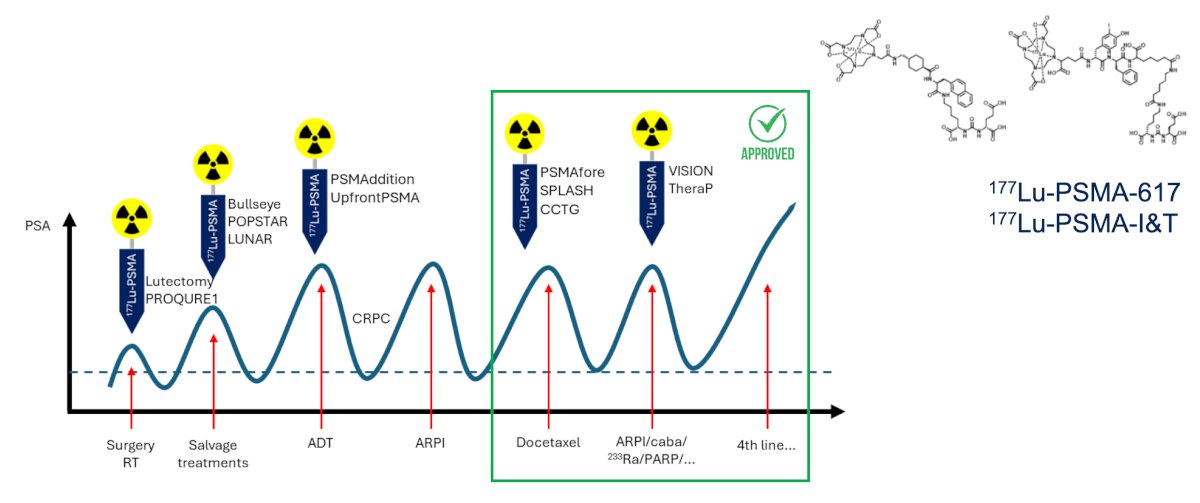
(UroToday.com) The 2026 ASCO annual meeting featured a plenary session and a discussant presentation by Dr. Karolien Goffin discussing “Safety and dosimetry of 177Lu-rosopatamab tetraxetan plus standard of care (SOC) in patients with mCRPC: Preliminary results from part 1 of phase 3 ProstACT Global study” by Dr. Pedro Barata. Dr. Goffin started her discussant presentation by reviewing the current PSMA radioligand therapy landscape, noting that small molecules remain the dominant targeting platform.
Agents such as 177Lu-PSMA-617 and 177Lu-PSMA-I&T have established the foundation for modern PSMA-targeted radiopharmaceutical therapy:
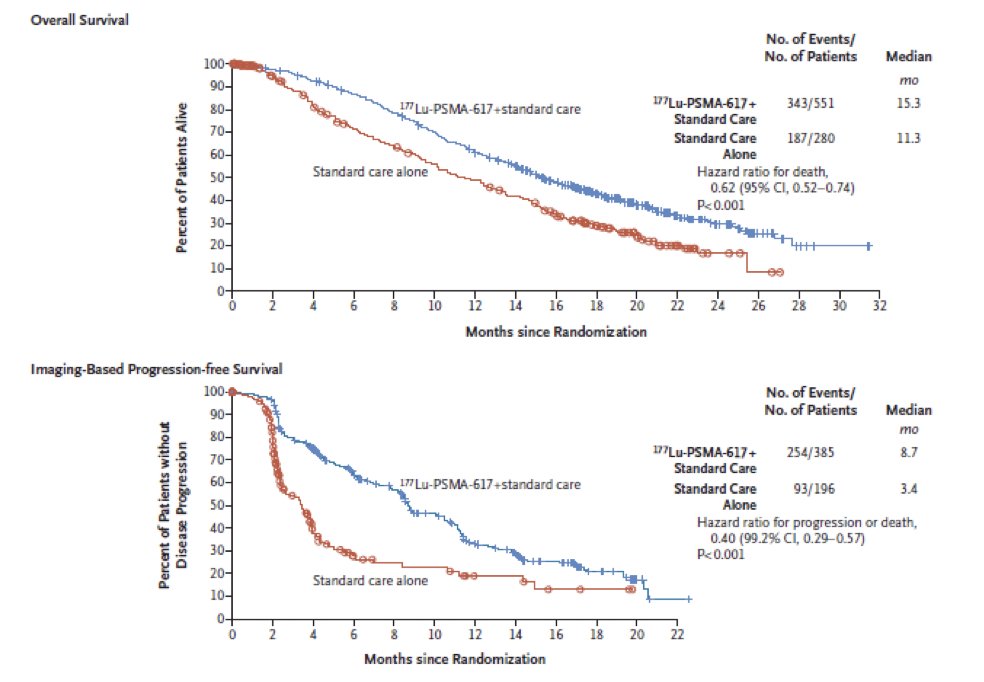
There have been several pivotal trials that have established 177Lu-PSMA-617 as a standard treatment option. In VISION,1 patients with PSMA-positive mCRPC who had progressed after androgen receptor pathway inhibition (ARPI) and docetaxel experienced an overall survival (HR 0.62, 95% CI 0.52-0.74) and radiographic progression-free survival (HR 0.40, 99.2% 0.29-0.57) benefit with 177Lu-PSMA-617:
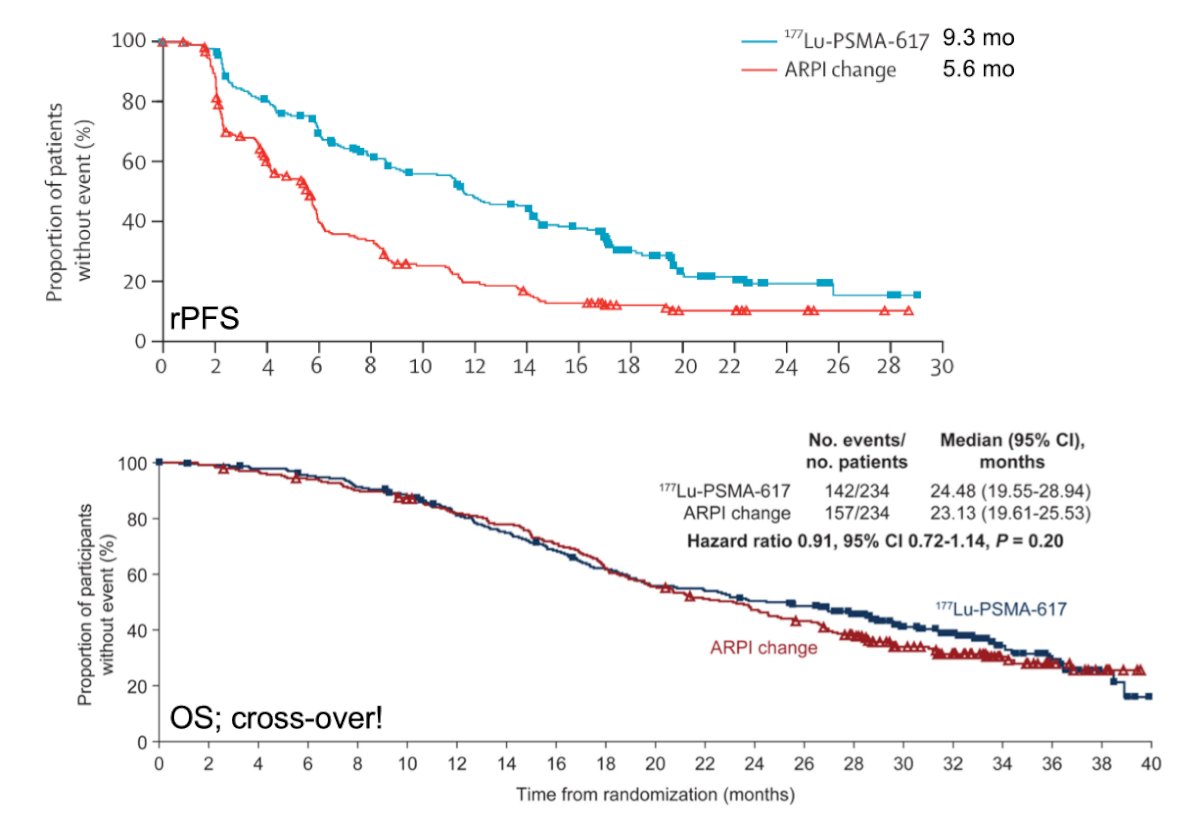
Subsequently, PSMAfore2 demonstrated improved radiographic progression-free survival (9.3 versus 5.6 months) in patients with PSMA-positive mCRPC progressing after ARPI, expanding the role of PSMA-targeted treatment earlier in the disease course. However, there was substantial crossover, and no overall survival benefit was noted in PSMAfore:
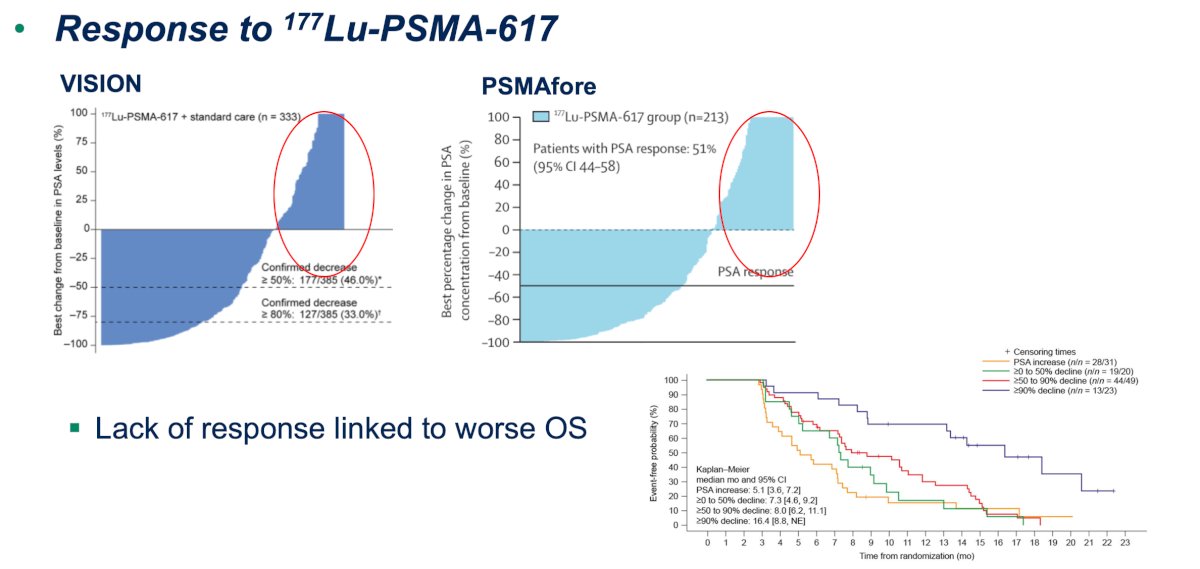
Despite these advances, Dr. Goffin noted that a significant unmet need remains. Data from both VISION and PSMAfore demonstrate that lack of PSA response to 177Lu-PSMA-617 is associated with worse overall survival outcomes.3 Accordingly, strategies to improve efficacy and broaden the therapeutic index of PSMA-targeted treatment continue to be pursued:
There are also practical complexities associated with small-molecule PSMA radioligand therapy. Standard treatment with 177Lu-PSMA-617 generally consists of six cycles administered every six weeks at approximately 200 mCi (7.4 GBq) per treatment. Patients often require dedicated radioligand therapy facilities, radiation safety precautions following administration, post-therapy SPECT/CT imaging, multiple follow-up visits, and repeat PET imaging assessments. In contrast, 177Lu-TLX591 utilizes two cycles administered every two weeks at 76 mCi (2.8 GBq), raising the possibility of a simplified treatment paradigm.
The ProstACT Global study was designed to enroll a population resembling that of PSMAfore. Eligible patients had mCRPC with progression following prior ARPI exposure in the mCSPC, nmCRPC, or mCRPC setting and demonstrated PSMA-positive disease on 68Ga-PSMA-11 PET/CT or PET/MRI. Importantly, ProstACT employed a stricter imaging criterion for PSMA positivity. Patients were required to have at least one lesion demonstrating SUVmax ≥2 times the mean liver SUV. In contrast, PSMAfore required uptake greater than liver parenchyma:
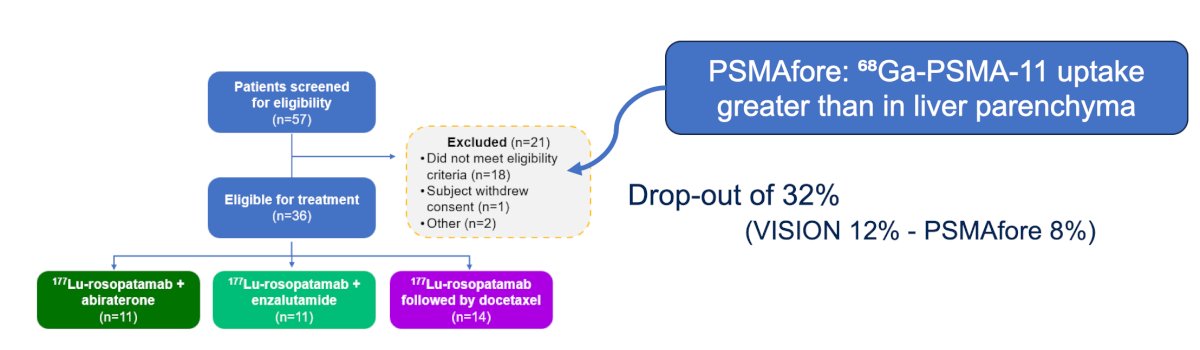
Dr. Goffin noted that this may partially explain the higher screening failure and dropout rates observed in ProstACT Global, where dropout reached 32%, compared with 12% in VISION and 8% in PSMAfore.
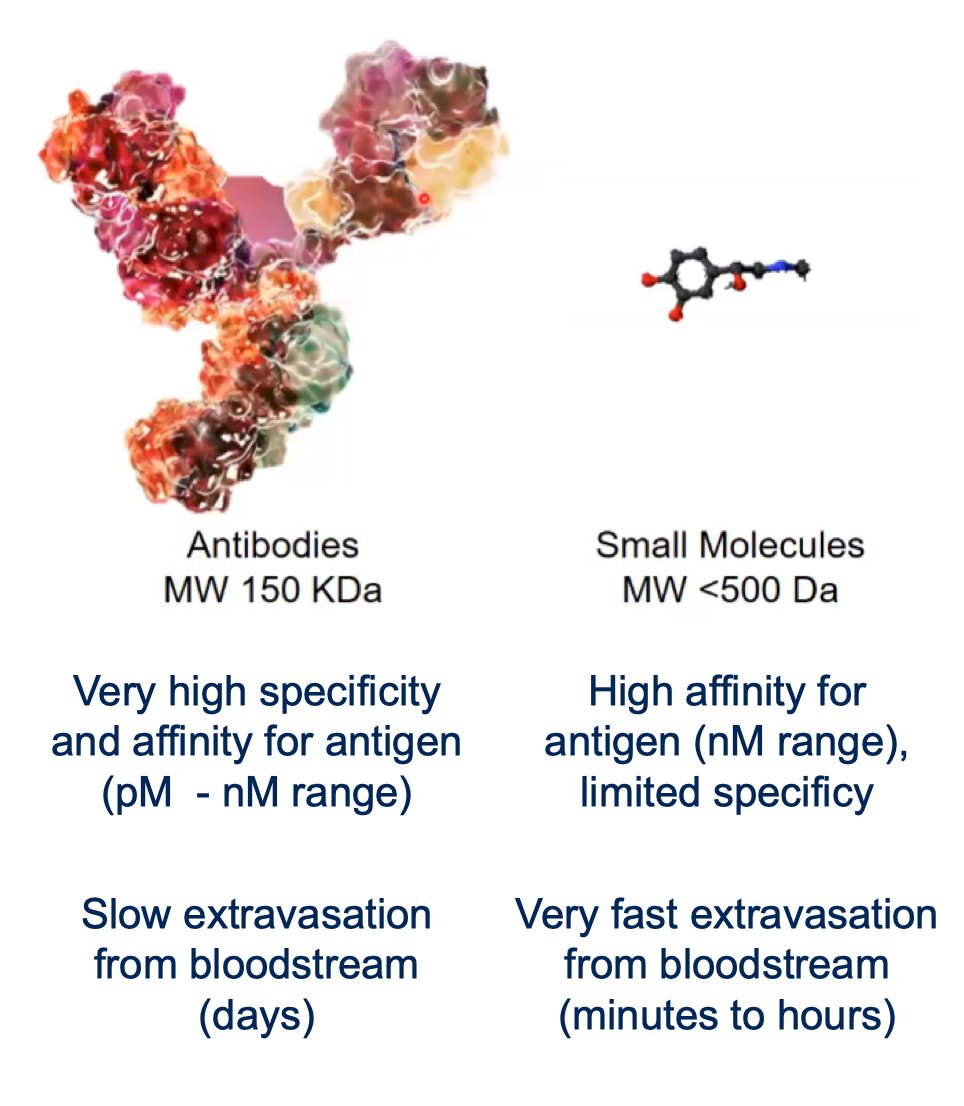
So, why antibodies for radioligand therapy? Monoclonal antibodies exhibit extremely high specificity and affinity for their targets, typically within the picomolar to nanomolar range. Antibodies demonstrate relatively slow extravasation from the bloodstream, often requiring days to reach target tissues. By contrast, small molecules generally exhibit rapid tissue penetration occurring over minutes to hours, albeit with somewhat lower specificity. These biological differences create distinct biodistribution patterns and may influence both efficacy and toxicity:
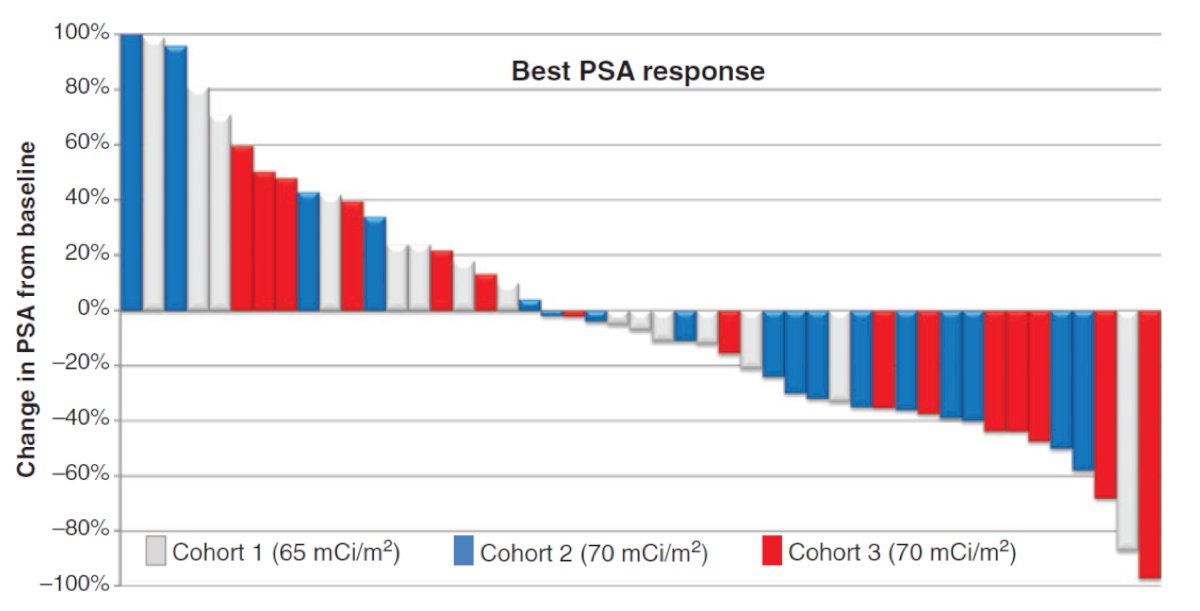
Dr. Goffin reviewed prior experience with 177Lu-J591, an earlier PSMA-targeted antibody radioligand. Although efficacy data were limited, early phase studies provided proof of concept for antibody-mediated PSMA targeting. In 2013, Tagawa et al.4 included 47 mCRPC patients progressing after hormonal therapy, more than half of whom had previously received docetaxel. Patients received a single administration of either 65 or 70 mCi/m² 177Lu-J591 with the following best PSA response:
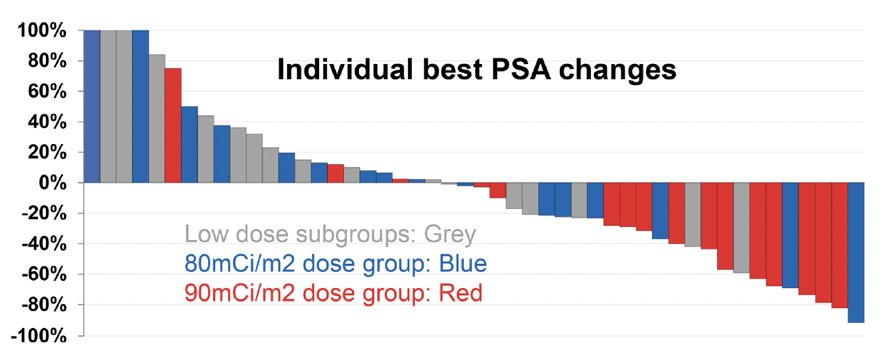
In 2019, Tagawa et al.5 enrolled 49 mCRPC patients who were refractory to or declined standard treatment options and evaluated two cycles of dose-escalated 177Lu-J591, ranging from 20–45 mCi/m² with the following individual best PSA changes:
These studies established feasibility while also highlighting significant hematologic toxicity associated with antibody-based delivery.
In ProstACT Global, Part 1 consists of a safety lead-in and dosimetry cohort, while Part 2 is a randomized expansion phase enrolling approximately 490 patients. The randomized phase is expected to provide pivotal efficacy data comparing 177Lu-TLX591 + standard of care versus standard of care alone and will ultimately determine whether antibody-based PSMA radioligand therapy can establish a role within the contemporary treatment paradigm:

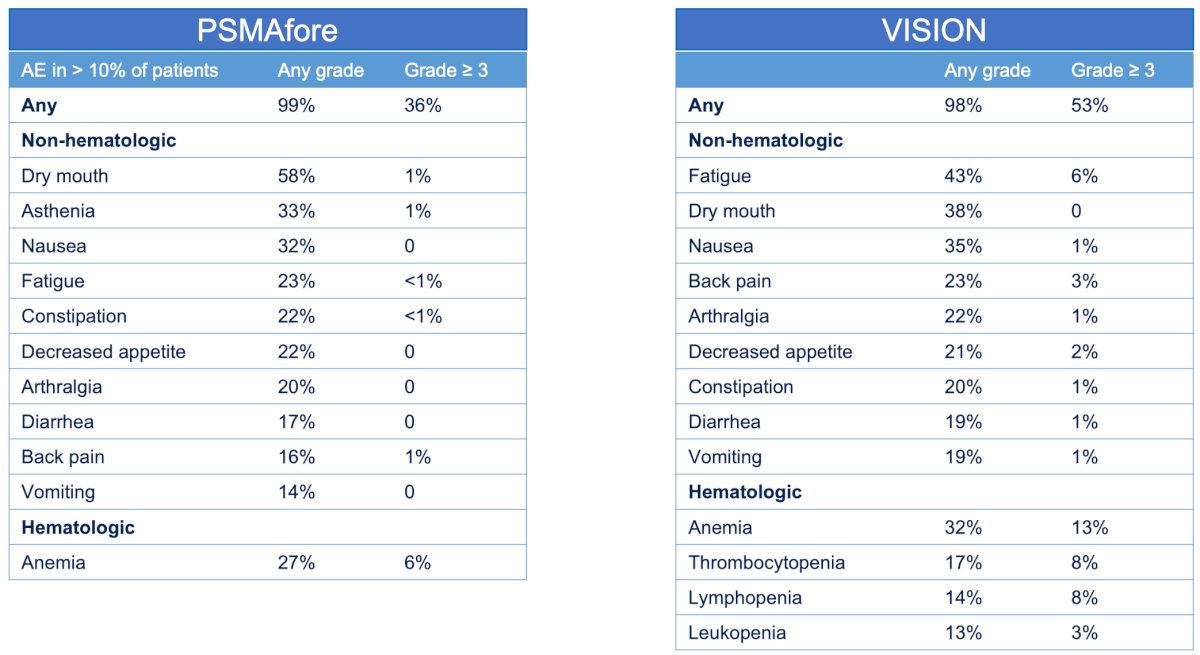
The subsequent portion of the presentation then focused on safety. Using data from VISION and PSMAfore, Dr. Goffin reviewed the adverse event profile of 177Lu-PSMA-617. In VISION, any grade adverse events occurred in 99% of patients, with grade ≥3 events observed in 36%. Dry mouth occurred in 58% of patients, asthenia in 33%, nausea in 32%, fatigue in 23%, constipation in 22%, decreased appetite in 22%, arthralgia in 20%, diarrhea in 17%, back pain in 16%, vomiting in 14%, and anemia in 27%, including 6% grade ≥3 anemia. Similarly, PSMAfore demonstrated high rates of adverse events, with 98% of patients experiencing any-grade toxicity and 53% experiencing grade ≥3 toxicity. Fatigue occurred in 43%, dry mouth in 38%, nausea in 35%, back pain in 23%, arthralgia in 22%, decreased appetite in 21%, constipation in 20%, diarrhea in 19%, vomiting in 19%, anemia in 32%, thrombocytopenia in 17%, lymphopenia in 14%, and leukopenia in 13%:
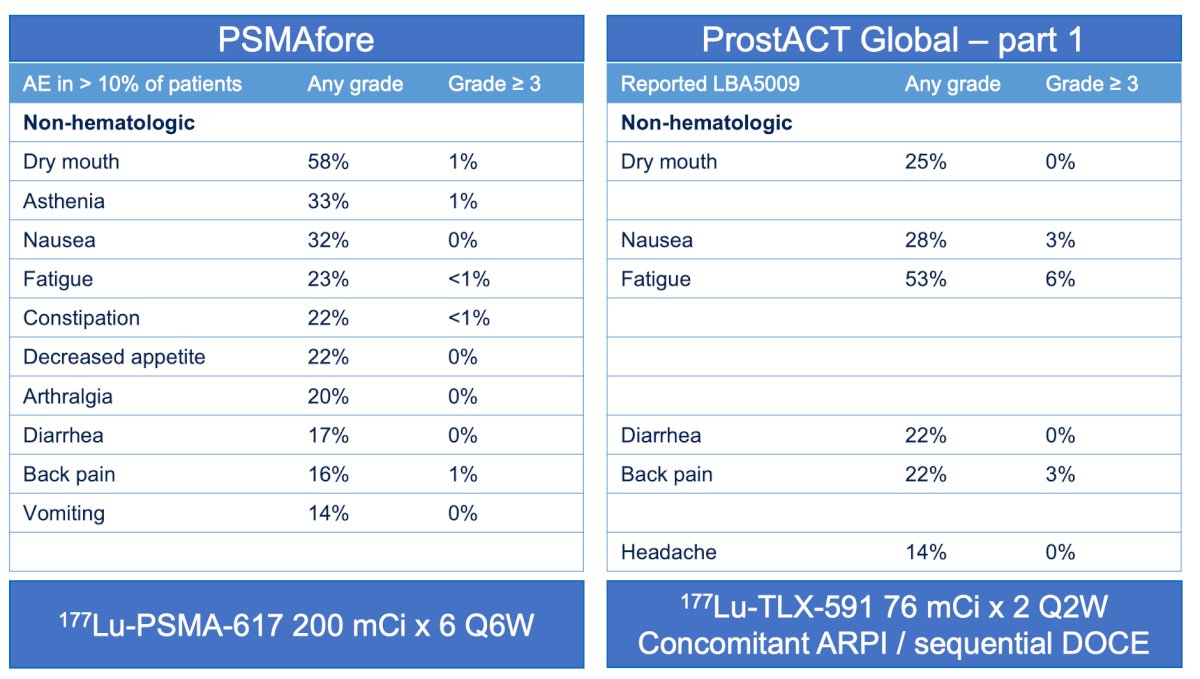
The ProstACT Global safety lead-in revealed a different toxicity profile. Non-hematologic toxicities included any grade dry mouth in 25% of patients with no grade ≥3 events, nausea in 28% with 3% grade ≥3 toxicity, fatigue in 53% with 6% grade ≥3 toxicity, diarrhea in 22% with no grade ≥3 events, back pain in 22% with 3% grade ≥3 toxicity, and headache in 14% without grade ≥3 events:
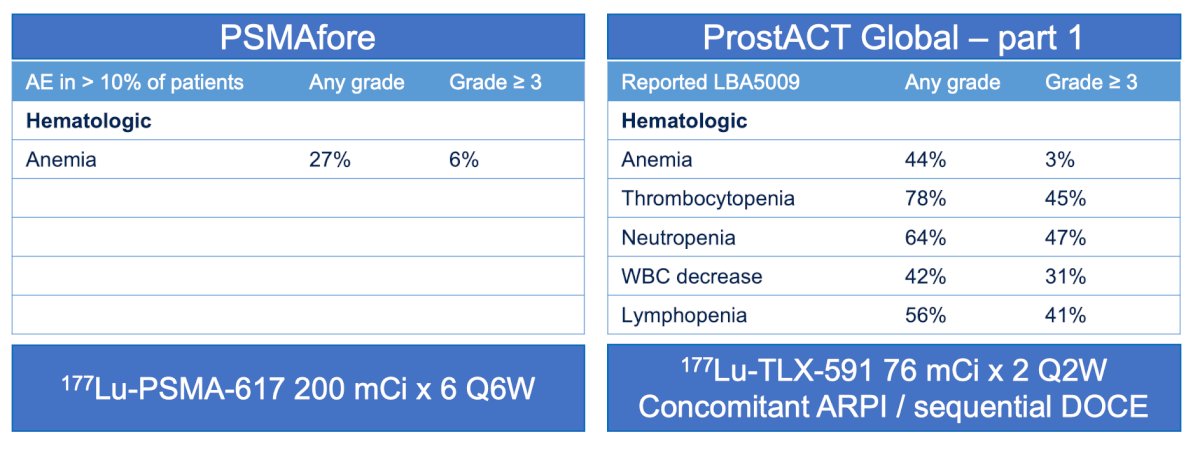
The most notable difference emerged in hematologic toxicity. In ProstACT Global, anemia occurred in 44% of patients (any grade), including 3% grade ≥3 events. Thrombocytopenia occurred in 78% of patients, with 45% experiencing grade ≥3 thrombocytopenia. Neutropenia occurred in 64% of patients, including 47% grade ≥3 events. White blood cell decreases occurred in 42% of patients, including 31% grade ≥3 events, while lymphopenia occurred in 56% of patients, including 41% grade ≥3 events:
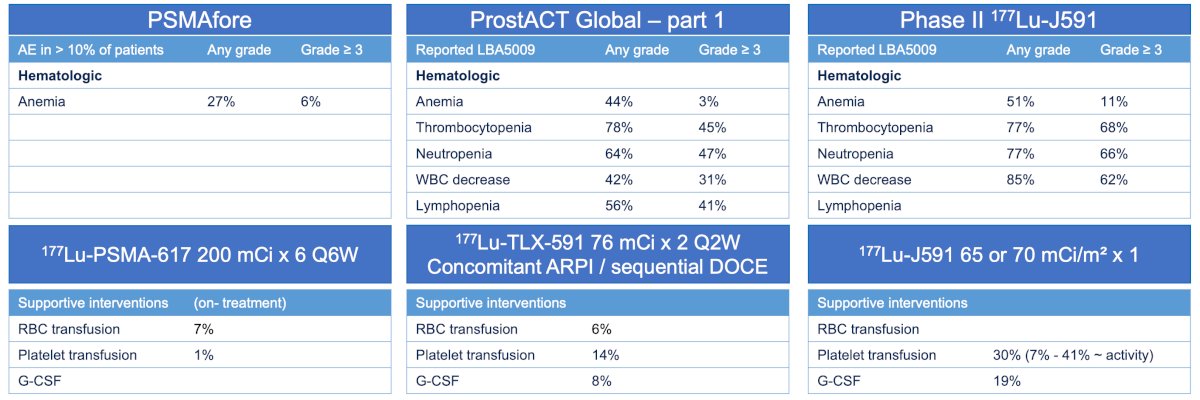
When compared with historical 177Lu-J591 data, these findings appear broadly consistent with prior antibody-based radioligand experience. In the phase II J591 study, anemia occurred in 51% of patients, thrombocytopenia in 77%, neutropenia in 77%, white blood cell decreases in 85%, and supportive care interventions included red blood cell transfusions in 6%, platelet transfusions in 14%, and G-CSF administration in 8%:
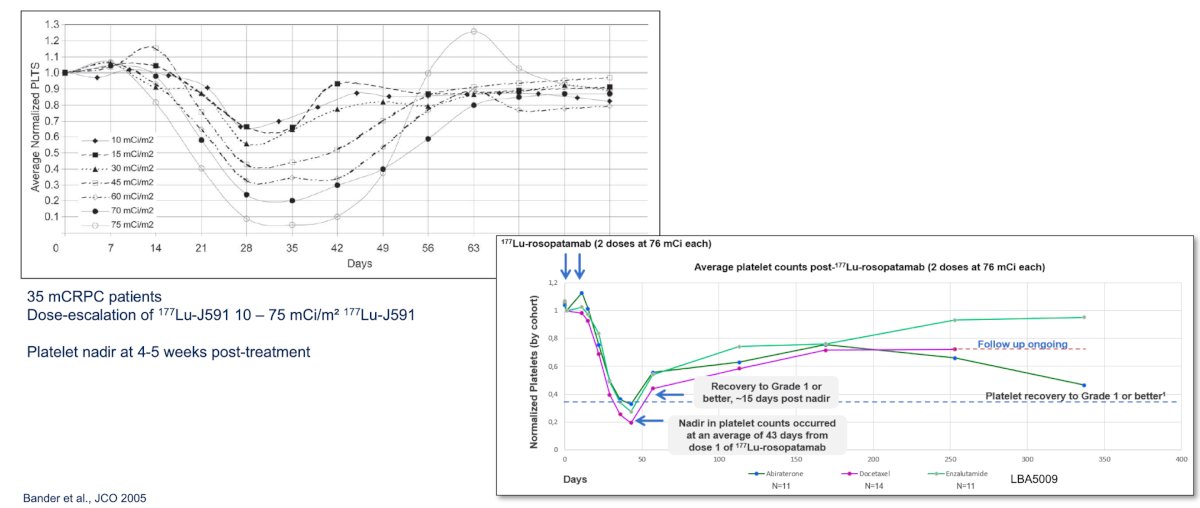
Across antibody-based PSMA radioligand programs, thrombocytopenia has emerged as a recurring toxicity. Historical dose-escalation studies with 177Lu-J591 demonstrated platelet nadirs occurring approximately 4–5 weeks following treatment administration, emphasizing the importance of careful monitoring and proactive supportive care:
Dr. Goffin concluded her discussant presentation with the following take-home points:
- 177Lu-TLX591 represents a novel PSMA-targeted radioligand therapy approach for patients with mCRPC
- The biodistribution and toxicity profile of 177Lu-TLX591 differ substantially from currently available small-molecule PSMA-directed radioligand therapies, making management of hematologic toxicity a critical consideration
- ProstACT Global is the first phase III trial evaluating a radio-antibody drug conjugate strategy in prostate cancer
Presented by: Karolien Goffin, MD, PhD, University Hospitals Leuven, KU Leuven, Leuven, Belgium
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.
- Armstrong AJ, Sartor O, de Bono J, et al. Association of declining prostate-specific antigen levels with clinical outcomes in patients with metastatic castration-resistant prostate cancer receiving [177Lu]Lu-PSMA-617 in the phase 3 VISION trial. Eur Urol. 2024 Dec;86(6):552-562.
- Tagawa ST, Milowsky MI, Morris M, et al. Phase II study of Lutetium-177-labeled anti-prostate-specific membrane antigen monoclonal antibody J591 for metastatic castration-resistant prostate cancer. Clin Cancer Res. 2013 Sep 15;19(18):5182-5191.
- Tagawa ST, Vallabhajosula S, Christos PJ, et al. Phase 1/2 study of fractionated dose lutetium-177-labeled anti-prostate-specific membrane antigen monoclonal antibody J591 (177Lu-J591) for metastatic castration-resistant prostate cancer. Cancer. 2019 Aug 1;125(15):2561-2569.