(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a prostate, testicular, and penile cancers poster session. Dr. Kevin Zarrabi presented the RiboX trial, a multicenter phase Ib/II study evaluating the safety and efficacy of the CDK4/6 inhibitor ribociclib in combination with enzalutamide in patients with androgen receptor pathway inhibitor-resistant metastatic prostate cancer (mAPMR).
The rationale for the study was based on the observation that retinoblastoma (RB) function is frequently attenuated through hyperphosphorylation. Since RB activity can potentially be reactivated through inhibition of CDK4/6, the investigators hypothesized that combining ribociclib with enzalutamide may enhance antitumor activity in patients with ARPI-resistant disease while retaining RB expression.
RiboX was a multicenter, open-label phase Ib/II trial that enrolled taxane-naïve patients with progression to mAPMR and confirmed RB expression on tumor biopsy. During the phase Ib dose-escalation portion, patients received ribociclib at 200 mg, 400 mg, or 600 mg once daily on days 1–21 in combination with fixed-dose enzalutamide 160 mg daily on days 1–28. No dose-limiting toxicities were observed, and the recommended phase II dose (RP2D) was established as ribociclib 600 mg once daily on days 1–21 plus enzalutamide 160 mg daily.
The phase II portion was initially designed as a randomized study comparing enzalutamide monotherapy versus enzalutamide plus ribociclib. However, due to changes in the treatment landscape during enrollment, the study was amended to a single-arm Simon two-stage design utilizing the RP2D combination regimen. The primary endpoint was the proportion of patients achieving a PSA50 response at 12 weeks. The null hypothesis was that the PSA50 response rate would be <78%, and 31 PSA50 responses were required to reject the null hypothesis. Secondary endpoints included radiographic progression-free survival (rPFS), PSA progression-free survival (PSA-PFS), overall survival (OS), and safety.
A total of 12 patients were enrolled in the phase Ib dose-escalation cohort. For the phase II portion, 12 patients received enzalutamide monotherapy, while 28 phase II patients plus 6 phase Ib patients treated at the RP2D yielded a total of 34 patients treated with ribociclib plus enzalutamide. Four patients in the combination arm were evaluable for PSA-PFS but did not have data available for rPFS analyses.
The primary endpoint was not met. The PSA50 response rate at 12 weeks was 75% (9/12 patients; 95% CI: 43–95) in the enzalutamide monotherapy arm and 82% (28/34 patients; 95% CI: 65–93) in the ribociclib plus enzalutamide arm, failing to reject the prespecified null hypothesis. Waterfall plot analyses demonstrated substantial PSA declines in both treatment groups, with the majority of patients experiencing some degree of PSA reduction from baseline.

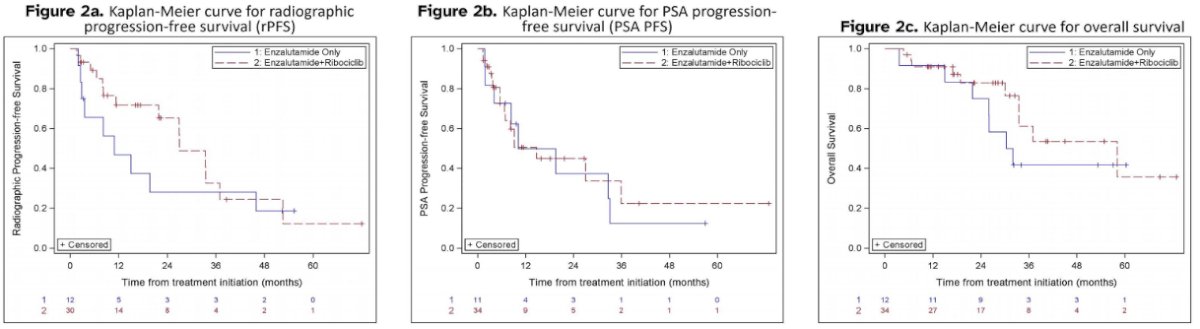
Despite not meeting the primary endpoint, encouraging signals were observed across several time-to-event outcomes. Median rPFS was 10.9 months (95% CI: 2.5–45.9) among patients treated with enzalutamide alone and 27.0 months (95% CI: 11.3–37.0) among evaluable patients receiving ribociclib plus enzalutamide. Kaplan-Meier analyses demonstrated prolonged disease control in a subset of patients treated with the combination regimen.
Similarly, median PSA-PFS was 10.1 months (95% CI: 1.8–33.1) with enzalutamide monotherapy and 14.8 months (95% CI: 6.7–35.9) with ribociclib plus enzalutamide.
The median OS was 31.2 months (95% CI: 15.0–not available) among patients receiving enzalutamide alone compared with 58.1 months (95% CI: 33.4–not available) among patients treated with ribociclib plus enzalutamide. The Kaplan-Meier OS curves demonstrated durable long-term survival in a subset of patients receiving combination therapy.
The combination regimen was generally well tolerated. Among patients treated at the RP2D, the most common treatment-emergent adverse events were:
- Fatigue (59%)
- Nausea (26.9%)
- Neutropenia (26.7%)
- Diarrhea (20.9%)
- Dizziness (14.7%)
- Arrhythmia (2.9%)
- Seizure (2.9%)
Grade 3 neutropenia occurred in 12% of patients. No unexpected safety signals were identified.
The investigators concluded that ribociclib plus enzalutamide was well tolerated but did not significantly improve PSA50 response rates, and the primary endpoint was not met. However, a disease-stabilizing effect was observed in a subset of patients receiving combination therapy, with evidence of prolonged rPFS and OS. The authors suggested that further investigation of this disease-stabilizing effect and refinement of patient-selection strategies beyond RB expression may be warranted.
Presented by: Kevin K. Zarrabi, MD, MS, FACP, Medical Oncologist, Thomas Jefferson University, Philadelphia, PA, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026