(UroToday.com) The 2026 ASCO annual meeting featured a plenary session and a discussant presentation by Dr. Jeremie Calais discussing two abstracts, including “AcTION: Phase 1 study of 225Ac-PSMA-617 in men with mCRPC with or without prior 177Lu-PSMA radioligand therapy” presented by Dr. Louise Emmett, and “CONVERGE-01 Part 3: Ac-225 rosopatamab tetraxetan (CONV01-alpha) in 177Lu-PSMA pretreated mCRPC” presented by Dr. Michael Morris.
Dr. Calais started his discussant presentation by reviewing the fundamental differences between beta and alpha emitters. Examples of beta emitters include lutetium-177, iodine-131, and yttrium-90, whereas alpha emitters include actinium-225, lead-212, and astatine-211. Beta particles are characterized by low linear energy transfer radiation of approximately 0.2–1 keV/μm and tissue penetration exceeding 1–3 mm, creating a cross-fire effect that generally requires approximately 2,000 radiation hits to induce cell death. In contrast, alpha particles generate high linear energy transfer radiation of 50–250 keV/μm, nearly 100-fold greater than beta emitters, with a path length of less than 10–100 μm. Consequently, only 2–10 alpha-particle hits may be required for cell killing. Dr. Calais emphasized that the radiobiology of targeted alpha therapy differs substantially from both external beam radiation therapy and beta-emitter radioligand therapy. Alpha particles cause densely ionizing radiation damage that results in complex DNA lesions, including double-strand breaks that are difficult to repair. These effects are less dependent on reactive oxygen species generation, tumor oxygenation status, or cell-cycle phase. Alpha radiation may therefore be particularly effective against micrometastatic disease and isolated tumor cells. Additionally, alpha radiation may induce bystander effects, immune modulation, and microenvironmental changes beyond direct tumor-cell killing.
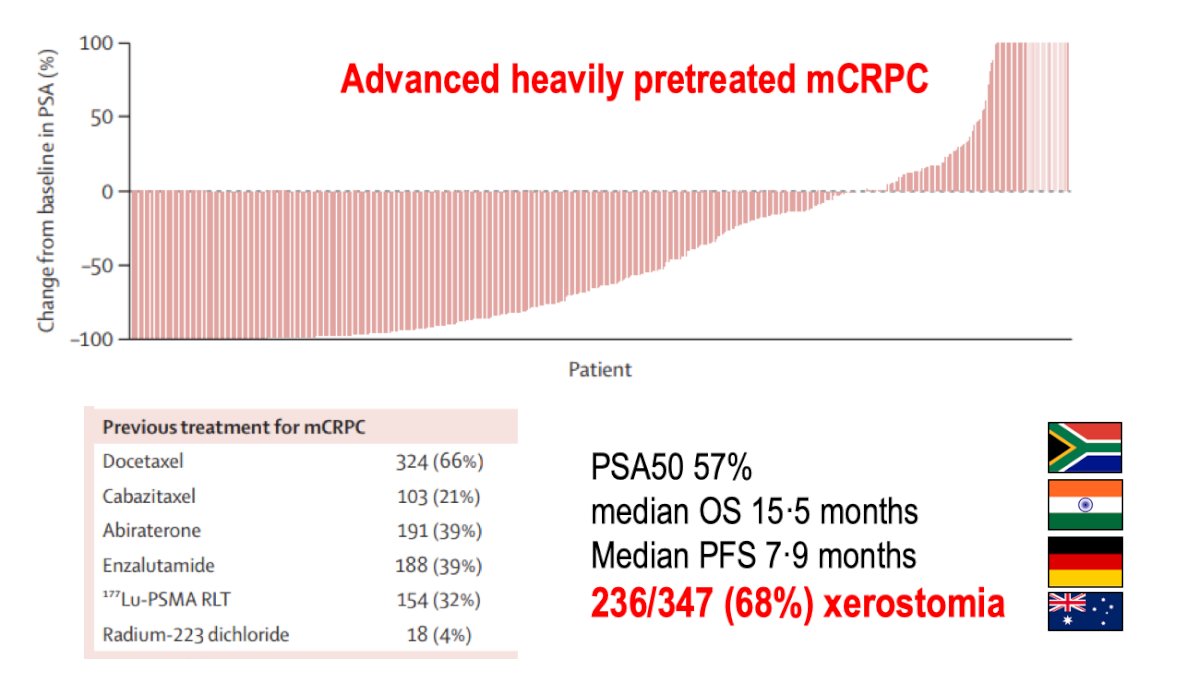
In terms of clinical experience with actinium-225 PSMA-targeted therapy, Dr. Calais reviewed several compassionate-use and retrospective studies evaluating actinium-225 PSMA-617 and PSMA-I&T across a range of disease settings, including metastatic hormone-sensitive prostate cancer, chemotherapy-naïve mCRPC, heavily pretreated mCRPC, and patients with diffuse bone marrow involvement or more than 20 bone metastases. Specific to the WARMTH Act study, the PSA50 response rate was 57%, the median progression-free survival was 7.9 months, and the median overall survival was 15.5 months. However, treatment-related xerostomia remained common, occurring in 236 of 347 patients (68%):1
Next, Dr. Calais next reviewed the rapidly expanding prospective clinical trial landscape for actinium-225 PSMA-targeted therapy. Ongoing studies include the phase 1 Single Dose Escalation study (NCT03276572), Fractionated Multiple Dose study (NCT04506567), AcTION (NCT04597411), TATCIST (NCT05219500), SatisfACtion (NCT05983198), FL-020 (NCT06492122), ACCEL (NCT06229366), CONVERGE-01 (NCT06549465), AlphaBreak (NCT06402331), PAnTHA (NCT06217822), PSMA-XT (NCT07135102), NeoPSMA (NCT06881823), PSMAcTION (NCT06780670), AcTFirst (NCT06855277), ANDROMEDA (NCT07150715), and AlphaPRO. These studies collectively span multiple disease states ranging from oligometastatic hormone-sensitive disease to advanced mCRPC:

Importantly, there are now alternative targeting platforms beyond the PSMA-617 small molecule. Dr. Calais highlighted J591, also known as rosopatamab tetraxetan, a PSMA-targeting monoclonal antibody. Compared with the approximately 1 kDa PSMA-617 small molecule, J591 is a 150 kDa antibody that remains in circulation for days rather than hours. This prolonged circulation may result in greater tumor retention and potentially higher radiation dose delivery. However, it may also increase marrow exposure, although the antibody platform may reduce salivary gland toxicity. Ongoing trials include ProstACT Select, ProstACT TARGET, CONVERGE-01, and the phase 3 ProstACT Global trial:

Dr. Calais highlighted dosing strategies for actinium-225 PSMA therapy. For the J591 antibody, weight-based dose-escalation studies evaluating 45 and 55 kBq/kg established a recommended phase 3 dose of 9 MBq per cycle, corresponding to a cumulative activity of 18 MBq. For 225Ac-PSMA-617, separate fixed-dose escalation studies evaluating 4, 6, 8, and 10 MBq established 10 MBq as the recommended phase 2 dose, with a potential cumulative activity of 60 MBq administered over six treatment cycles:

With regards to the two trials presented, the AcTION trial is the first prospective dosage escalation study of 225Ac-PSMA-617, an alpha-emitting, PSMA-targeted radioligand therapy in patients with mCRPC (NCT04597411). This study enrolled patients with progressive, PSMA-positive mCRPC in 3 groups:
- Group A: prior chemotherapy and an androgen receptor pathway inhibitor (ARPI), but no prior 177Lu-PSMA radioligand therapy
- Group B: no prior chemotherapy, ARPI, or 177Lu-PSMA radioligand therapy (chemotherapy/ARPI-naïve)
- Group C: prior 177Lu-PSMA radioligand therapy
In Group A, the PSA50 rate was 58.8% (95% CI 40.7, 75.4) and PSA90 rate was 63.6% (95% CI 30.8, 89.1). For Group B patients, the PSA50 rate was 100% (95% CI 71.5, 100) and PSA90 rate was 90.9% (95% CI 58.7, 99.8). For Group C patients, the PSA50 rate was 56.3% (95% CI 29.9, 80.2) and PSA90 rate was 18.8% (95% CI 4.0, 45.6).
CONV01-α is an alpha-emitting radionuclide conjugated to a PSMA-targeting monoclonal antibody, which was assessed in the phase 2 multi-center CONVERGE-01 trial. This trial evaluated the safety and efficacy of CONV01-α in patients with mCRPC, including those previously treated with Lu-PSMA-617 or -I&T (Lu-PSMA) in a dose escalation and in an initial expansion cohort. Eligible patients for CONVERGE-01 had PSMA PET-positive (VISION criteria2) mCRPC with previous exposure to ≥1 ARPI, 0-1 taxane regimens, and 1-6 cycles of Lu-PSMA. CONV01-α was administered in a single cycle of two doses (D1 and D15). Dr. Calais emphasized that CONV01-α demonstrated promising activity in 177Lu-PSMA-617-exposed patients, with a PSA50 rate of 40%. Although we must be cautious with comparisons between trials, Dr. Calais provided the following data from these two trials in the context of 177Lu-PSMA-617 results in PSMAddition and VISION:2
![CONV01-α is an alpha-emitting radionuclide conjugated to a PSMA-targeting monoclonal antibody, which was assessed in the phase 2 multi-center CONVERGE-01 trial. This trial evaluated the safety and efficacy of CONV01-α in patients with mCRPC, including those previously treated with Lu-PSMA-617 or -I&T (Lu-PSMA) in a dose escalation and in an initial expansion cohort. Eligible patients for CONVERGE-01 had PSMA PET-positive (VISION criteria [2]) mCRPC with previous exposure to ≥1 ARPI, 0-1 taxane regimens, and 1-6 cycles of Lu-PSMA. CONV01-α was administered in a single cycle of two doses (D1 and D15). Dr. Calais emphasized that CONV01-α demonstrated promising activity in 177Lu-PSMA-617-exposed patients, with a PSA50 rate of 40%. Although we must be cautious with comparisons between trials, Dr. Calais provided the following data from these two trials in the context of 177Lu-PSMA-617 results in PSMAddition and VISION [2]:](/images/com-doc-importer/271-asco-2026/asco-2026-discussant-moving-beyond-beta-emitters-the-next-generation-radioligand-therapies-in-prostate-cancer/image-4.jpg)
The safety profile of actinium-225 therapies was then compared with data from phase 3 lutetium-177 PSMA studies:
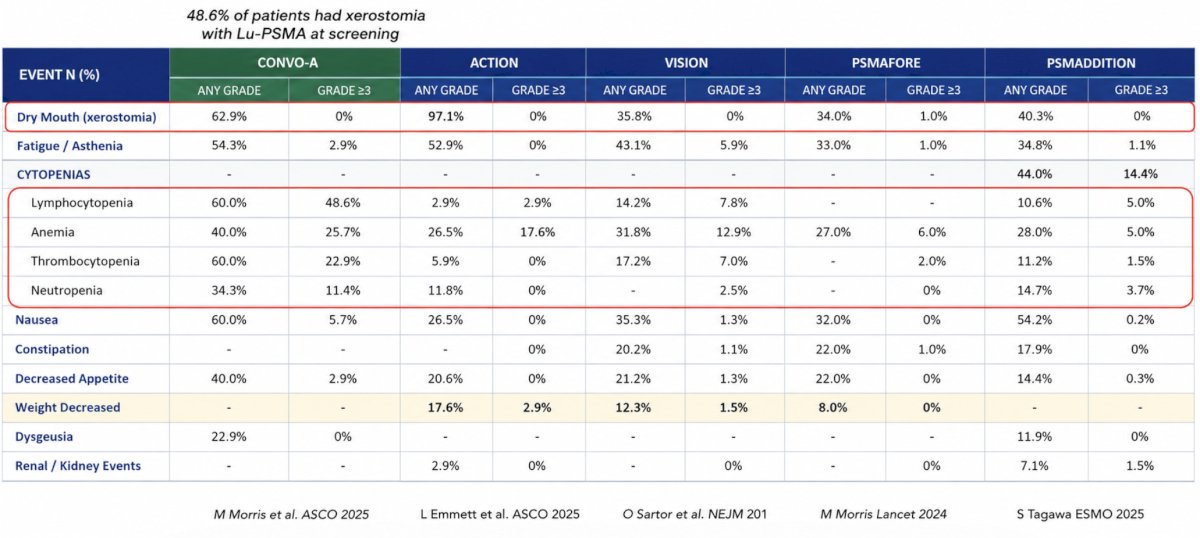
Xerostomia remains a major toxicity concern. Dr. Calais emphasized that current toxicity grading systems inadequately characterize salivary gland dysfunction and argued that the field must improve assessment strategies. The Xerostomia Inventory, saliva flow measurements, and the FACT-RNT patient-reported outcome instrument are potential tools for more accurately assessing treatment-related salivary toxicity. Unfortunately, current management remains largely symptomatic and supportive rather than regenerative.
Long-term toxicity remains an important area of ongoing investigation. Dr. Calais reviewed emerging data regarding renal toxicity following PSMA-targeted radiopharmaceutical therapy and highlighted ongoing long-term follow-up studies, including NCT05803941, which is monitoring approximately 700 patients treated with lutetium-177 PSMA with CTCAE assessments every six months for up to ten years. Similar concerns exist regarding bone marrow toxicity and therapy-related myeloid neoplasms. A review of 28 studies involving 7,334 patients treated with peptide receptor radionuclide therapy for neuroendocrine tumors reports a mean incidence of therapy-related myeloid neoplasms of 2.61%.
Dr. Calais also discussed combination approaches integrating alpha and beta emitters. Examples include the phase 1/2 study combining lutetium-177 PSMA-I&T with actinium-225 J591 (NCT04886986) and the AlphaBet study evaluating lutetium-177 PSMA-I&T plus radium-223 (NCT05383079). These “tandem” or “cocktail” strategies aim to exploit the complementary biologic properties of alpha and beta radiation. Beyond actinium-225, there are several next-generation radionuclides currently entering clinical development. These include copper-67, terbium-161, lead-212, and astatine-211. Ongoing studies include SECuRE (Cu-67-SAR-bisPSMA), VIOLET (Tb-161-PSMA-I&T), PROGNOSTICS (Tb-161-SibuDAB), TheraPb (Pb-212-ADVC001), ARTISAN (Pb-212-AB001), and Alpha-PS1 (At-211-PSMA-5):

Early efficacy signals from these programs are encouraging. For example, terbium-161 PSMA-I&T demonstrated a PSA50 response rate of 70%, a median PSA progression-free survival of 9 months, and a median progression-free survival of 11 months. Copper-67 SAR-bisPSMA and astatine-211 PSMA-targeted therapies also continue to generate interest as novel radiopharmaceutical platforms.
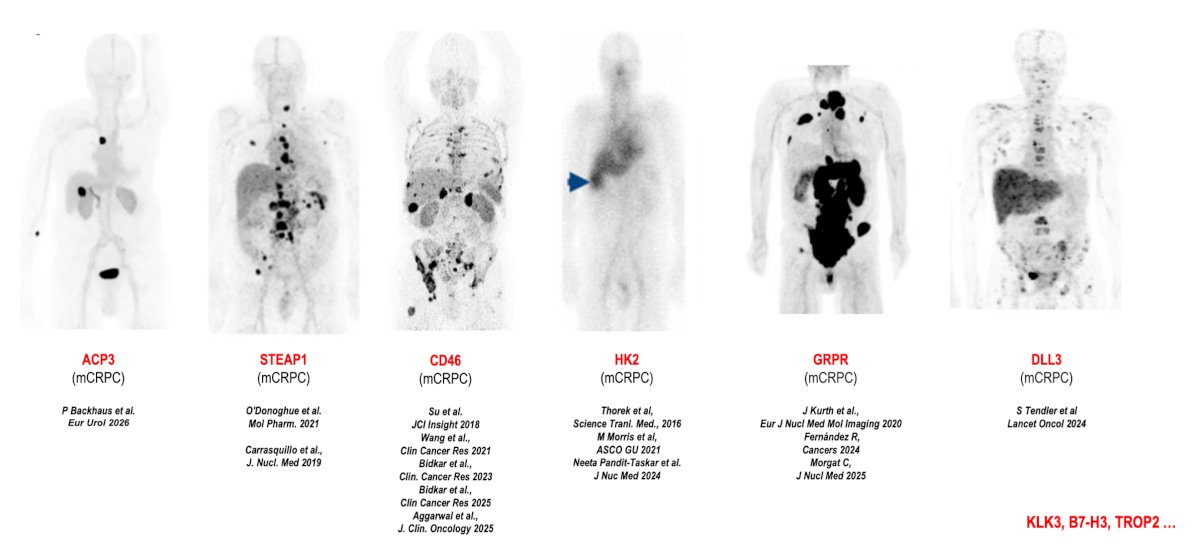
Dr. Calais also discussed several emerging therapeutic targets in mCRPC beyond PSMA. These include STEAP1, CD46, hexokinase-2 (HK2), gastrin-releasing peptide receptor (GRPR), DLL3, ACP3, KLK3, B7-H3, and TROP2. These targets may ultimately provide therapeutic opportunities for patients whose tumors exhibit heterogeneous PSMA expression or resistance to PSMA-directed treatment:
Finally, several next-generation ligand developments include the following examples:
- PSMA-RADmAb (TLX592-Tx): a monoclonal antibody engineered for faster clearance than conventional antibody constructs while maintaining favorable tumor targeting
- HYNIC-iPSMA (TLX597-Tx, PanPSMA): incorporates a hydrazinonicotinamide moiety to increase lipophilicity, enhance tumor retention, reduce passive salivary gland uptake, and potentially decrease renal cortical retention
- Albumin-binding constructs, such as actinium-225 PSMA-Trillium (BAY 3563254), are currently being evaluated in the phase 1 PAnTHA study
Dr. Calais concluded his discussant presentation with the following take-home points:
- Alpha-emitting PSMA-targeted radiopharmaceutical therapy appears to induce higher anti-tumor activity and deeper responses than beta-emitting lutetium-177 PSMA therapy due to distinct radiobiologic mechanisms
- Actinium-225 PSMA-targeted radiopharmaceutical therapy may carry greater toxicity than lutetium-177 PSMA and requires careful disease stage-specific monitoring and quality of life assessment
- Numerous next-generation radiopharmaceutical agents are currently in development, raising the question of whether these therapies will ultimately replace beta emitters or be incorporated alongside them
Presented by: Jeremie Calais, MD, MSc, PhD, Certified Principal Investigator, ACRIP, Associate Professor, Department of Molecular and Medical Pharmacology, Director, Theranostics Program, Director, Clinical Research Program, Ahmanson Translational Theranostics Division, David Geffen School of Medicine, University of California, Los Angeles (UCLA), Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- Sathekge MM, Lawal IO, Bal C, et al. Actinium-225-PSMA radioligand therapy of metastatic castration-resistant prostate cancer (WARMTH Act): A multicentre, retrospective study. Lancet Oncol. 2024 Feb;25(2):175-183.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.