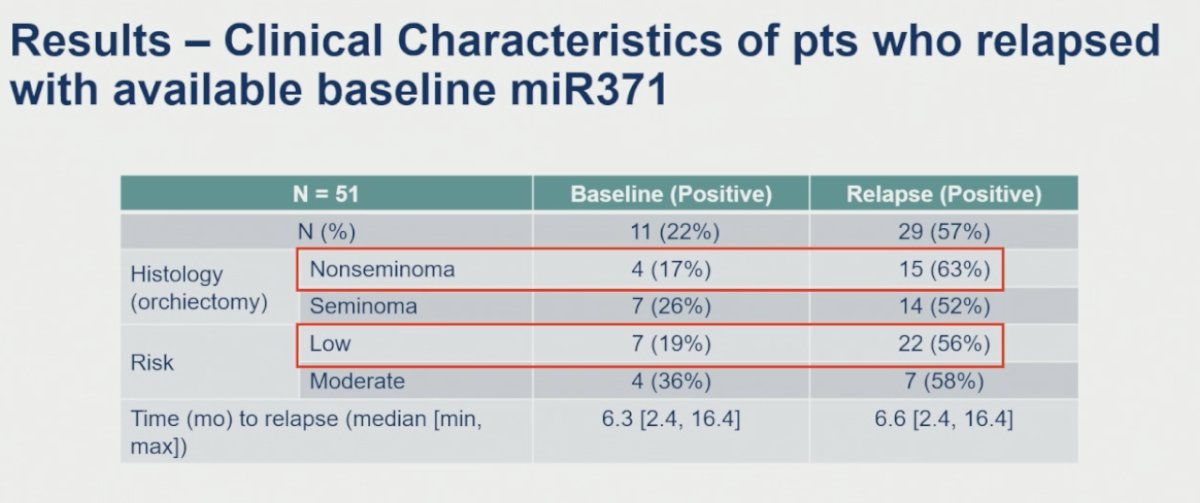
Moreover, Dr. Nappi highlighted a significant association between post-orchiectomy baseline miR371 positivity and relapse-free survival. Patients with positive baseline miR371 following orchiectomy experienced markedly inferior relapse-free survival compared with miR371-negative patients, with a hazard ratio of 9.9 that was highly statistically significant (p<0.001). She emphasized that these findings suggest persistent miR371 positivity after orchiectomy may identify patients harboring occult residual disease at substantially higher risk of relapse during active surveillance.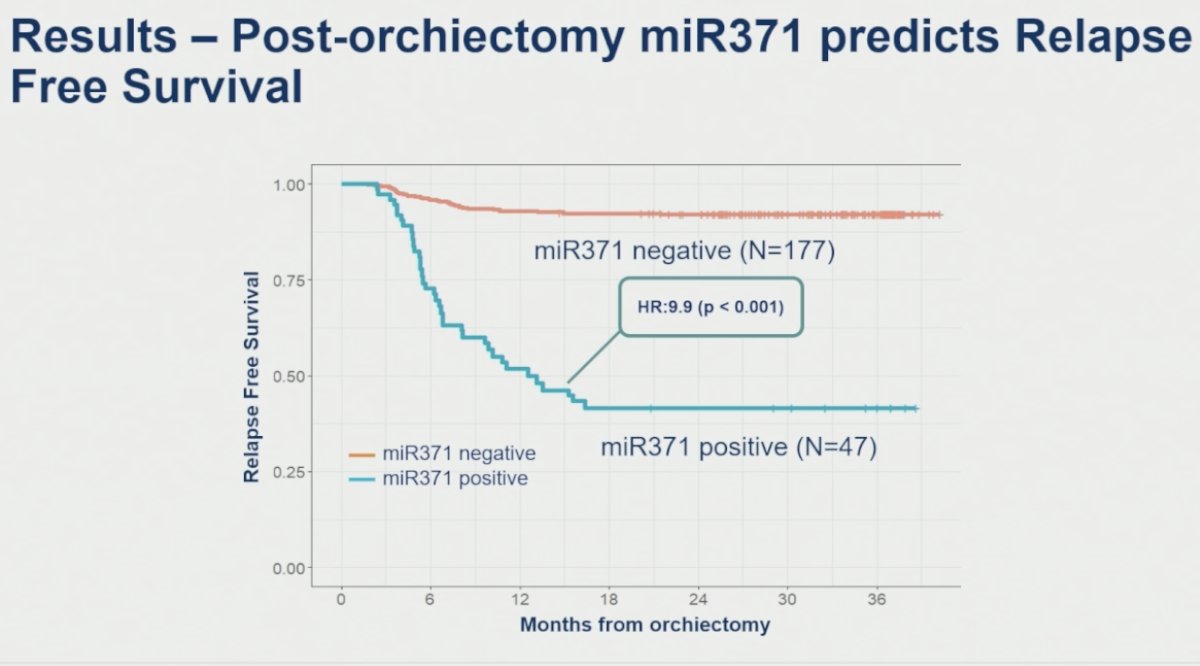
Dr. Nappi also evaluated the operating characteristics of baseline post-orchiectomy miR371 specifically among patients who subsequently relapsed during surveillance. In this setting, miR371 demonstrated high specificity of 0.94 (95% CI 0.90-0.97) and a negative predictive value of 0.84 (95% CI 0.82-0.86), although sensitivity remained limited at 0.22 (95% CI 0.10-0.33). The positive predictive value was 0.43 (95% CI 0.24-0.63), with an overall AUC of 0.58 (p=0.005).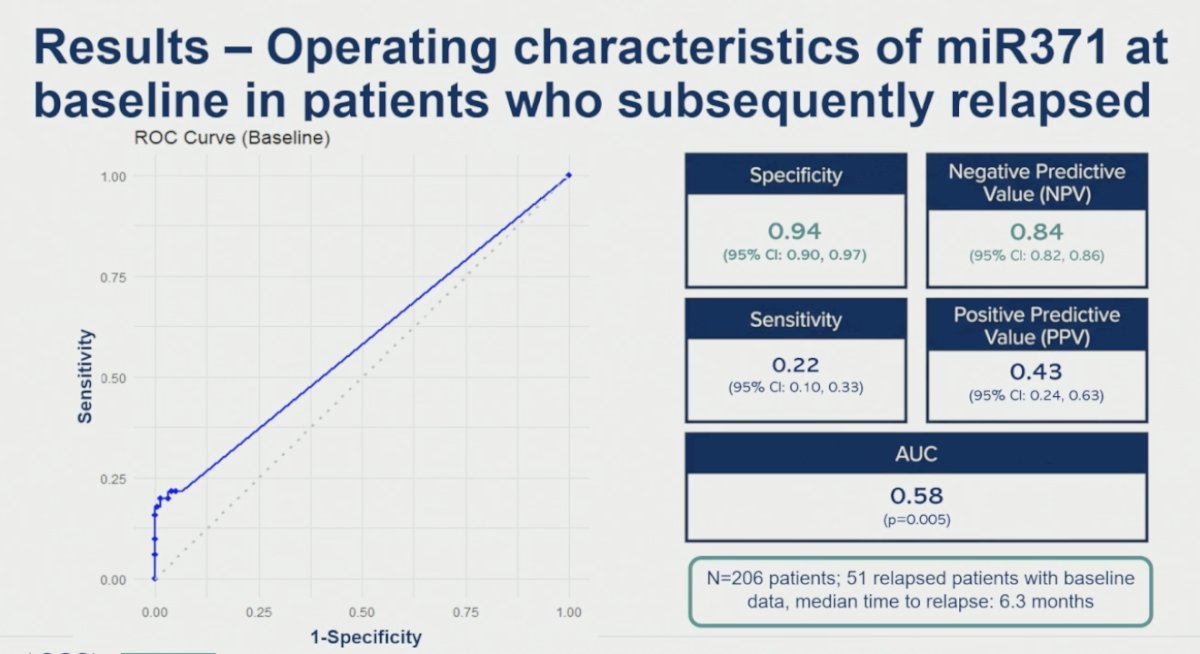
Dr. Nappi subsequently presented swimmer plot analyses among patients who ultimately relapsed and had available baseline miR371 samples, further stratified according to risk group. Among low-risk patients, who were predominantly composed of CSI seminoma cases, the median time to relapse was approximately 7 months, shorter than initially anticipated. In this subgroup, the sensitivity of miR371 for relapse detection was 56%, although only 20% of low-risk patients demonstrated true-positive miR371 positivity at baseline. In contrast, moderate-risk patients, primarily consisting of LVI-positive nonseminoma, experienced a substantially shorter median time to relapse of approximately 4 months. Sensitivity for relapse detection in this cohort reached 59%, with 33% of moderate-risk patients demonstrating true-positive baseline miR371 positivity.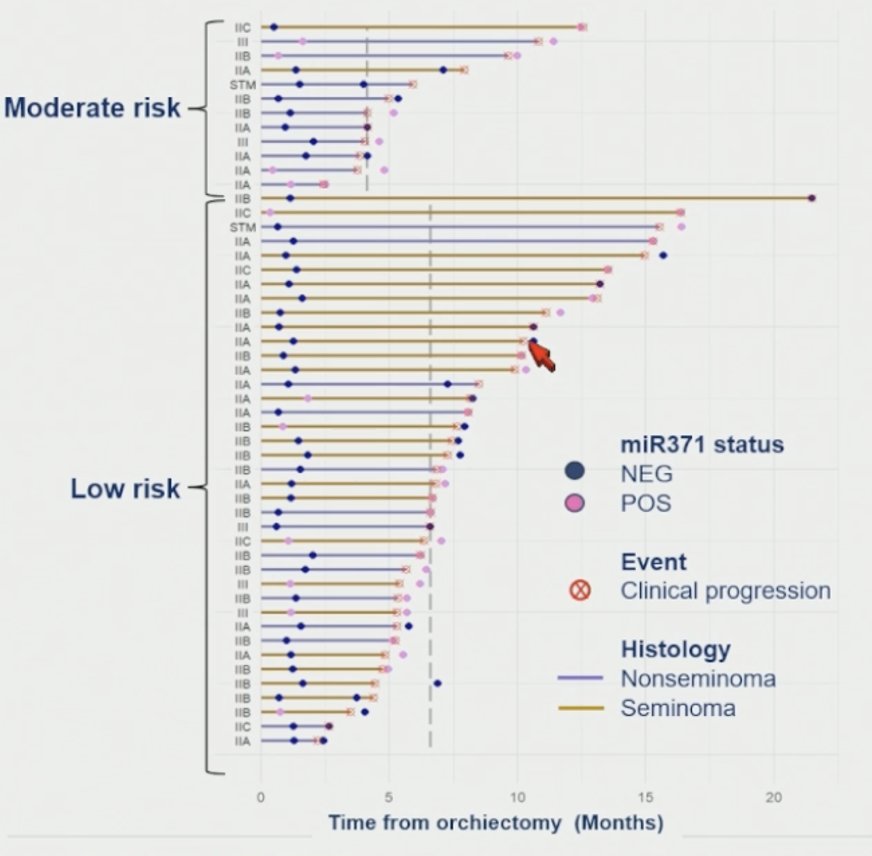
ROC analyses demonstrated similar performance between the low- and moderate-risk cohorts, with overlapping ROC curves and AUC values of 0.74 and 0.77, respectively. She emphasized that, collectively, these findings strongly suggest that miR371 outperforms the historical accuracy of conventional serum tumor markers such as AFP and HCG, particularly in seminoma. Moreover, Dr. Nappi highlighted that the high specificity of miR371 for germ cell tumors appears superior to cross-sectional imaging, while its sensitivity was competitive with contemporary imaging-based surveillance approaches.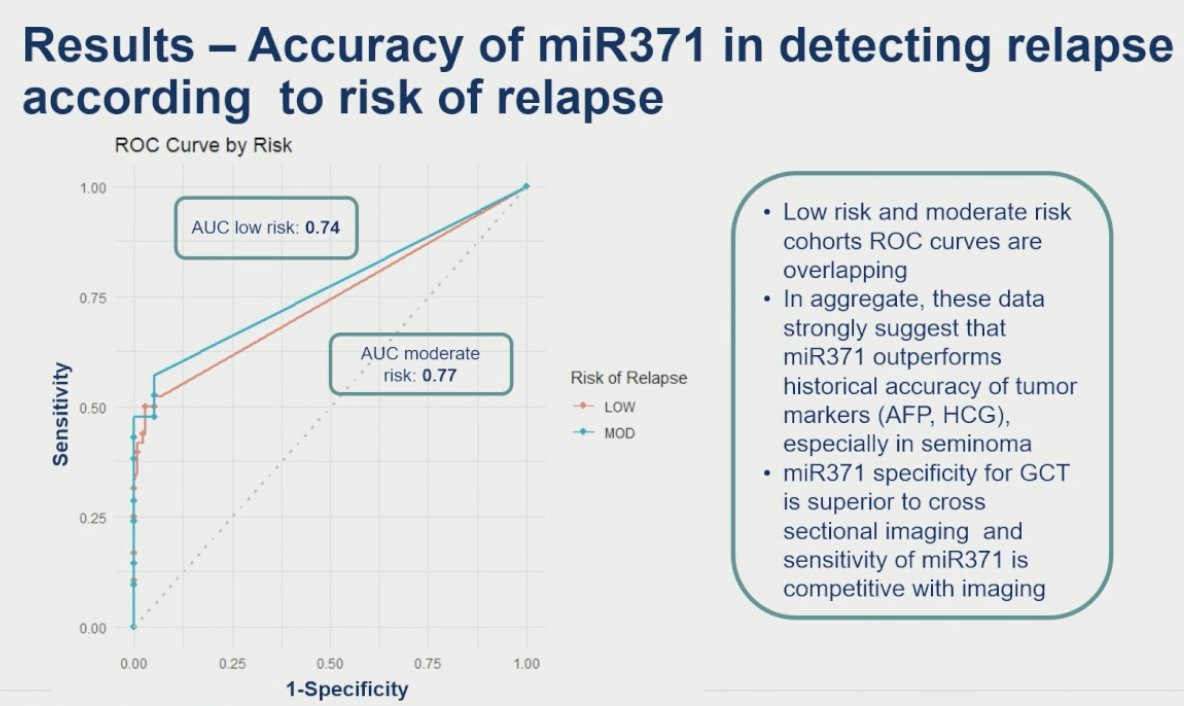
Dr. Nappi also reviewed false-positive miR371 results among control patients who did not experience relapse during surveillance. Overall, only 10 of 155 control patients demonstrated a false-positive result, corresponding to a false-positive rate of 6% and confirming an overall specificity of 94%. False-positive events were evenly distributed between seminoma and nonseminoma histologies, with five cases each, and occurred predominantly within the low-risk cohort, which accounted for 9 of the 10 false-positive cases. Importantly, median follow-up among these patients exceeded 30 months, with an overall follow-up duration of approximately 37.5 months, supporting the durability of the negative clinical outcomes despite isolated positive miR371 findings.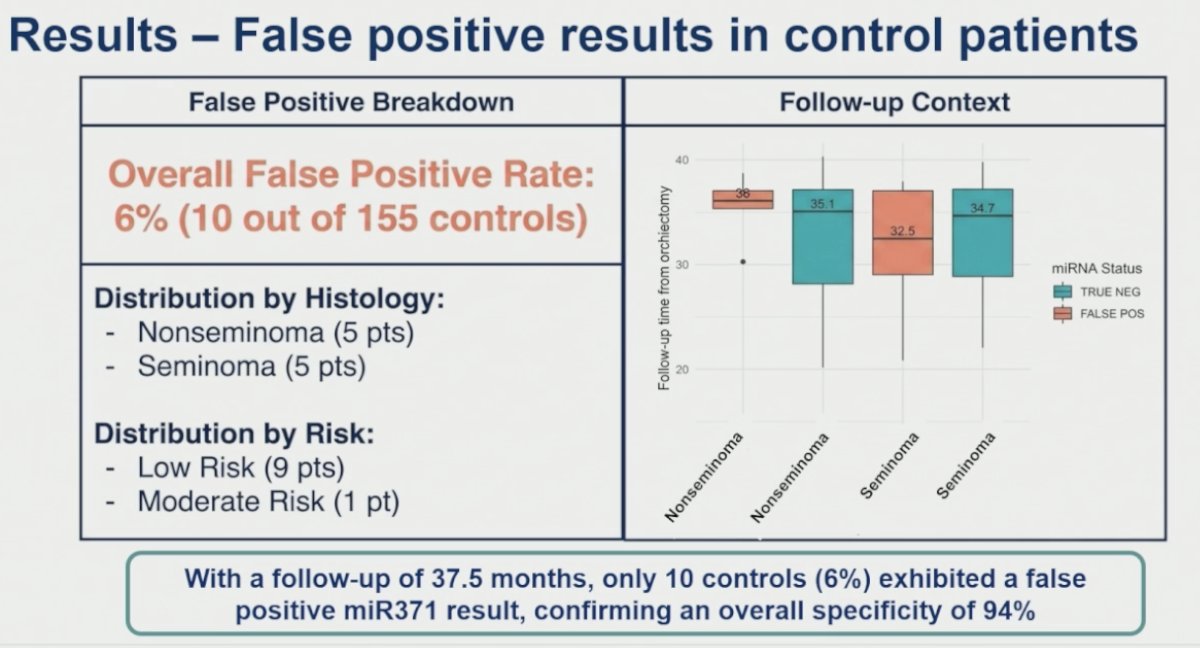
Dr. Nappi acknowledged several important limitations of the current analysis, including the selected nature of the cohort derived from a preplanned interim analysis focusing on the first 69 relapse events within a case-control study design. She also noted the limited number of baseline samples available for analysis. In addition, the current report was restricted to qualitative miR371 assessment, with results categorized as positive or negative. Dr. Nappi emphasized that quantitative miR371 analyses at baseline and longitudinally throughout surveillance are ongoing and will be presented as part of the full cohort analysis in a subsequent report.
Dr. Nappi concluded by outlining several important next steps for the clinical development of miR371 in testicular cancer surveillance. These efforts include completion of the full cohort analysis incorporating longitudinal samples from both relapsed and non-relapsed patients, as well as development of quantitative longitudinal miR371 assays over time during surveillance. She also highlighted ongoing cross-validation initiatives through international collaborations, including the ANZUP CLIMATE study and the Italian Germ Cell Study Group BRIDGE study, aimed at external verification of findings. Finally, Dr. Nappi emphasized future clinical utility and practice integration studies, including GCC.2 through the Canadian Cancer Trials Group and the MAGESTIC study, which aim to further define how miR371 can be incorporated into routine clinical management of germ cell tumors.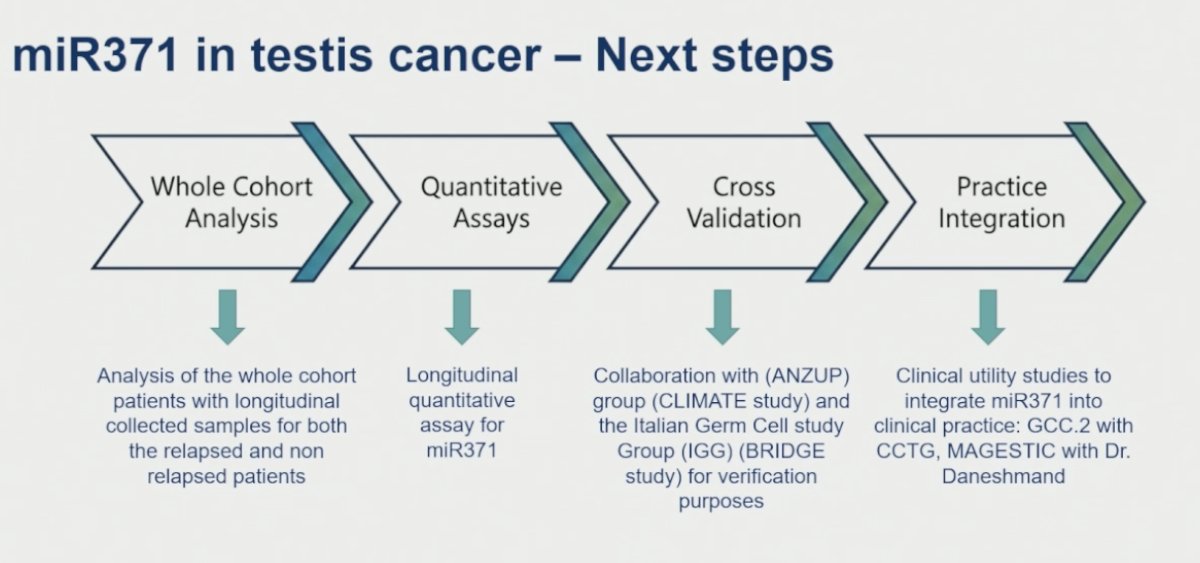
Dr. Nappi concluded her presentation with the following key takeaway messages:
- The SWOG S1823/GCC.1 study demonstrated very high specificity (94%) and negative predictive value (90%) for miR371 in detecting relapse among patients with early-stage germ cell tumors managed with active surveillance.
- miR371 sensitivity and positive predictive value increased in patients with more advanced relapse burden, further supporting the association between miR371 expression and tumor burden.
- This investigator-initiated and real-world collaborative study conducted across centers in Canada and the United States supports the clinical promise of miR371 as a surveillance biomarker in germ cell tumors.
- The clinical utility of miR371 continues to evolve, with additional miR371-informed prospective and longitudinal studies currently underway.
Presented by: Lucia Nappi, MD, PhD, Vancouver Prostate Centre, Department of Urologic Sciences, University of British Columbia, Vancouver, BC, Canada
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026