(UroToday.com) The 2026 ASCO annual meeting featured an optimizing care for patients with metastatic castration resistant prostate cancer (mCRPC) session and a presentation by Dr. Karim Fizazi discussing that one size does not fit all for first-line treatment for mCRPC. Dr. Fizazi began by highlighting the molecular heterogeneity of mCRPC, noting that seminal genomic work has demonstrated that advanced prostate cancer encompasses multiple biologically distinct disease states. This heterogeneity mandates individualized treatment approaches rather than a “one-size-fits-all” strategy.
Dr. Fizazi subsequently presented a practical algorithm for treatment decision making in mCRPC. Following confirmation of castration resistant disease, defined by testosterone <0.5 ng/mL and evidence of disease progression, patients should undergo comprehensive imaging and NGS testing. According to Dr. Fizazi, the results of genomic profiling divide patients into three broad clinical categories:
- Those with informative NGS findings
- Those with clinically indolent disease and non-informative NGS results
- Those with aggressive disease and non-informative NGS results

For patients in whom NGS identifies actionable alterations, there are several examples where molecular findings directly influence treatment selection. Homologous recombination repair (HRR) alterations, particularly BRCA1 and BRCA2 mutations, support the use of PARP inhibitors and potentially platinum chemotherapy. Patients with microsatellite instability-high (MSI-H) or mismatch repair-deficient (dMMR) tumors may benefit from immune checkpoint inhibition. Emerging evidence also suggests that androgen receptor mutations and PTEN loss may inform future therapeutic strategies.
With regards to PARP inhibitors, TRITON-31 evaluated rucaparib in patients with HRR-mutated mCRPC, including BRCA1/2 and ATM alterations. Patients with BRCA1/2 had a PFS benefit with rucaparib versus control (HR 0.50, 95% CI 0.36-0.69), whereas those with ATM alterations did not have a PFS benefit with rucaparib (HR 0.95, 95% CI 0.59-1.52):
![With regards to PARP inhibitors, TRITON-3 [1] evaluated rucaparib in patients with HRR-mutated mCRPC, including BRCA1/2 and ATM alterations. Patients with BRCA1/2 had a PFS benefit with rucaparib versus control (HR 0.50, 95% CI 0.36-0.69), whereas those with ATM alterations did not have a PFS benefit with rucaparib (HR 0.95, 95% CI 0.59-1.52):](/images/com-doc-importer/271-asco-2026/asco-2026-first-line-metastatic-castration-resistant-prostate-cancer-one-size-doesnt-fit-all/image-1.jpg)
TALAPRO-22 demonstrated improved outcomes with enzalutamide + talazoparib in the BRCA population, showing a radiographic progression-free survival benefit (HR 0.26, 95% CI 0.16-0.42) as well as in HRR non-BRCA altered (HR 0.65, 95% CI 0.47-0.91) mCRPC:

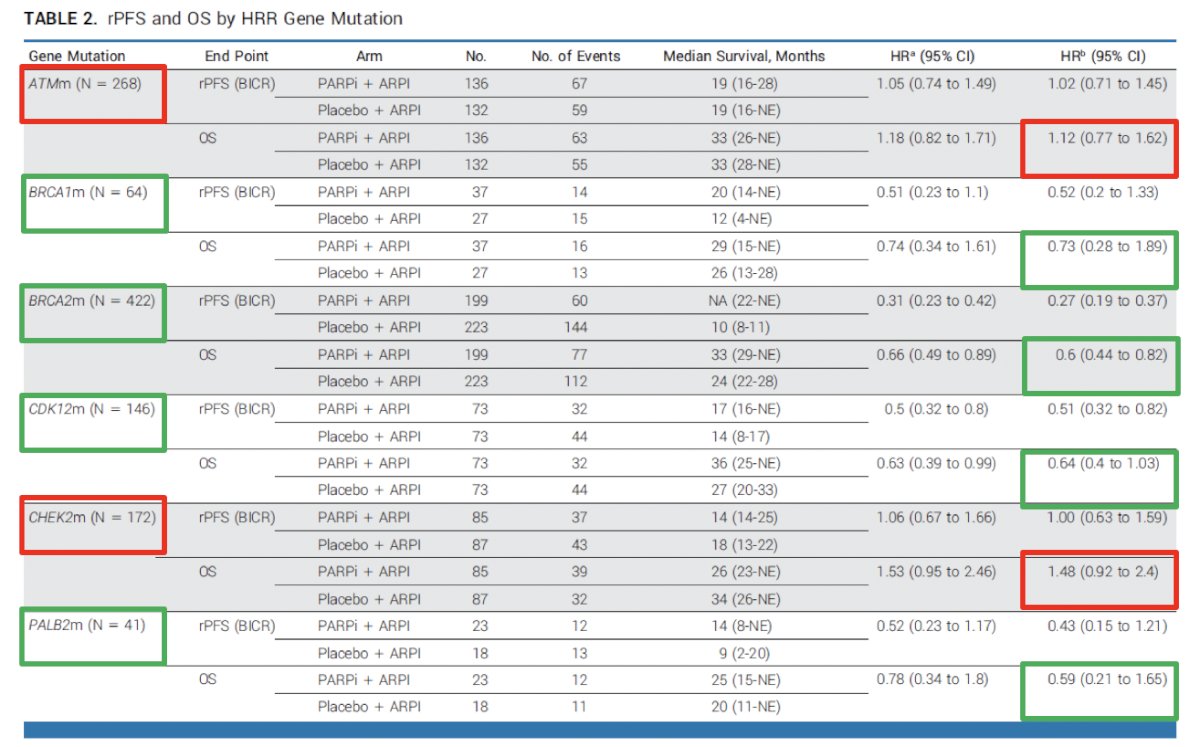
Importantly, the FDA analyses evaluating overall survival according to individual gene alterations have reinforced that the magnitude of benefit varies considerably across molecular subgroups (BRCA1, BRCA2, CKD12, and PALB2),3 emphasizing the importance of precise genomic characterization:
Immune checkpoint inhibition represents another example of biomarker-driven therapy. Dr. Fizazi noted that MSI-high disease remains uncommon in mCRPC, occurring in approximately 3% of patients. Data from Abida and colleagues4 demonstrated PSA50 responses in 53% of patients treated with PD-1/PD-L1 inhibitors, with many experiencing durable responses. More recently, Van Wilpe et al.5 reported outcomes among 68 patients with post-ARPI and post-docetaxel mCRPC, including 21 patients with dMMR disease treated with ipilimumab plus nivolumab. In this cohort, PSA50 responses reached 86%, highlighting the activity of immunotherapy in appropriately selected patients:
![Immune checkpoint inhibition represents another example of biomarker-driven therapy. Dr. Fizazi noted that MSI-high disease remains uncommon in mCRPC, occurring in approximately 3% of patients. Data from Abida and colleagues [4] demonstrated PSA50 responses in 53% of patients treated with PD-1/PD-L1 inhibitors, with many experiencing durable responses. More recently, Van Wilpe et al. [5] reported outcomes among 68 patients with post-ARPI and post-docetaxel mCRPC, including 21 patients with dMMR disease treated with ipilimumab plus nivolumab. In this cohort, PSA50 responses reached 86%, highlighting the activity of immunotherapy in appropriately selected patients:](/images/com-doc-importer/271-asco-2026/asco-2026-first-line-metastatic-castration-resistant-prostate-cancer-one-size-doesnt-fit-all/image-4.jpg)
Androgen receptor mutations emerge in approximately 20% of patients with mCRPC. Dr. Fizazi reviewed the biologic mechanisms underlying common alterations, such as AR L702H and AR T878A mutations, which may allow activation of the androgen receptor pathway through corticosteroids and progesterone:

A new therapy, opevesostat (ODM-208), inhibits the first step of steroidogenesis, targeting CYP11A1. CYPIDES was the first-in-human phase 1 (3 + 3 design) and phase 2 study,6 administering ODM-208 twice daily with glucocorticoid/mineralocorticoid replacement and ongoing ADT to adults with previously treated mCRPC, regardless of androgen receptor gene ligand-binding domain mutations (phase 1) and with activating androgen receptor ligand-binding domain mutations (phase 2). Overall, there were 92 patients who received one or more doses of ODM-208: 47 in phase 1 (42.6% with an activating androgen receptor ligand-binding domain mutation) and 45 in phase 2. Treatment-related adrenal insufficiency was the most common toxicity in phase 1 (n = 17, 36.2%; necessitating ODM-208 discontinuation in one patient). Adrenal insufficiency occurred in six patients (13.3%) at 5 mg twice a day in phase 2. A PSA50 response occurred in 14 of 19 (73.7%) patients with an activating androgen receptor ligand-binding domain mutation, and 2 of 23 (8.7%) patients with an androgen receptor wild type in phase 1, and in 24 of 45 (53.3%) patients with an activating androgen receptor ligand-binding domain mutation in phase 2:
![A new therapy, opevesostat (ODM-208), inhibits the first step of steroidogenesis, targeting CYP11A1. CYPIDES was the first-in-human phase 1 (3 + 3 design) and phase 2 study [6], administering ODM-208 twice daily with glucocorticoid/mineralocorticoid replacement and ongoing ADT to adults with previously treated mCRPC, regardless of androgen receptor gene ligand-binding domain mutations (phase 1) and with activating androgen receptor ligand-binding domain mutations (phase 2). Overall, there were 92 patients who received one or more doses of ODM-208: 47 in phase 1 (42.6% with an activating androgen receptor ligand-binding domain mutation) and 45 in phase 2. Treatment-related adrenal insufficiency was the most common toxicity in phase 1 (n = 17, 36.2%; necessitating ODM-208 discontinuation in one patient). Adrenal insufficiency occurred in six patients (13.3%) at 5 mg twice a day in phase 2. A PSA50 response occurred in 14 of 19 (73.7%) patients with an activating androgen receptor ligand-binding domain mutation, and 2 of 23 (8.7%) patients with an androgen receptor wild type in phase 1, and in 24 of 45 (53.3%) patients with an activating androgen receptor ligand-binding domain mutation in phase 2:](/images/com-doc-importer/271-asco-2026/asco-2026-first-line-metastatic-castration-resistant-prostate-cancer-one-size-doesnt-fit-all/image-6.jpg)
Another emerging biomarker discussed was PTEN inactivity. Recent transcriptomic analyses suggest that PTEN-inactive tumors derive greater benefit from docetaxel. Data presented from Grist et al.7 reported that the Decipher RNA signature was both prognostic and predicted survival benefit from docetaxel for metastatic prostate cancer (biomarker-docetaxel interaction p = 0.039). Additionally, transcriptome-based classification of PTEN inactivation identified tumors more likely to have PTEN protein loss (p < 0.001) and metabolically perturbed metastatic prostate cancer that had shorter survival with hormone therapies (p < 0.001), but exhibited docetaxel sensitivity (biomarker-docetaxel interaction p = 0.002):
![Another emerging biomarker discussed was PTEN inactivity. Recent transcriptomic analyses suggest that PTEN-inactive tumors derive greater benefit from docetaxel. Data presented from Grist et al. [7] reported that the Decipher RNA signature was both prognostic and predicted survival benefit from docetaxel for metastatic prostate cancer (biomarker-docetaxel interaction p = 0.039). Additionally, transcriptome-based classification of PTEN inactivation identified tumors more likely to have PTEN protein loss (p < 0.001) and metabolically perturbed metastatic prostate cancer that had shorter survival with hormone therapies (p < 0.001), but exhibited docetaxel sensitivity (biomarker-docetaxel interaction p = 0.002):](/images/com-doc-importer/271-asco-2026/asco-2026-first-line-metastatic-castration-resistant-prostate-cancer-one-size-doesnt-fit-all/image-7.jpg)
Dr. Fizazi then transitioned to patients with clinically indolent mCRPC and non-informative NGS results. In this setting, treatment options remain numerous. If an ARPI has not previously been utilized, agents such as abiraterone or enzalutamide remain reasonable choices. However, he emphasized that switching from one ARPI to another generally provides limited benefit, particularly switching from enzalutamide to abiraterone. Evidence supporting this comes from a Canadian randomized phase II trial evaluating sequencing strategies of abiraterone followed by enzalutamide versus enzalutamide followed by abiraterone. Among 202 patients, activity from abiraterone following enzalutamide was limited, reinforcing concerns regarding cross-resistance between AR-targeted therapies:

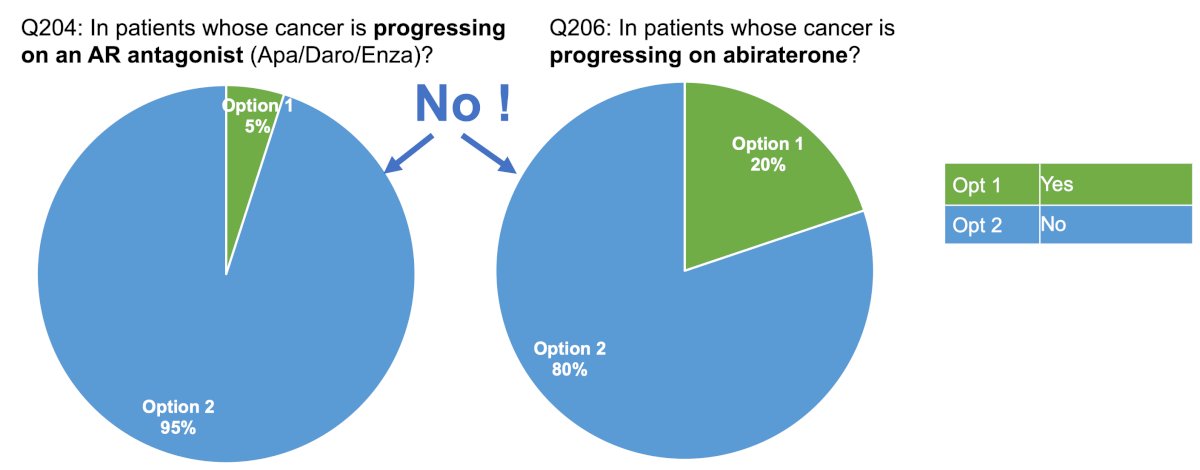
These findings were echoed by preliminary results from APCCC 2026 consensus voting. When experts were asked whether they recommend a direct ARPI switch for most asymptomatic patients progressing on abiraterone or on an AR antagonist, >80% voted against this strategy:
Several alternative options for indolent mCRPC were also reviewed. PEACE-39 demonstrated improved overall survival with enzalutamide + radium-223 compared with enzalutamide alone in patients with mCRPC, asymptomatic or mildly symptomatic bone metastases, and no visceral metastases:
![Several alternative options for indolent mCRPC were also reviewed. PEACE-3 [9] demonstrated improved overall survival with enzalutamide + radium-223 compared with enzalutamide alone in patients with mCRPC, asymptomatic or mildly symptomatic bone metastases, and no visceral metastases:](/images/com-doc-importer/271-asco-2026/asco-2026-first-line-metastatic-castration-resistant-prostate-cancer-one-size-doesnt-fit-all/image-10.jpg)
The PSMAfore phase III trial10 evaluated 177Lu-PSMA-617 versus ARPI change among taxane-naïve patients who had progressed after one prior second-generation ARPI. Eligible patients required at least one PSMA-positive metastatic lesion on PSMA PET imaging and could not have exclusionary PSMA-negative disease. The study randomized 234 patients to each treatment arm:
![The PSMAfore phase III trial [10] evaluated 177Lu-PSMA-617 versus ARPI change among taxane-naïve patients who had progressed after one prior second-generation ARPI. Eligible patients required at least one PSMA-positive metastatic lesion on PSMA PET imaging and could not have exclusionary PSMA-negative disease. The study randomized 234 patients to each treatment arm:](/images/com-doc-importer/271-asco-2026/asco-2026-first-line-metastatic-castration-resistant-prostate-cancer-one-size-doesnt-fit-all/image-11.jpg)
PSMAfore demonstrated a significant improvement in radiographic progression-free survival for 177Lu-PSMA-617: the primary analysis reported a hazard ratio of 0.41 (95% CI: 0.29–0.56; p < 0.0001), while updated analyses demonstrated a hazard ratio of 0.43 (95% CI: 0.33–0.54). The median radiographic progression-free survival improved from 5.59 months with ARPI change to 12.02 months with 177Lu-PSMA-617: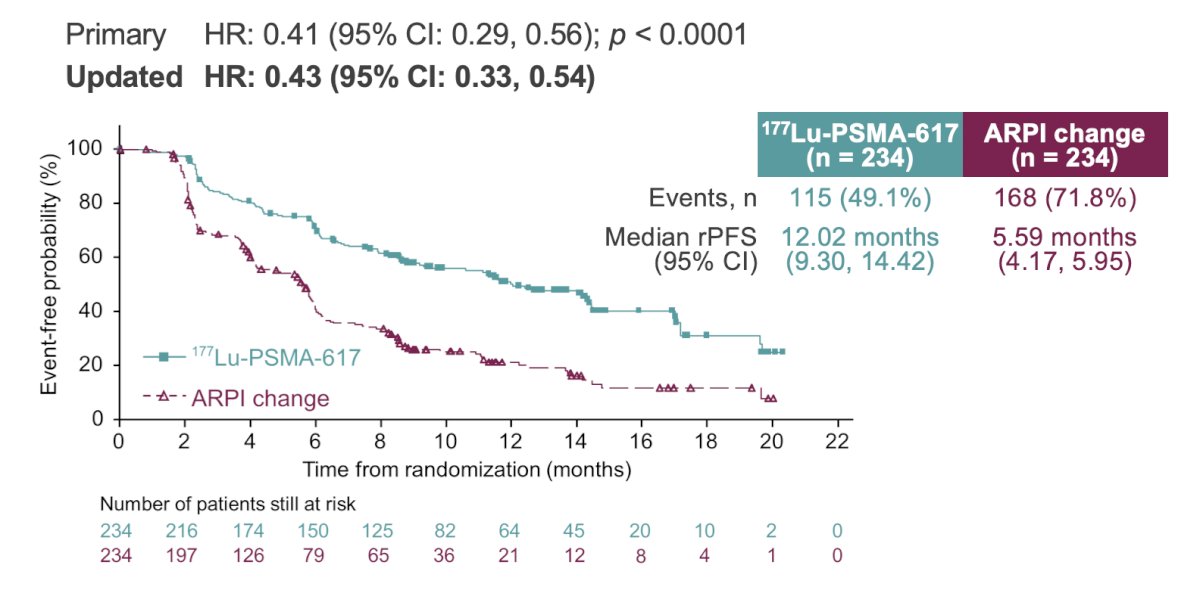
Importantly, radioligand therapy also improved patient-reported outcomes. In PSMAfore, the median time to deterioration in FACT-P total score was 9.17 months with 177Lu-PSMA-617 compared with 4.60 months following ARPI change (HR 0.48, 95% CI: 0.37–0.63). Similarly, the median time to worsening pain measured by BPI-SF improved from 4.50 months to 8.15 months (HR 0.64, 95% CI: 0.50–0.83):

Dr. Fizazi also emphasized several practical strategies for selected patients with indolent disease. Switching prednisone to dexamethasone in patients receiving abiraterone can produce clinically meaningful responses, with PSA50 responses of 20%, PSA30 responses of 40%, and a median duration of response of 28 weeks. Additionally, metastasis-directed radiotherapy continues to be explored, with the recent WOLVERINE 11 meta-analytic data from randomized trials supporting a role for MDT in selected patients (PFS HR 0.45, 95% CI 0.35-0.58):
![Dr. Fizazi also emphasized several practical strategies for selected patients with indolent disease. Switching prednisone to dexamethasone in patients receiving abiraterone can produce clinically meaningful responses, with PSA50 responses of 20%, PSA30 responses of 40%, and a median duration of response of 28 weeks. Additionally, metastasis-directed radiotherapy continues to be explored, with the recent WOLVERINE [11] meta-analytic data from randomized trials supporting a role for MDT in selected patients (PFS HR 0.45, 95% CI 0.35-0.58):](/images/com-doc-importer/271-asco-2026/asco-2026-first-line-metastatic-castration-resistant-prostate-cancer-one-size-doesnt-fit-all/image-14.jpg)
Finally, Dr. Fizazi discussed aggressive mCRPC that is not informative by NGS testing. A practical clinical definition of aggressive disease is characterized by rapidly progressive bone metastases, clinical deterioration with fatigue, anemia or pain, rapidly rising PSA, evolving bone marrow failure, neuroendocrine differentiation, suppressor gene loss including PTEN, TP53, or RB alterations, and the presence of liver metastases. For these patients, he is strongly in favor of immediate chemotherapy. Taxanes, including docetaxel and cabazitaxel, with or without platinum-based chemotherapy, remain the preferred approach.
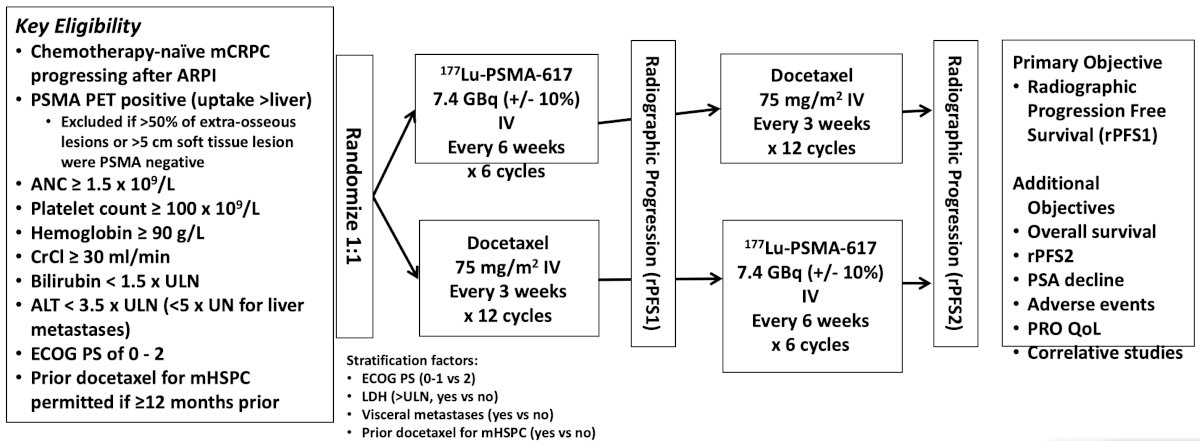
The PLUDO Canadian randomized phase II study was presented by Dr. Kim Chi at ESMO 2025 and directly compared docetaxel with 177Lu-PSMA-617 in chemotherapy-naïve mCRPC following ARPI progression. Patients were randomized to either docetaxel 75 mg/m² every three weeks for up to 12 cycles or 177Lu-PSMA-617 at 7.4 GBq every six weeks for six cycles. The primary endpoint was radiographic progression-free survival:
PLUDO reported that overall survival favored docetaxel: the median overall survival was 18.2 months among patients receiving docetaxel, followed by crossover to radioligand therapy, compared versus 14.3 months among patients receiving initial 177Lu-PSMA-617 followed by docetaxel (HR 1.64, 95% CI 1.14–2.35; p = 0.02):

This data supports the continued use of taxane chemotherapy in appropriately selected patients with aggressive disease biology. Dr. Fizazi further reinforced the value of chemotherapy by highlighting the CARD trial.12 This study enrolled patients with mCRPC who progressed within 12 months on a prior AR-targeted agent and randomized them to cabazitaxel versus an alternative ARPI:

Cabazitaxel significantly improved overall survival, achieving a median overall survival of 13.6 months compared with 11.0 months for ARPI switch (HR 0.64, 95% CI 0.46–0.89; p = 0.0078). These findings remain among the strongest evidence against routine ARPI switching following progression.
In almost all patients with mCRPC, attention is required for a patient’s comorbidities, geriatric assessment, supportive care interventions, and potential drug-drug interactions. Ongoing studies are also evaluating adjunctive therapies such as statins and low-dose aspirin, including the ongoing PEACE-4 trial. Regarding bone health, the results from PEACE-3 demonstrated a major reduction in fracture risk with the use of bone-protecting agents, particularly denosumab. Dr. Fizazi stressed that bone protective therapy should be considered standard care for patients with bone metastatic mCRPC:

Dr. Fizazi concluded his presentation discussing that one size does not fit all for first-line treatment for mCRPC with the following take-home points:
- mCRPC is a highly heterogeneous disease requiring individualized treatment strategies
- Next-generation sequencing should be routinely incorporated to identify patients who may benefit from targeted therapies or immunotherapy
- For patients with indolent disease, several effective options exist, including radioligand therapy and selected hormonal strategies
- Patients with aggressive disease biology should generally receive prompt chemotherapy-based treatment
- Regardless of treatment selection, optimization of supportive care and incorporation of bone-protecting agents remain essential components of high-quality mCRPC management
Presented by: Karim Fizazi, MD, PhD, Professor, University of Paris Saclay, President of GETUG, Head of the Genito-Urinary Group, Department of Cancer Medicine, Institut Gustave Roussy and Centre Oscar Lambret, Villejuif, France, Institut Gustave Roussy (IGR), Villejuif, France
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- Fizazi K, Piulats JM, Reaume MN, et al. Rucaparib or Physician’s Choice in Metastatic Prostate Cancer. N Engl J Med. 2023 Feb 23;388(8):719-732.
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): A randomized, placebo-controlled, phase 3 trial. Lancet. 2023 Jul 22;402(10398):291-303.
- Fallah J, Xu J, Weinstock C, et al. Efficacy of Poly(ADP-ribose) Polymerase Inhibitors by Individual Genes in Homologous Recombination Repair Gene-Mutated Metastatic Castration-Resistant Prostate Cancer: A US Food and Drug Administration Pooled Analysis. J Clin Oncol. 2024 10;42(14):1687-1698.
- Abida W, Cheng ML, Armenia J, et al. Analysis of the prevalence of microsatellite instability in prostate cancer and response to immune checkpoint blockade. JAMA Oncol. 2019 Apr 1;5(4):471-478.
- Van Wilpe S, Kloots SH, Slootbeek PHJ, et al. Ipilimumab with nivolumab in molecularly selected patients with castration-resistant prostate cancer: Primary analysis of the phase II INSPITE trial. Ann Oncol. 2024 Dec;35(12):1126-1137.
- Fizazi K, Bernard-Tessier A, Roubaud G, et al. Targeted inhibition of CYP11A1 in castration-resistant prostate cancer. NEJM Evid. 2024 Jan;3(1):EVIDoa2300171.
- Grist E, Dutey-Magni P, Parry MA, et al. Tumor transcriptome-wide expression classifiers predict treatment sensitivity in advanced prostate cancers. Cell. 2025 Oct 2;188(20):5717-5734.
- Khalaf DJ, Annala M, Taavitsainen S, et al. Optimal sequencing of enzalutamide and abiraterone acetate plus prednisone in metastatic castration-resistant prostate cancer: a multicentre, randomised, open-label, phase 2, crossover trial. Lancet Oncol. 2019l20(12):1730-1739.
- Tombal B, Choudhury A, Saad F, et al. Enzalutamide plus radium-223 in metastatic castration-resistant prostate cancer: results of the EORTC 1333/PEACE-3 trial. Ann Oncol. 2025 Sep;36(9):1058-1067.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.
- Tang C, Sherry AD, Hwang H, et al. Metastasis-directed therapy and standard of care versus standard of care for oligometastatic prostate cancer (WOLVERINE): A systematic review and individual patient data meta-analysis from the X-MET collaboration. Lancet Oncol. 2026 Feb;27(2):181-190.
- de Wit R, de Bono J, Sternberg CN, et al. Cabazitaxel versus Abiraterone or Enzalutamide in Metastatic Prostate Cancer. N Engl J Med 2019 Dec 26;381(26):2506-2518.