(UroToday.com) The 2026 ASCO annual meeting featured an artificial intelligence session and a presentation by Sebastian Medina discussing an artificial intelligence-based pathology classifier to predict benefit from enzalutamide in metastatic hormone-sensitive prostate cancer (mHSPC) from ENZAMET. Androgen receptor pathway inhibitors (ARPIs) added to ADT are the backbone of first-line treatment for mHSPC, however some patients may require more non-androgen receptor-directed therapy and cannot be identified up front.
Patients with tumors who benefit less from ARPI may be candidates for intensification with docetaxel. Thus, identifying them in practice requires a biomarker, as there is no randomized data of ADT + ARPI with or without docetaxel. mHSPC lacks accessible biomarkers to guide treatment selection, and the current options require specialty assays that are not routinely performed. H&E-stained tissue is routinely available from diagnosis and has rich morphological and spatial information, and a biomarker from H&A can be applied without additional testing.
The ENZAMET trial established that adding enzalutamide to ADT improves overall survival in mHSPC.1 However, heterogeneity in treatment response and toxicity complicates clinical decision-making. The investigator’s evaluated a previously developed Artificial Intelligence Pathology Image Classifier (APIC) to determine whether it could identify ENZAMET participants more likely to benefit from adding enzalutamide rather than non-steroidal antiandrogen to ADT.
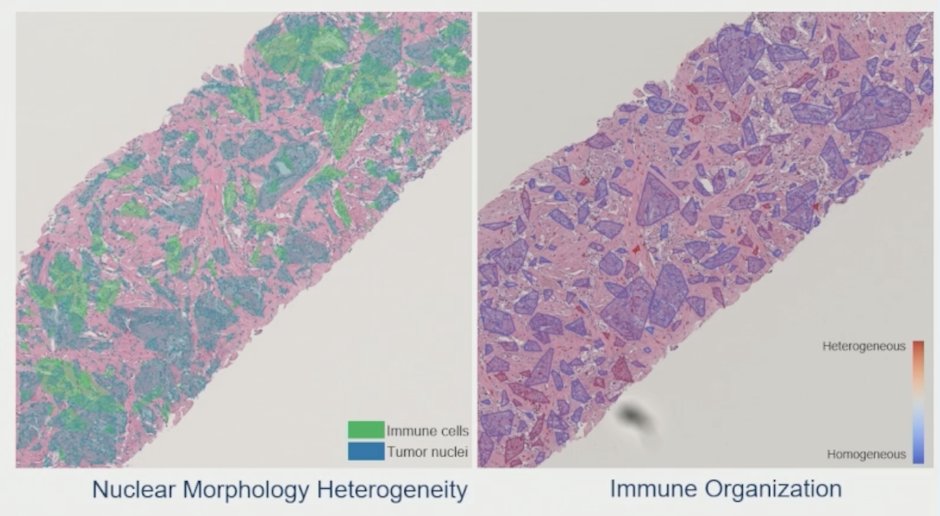
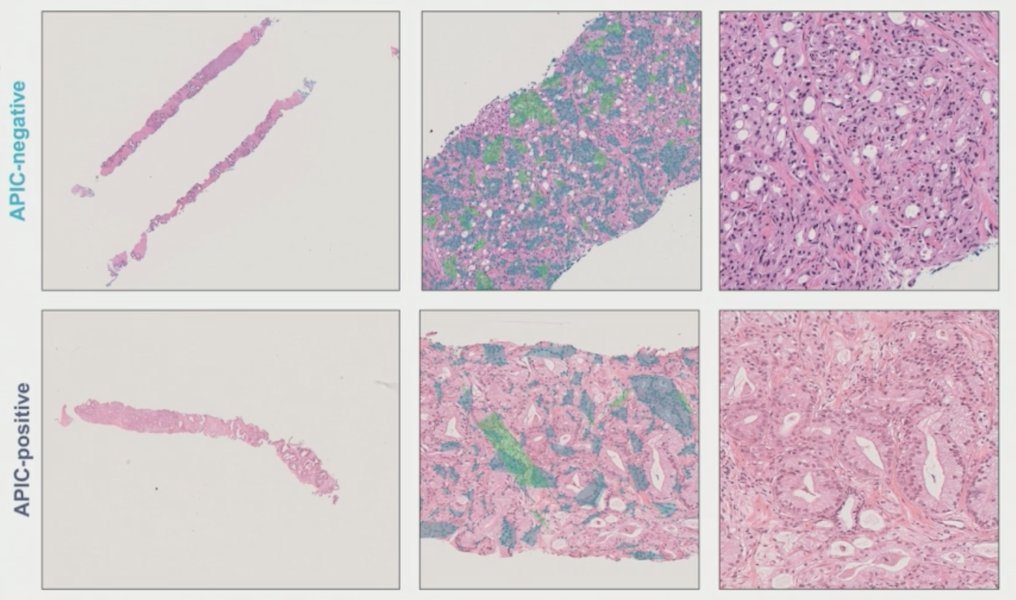
This artificial intelligence biomarker study analyzed digitized H&E tumor specimens from ENZAMET (ANZUP 1304), a phase 3 trial randomizing participants with mHSPC to ADT + enzalutamide or a non-steroidal antiandrogen, with early docetaxel permitted. APIC, a model quantifying nuclear morphology and tumor immune architecture validated in CHAARTED,2 was applied without modification:
The primary multivariable analysis evaluated the treatment-APIC interaction for overall survival using Cox models adjusted for disease volume (CHAARTED criteria), early docetaxel, and age. Sensitivity analyses excluded participants receiving early docetaxel. APIC associations with 18 circulating immune markers were explored.
The ENZAMET biomarker cohort had no significant differences between the intention-to-treat trial and the studied cohorts. Patients receiving triplet therapy were more likely to have high-volume synchronous disease: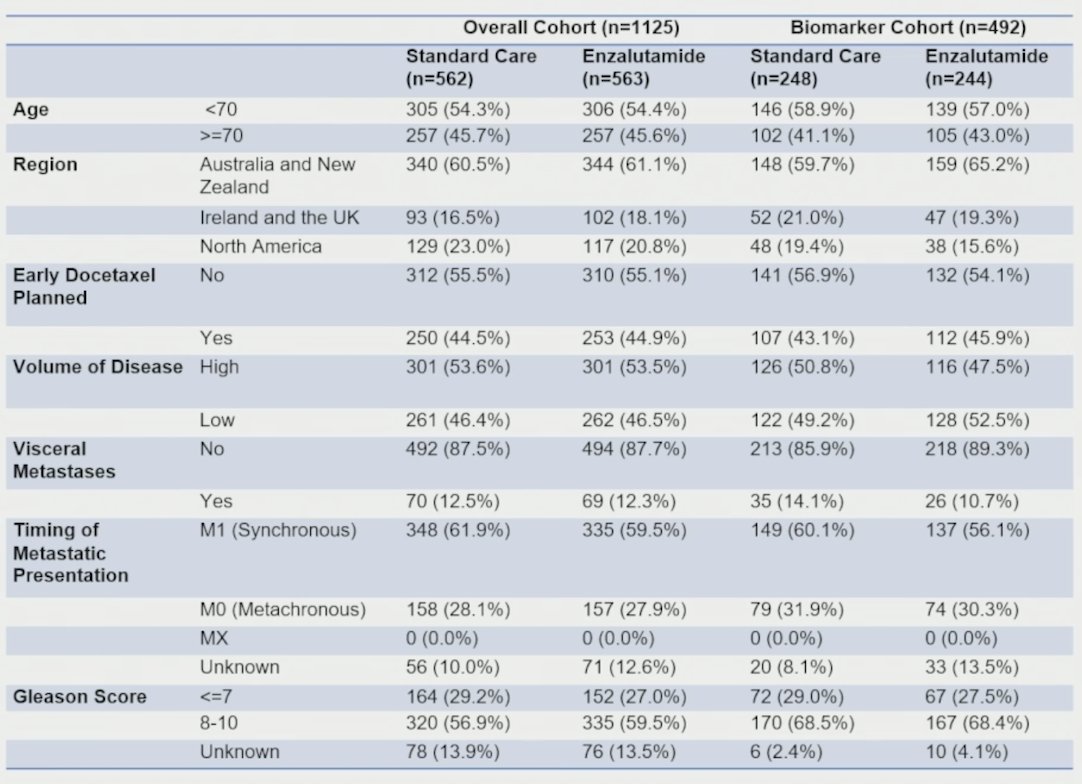
Among 492 evaluable participants, 316 (64%) were APIC-negative and 176 (36%) APIC-positive. APIC-negative was associated with improved overall survival with enzalutamide versus non-steroidal antiandrogen (HR 0.50, 95% CI 0.35-0.73), while APIC-positive showed no benefit to the addition of enzalutamide (HR 1.04, 95% CI 0.67-1.62):

Thus, APIC identified 64% of patients who could have avoided treatment intensification with a non-androgen receptor-directed therapy.
Excluding early docetaxel use, APIC-negative was also associated with enzalutamide benefit (HR 0.40, 95% CI 0.23-0.69), while no significant benefit was observed for APIC-positive addition of enzalutamide (HR 0.79, 95% CI 0.43-1.46):
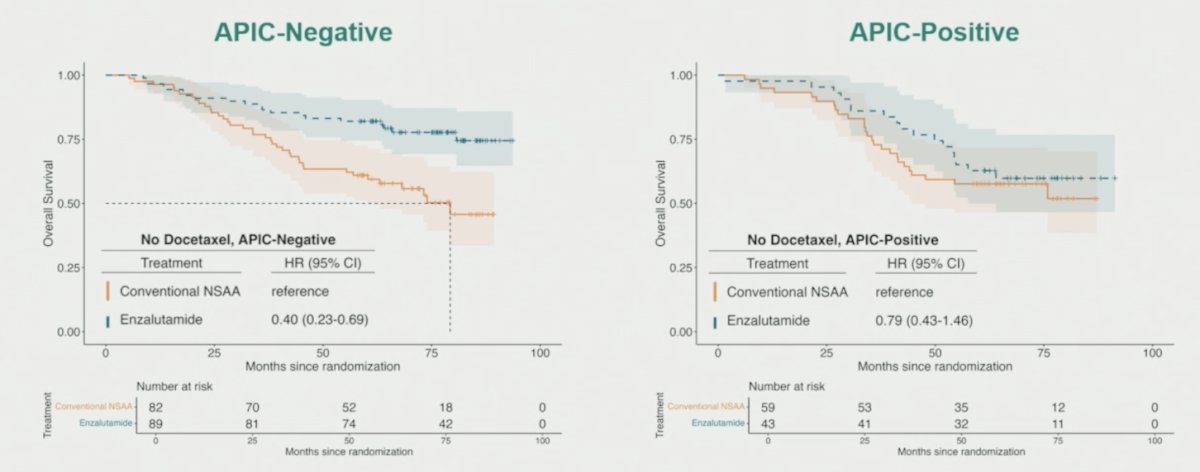
Sebastian Medina emphasized that this means that the APIC-negative benefit was not explained by early concurrent docetaxel. Additionally, there was a significant treatment-biomarker interaction, with the treatment effect most pronounced in low volume APIC-negative disease (p < 0.001):

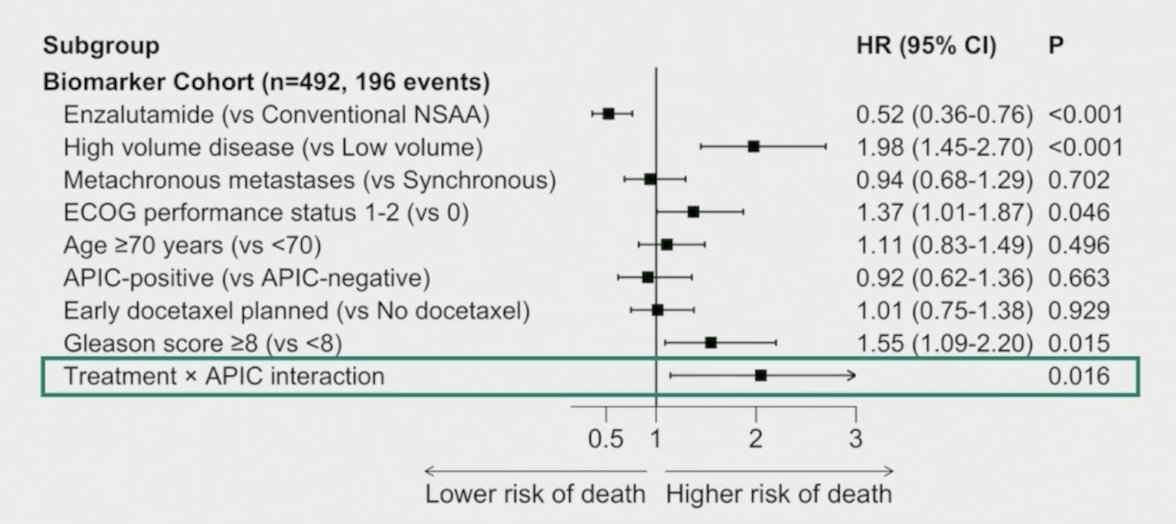
In multivariable analysis, the biomarker-treatment interaction (p = 0.016) held after adjustment for standard clinical prognostic factors such as disease volume, timing of metastases, performance status, and Gleason score:
Participants with APIC-negative disease showed higher immune infiltrates on H&E:
Further, participants with APIC-positive disease had elevated plasma myeloid progenitor inhibitor factor 1, which was associated with a poor prognosis. As such, a poor prognosis and limited enzalutamide benefit in APIC-positive disease may be associated with an immune-cold phenotype:

There were several limitations with this analysis, including:
- The biomarker cohort represented 43.7% of ENZAMET - inclusion criteria were mainly determined by tissue availability, and unmeasured selection bias cannot be excluded
- APIC was developed in CHAARTED, where ARPIs were not standard care
▪ Performance in populations with prior ARPI exposure warrants further investigation - There was limited ethnic diversity in ENZAMET and CHAARTED, and validation in cohorts with greater representation of ancestry is needed
- Lack of randomization to docetaxel precludes determining whether APIC-positive disease benefits from adding docetaxel to enzalutamide plus ADT
Sebastian Medina concluded his presentation discussing an artificial intelligence-based pathology classifier to predict benefit from enzalutamide in mHSPC from ENZAMET with the following take-home points:
- APIC is an interpretable artificial intelligence biomarker computable from routine H&E
- APIC-negative:
▪ Is predictive of overall survival benefit from ADT + enzalutamide
▪ Identified participants who may not require treatment intensification
- APIC-positive:
▪ Defines a poor prognostic group who may benefit from the addition of non-androgen receptor-directed therapy
▪ Should be interpreted alongside the prior CHAARTED finding that APIC-positive disease did benefit from adding docetaxel to ADT
▪ Is suggestive of a subgroup that may warrant treatment intensification with docetaxel
Presented by: Sebastian R. Medina, PhD student, Emory University, Atlanta, GA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- Davis ID, Martin AJ, Stockler MR, et al. Enzalutamide with Standard First-Line Therapy in Metastatic Prostate Cancer. N Engl J Med 2019 Jul 11;381(2):121-131.
- Medina S, Tokuyama N, Hammouda K, et al. A computation pathology model to predict docetaxel benefit in localized high-risk and metastatic prostate cancer. Clin Cancer Res. 2026 Feb;32(3):645-653.