(UroToday.com) The 2026 ASCO annual meeting featured a plenary session and a presentation by Dr. Mary-Ellen Taplin discussing the final analysis of PROTEUS, a phase 3 trial of perioperative apalutamide + ADT versus placebo + ADT with radical prostatectomy in high-risk localized or locally advanced prostate cancer.
Dr. Taplin began by highlighting the significant unmet need in high-risk localized prostate cancer. Despite refinement of radical prostatectomy as a curative-intent approach, more than half of patients with high-risk disease ultimately relapse, often requiring additional therapy and experiencing associated morbidity.1,2 She noted that the development of metastatic disease is associated with poor prognosis, with a median time from metastasis to death historically reported at approximately 3–5 years.
She further emphasized that apalutamide has already demonstrated clinical activity in both mCSPC and mCRPC3 and has shown encouraging activity in the neoadjuvant setting in prior phase II studies.4,5 These observations provided the rationale for the PROTEUS trial, designed to evaluate whether the addition of neoadjuvant and adjuvant apalutamide plus ADT to radical prostatectomy could improve pathologic response and long-term clinical outcomes compared with placebo plus ADT.
Dr. Taplin then reviewed the PROTEUS trial design, a randomized, double-blind, placebo-controlled phase III study in patients with high-risk localized or locally advanced prostate cancer. She emphasized that PROTEUS represents the largest therapeutic trial ever conducted in localized prostate cancer, enrolling patients across 18 countries with a racially diverse population. Importantly, the study successfully accrued during the global COVID-19 pandemic after opening in 2019. A total of 2,109 patients were randomized 1:1 to receive neoadjuvant apalutamide 240 mg daily plus ADT versus placebo plus ADT for six cycles prior to radical prostatectomy, followed by adjuvant apalutamide plus ADT versus placebo plus ADT for an additional six cycles after surgery. Study therapy was briefly held around the time of prostatectomy and subsequently resumed postoperatively. The study design is presented below:
Patients were stratified by nodal status, Gleason score, and geographic region. Dr. Taplin highlighted that metastasis-free survival was selected as a coprimary endpoint at the time the study was designed, when conventional imaging remained the standard staging modality. However, as PSMA PET/CT rapidly emerged as the preferred imaging approach for localized prostate cancer staging by 2021, the trial protocol was amended to incorporate PSMA PET imaging. Under the amended protocol, patients underwent PSMA PET imaging three months after prostatectomy, with both conventional imaging and PSMA PET performed at the time of biochemical recurrence and every six months thereafter.
Dr Taplin also discussed an important PROTEUS substudy designed to complement the main trial. In this substudy, approximately 400 patients were randomized to radical prostatectomy alone versus the full PROTEUS regimen, aiming to further define the contribution of systemic intensification with apalutamide plus ADT in the perioperative setting.
The trial incorporated dual coprimary endpoints assessed by blinded independent central review, including:
- Pathologic complete response/minimal residual disease, defined as ypT0 or ≤ypT2 disease with ≤5 mm residual tumor
- Metastasis-free survival, defined by metastatic progression identified on conventional imaging or PSMA PET imaging, histopathologic confirmation, or death.
She emphasized that the incorporation of PSMA PET into the MFS endpoint reflected the evolving imaging landscape during trial conduct and the increasing adoption of PSMA PET/CT in localized prostate cancer staging and surveillance. Secondary endpoints, tested hierarchically, included event-free survival, time to first subsequent therapy, time to distant metastasis by conventional or PSMA PET imaging, no evidence of disease at four years, metastasis-free survival by conventional imaging alone, and time to PSA-free survival with testosterone recovery. Additional exploratory endpoints included residual cancer burden, overall survival for no detriment of treatment, and testosterone recovery to >200 ng/dL.
The study was powered at 94% for the pCR/MRD endpoint and 85% for MFS, with two-sided alpha allocations of 0.01 and 0.04, respectively. The final MFS analysis was event-driven and planned after approximately 477 metastasis-free survival events, with 472 events ultimately observed. Importantly, she noted that the statistical design allowed alpha allocated to the pCR/MRD endpoint to be recycled to MFS if both pCR/MRD and event-free survival achieved statistical significance. Under this hierarchical testing strategy, because pCR/MRD and EFS were both statistically significant at the 0.01 level, metastasis-free survival and subsequent secondary endpoints were formally tested hierarchically at the adjusted alpha threshold of 0.0416.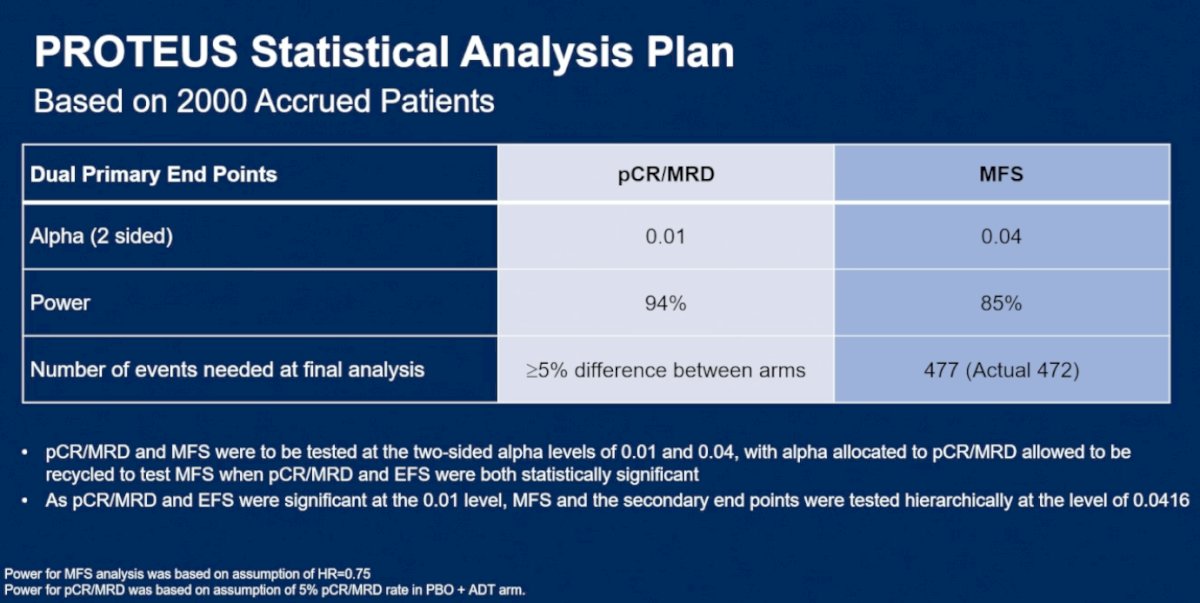
Dr. Taplin noted that baseline characteristics were well balanced between treatment arms, as shown in the table below. Median patient age was 66 years in both groups, with approximately 10% of patients aged ≥75 years. Importantly, she emphasized that this was a very high-risk study population: nearly 40% of patients had a baseline PSA ≥20 ng/mL, approximately 35% had clinical stage ≥T3 disease at diagnosis, and about 12% demonstrated evidence of nodal involvement on conventional imaging. In addition, over 95% of patients had a Gleason score ≥8 disease at diagnosis.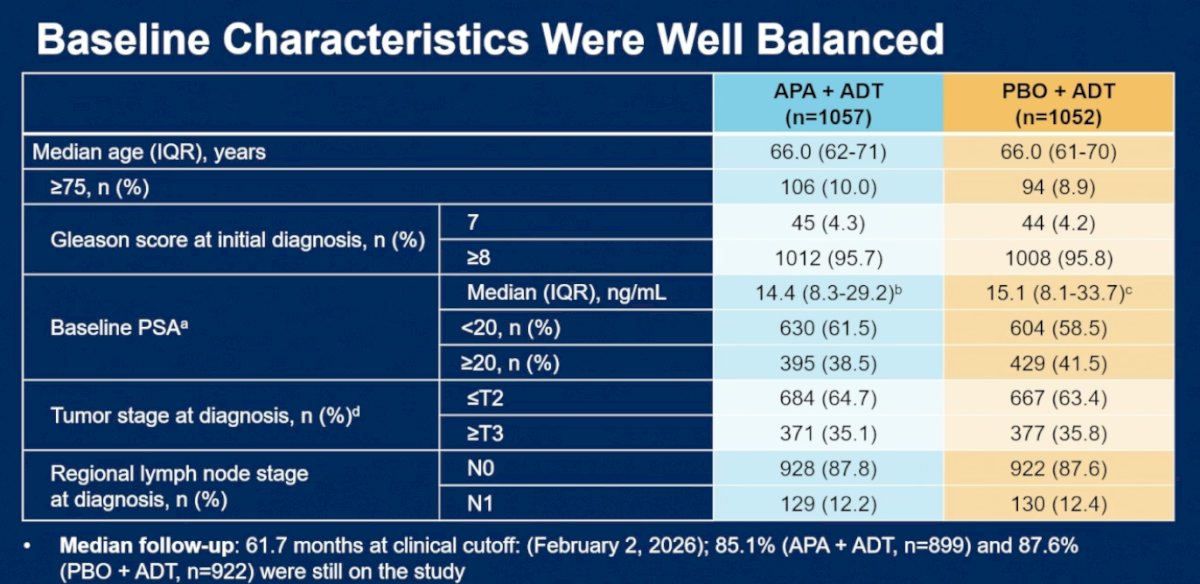
At the clinical cutoff date of February 2, 2026, median follow-up was 61.7 months. Dr. Taplin highlighted that a large proportion of patients remained on study at the time of analysis, including 85.1% in the apalutamide plus ADT arm and 87.6% in the placebo plus ADT arm.
The PROTEUS trial met its dual coprimary endpoint of pathologic complete response/minimal residual disease (pCR/MRD). Treatment with neoadjuvant apalutamide plus ADT resulted in a 9-fold improvement in pCR/MRD rates at the time of radical prostatectomy compared with placebo plus ADT, with pCR/MRD achieved in 8.9% versus 1.0% of patients, respectively (OR 10.17; 95% CI 5.27–19.64; p<0.0001).
Complete pathologic response (ypT0) rates were 5.1% with apalutamide plus ADT versus 0.4% with placebo plus ADT.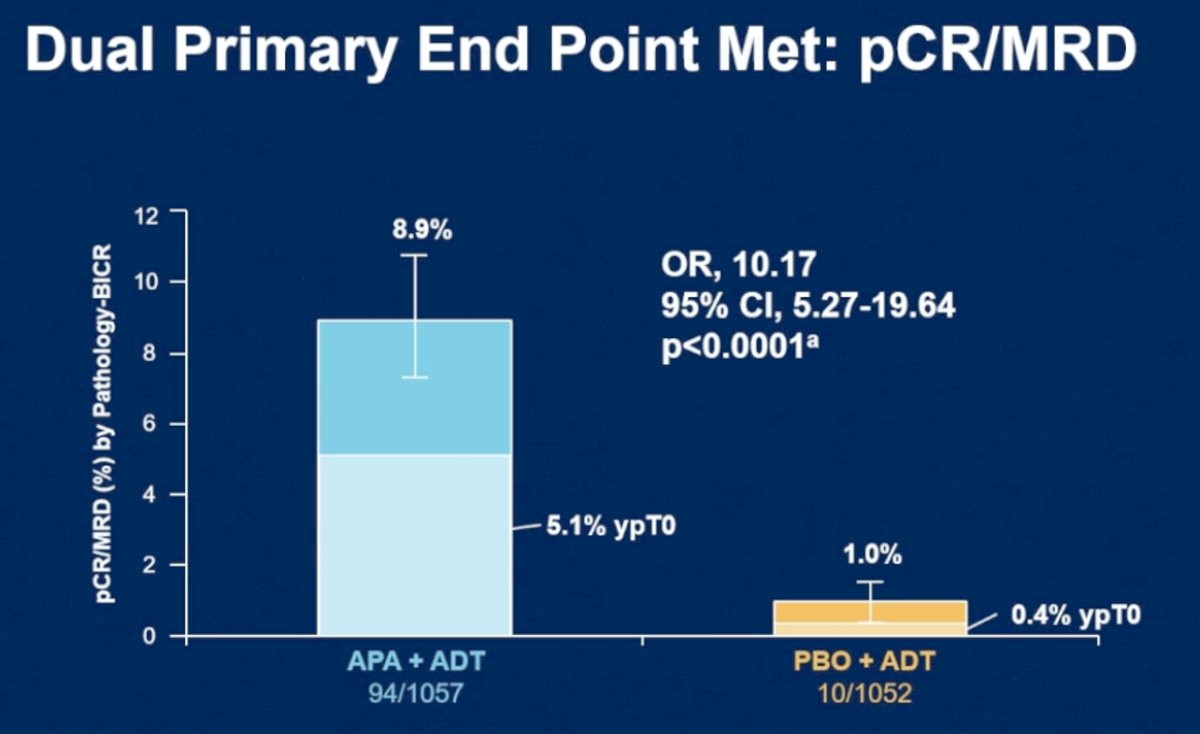
Dr. Taplin highlighted that these findings were further corroborated by the exploratory residual cancer burden endpoint, defined as ≤ypT2, N0 disease with residual tumor ≤0.25 cm³. Residual cancer burden responses were observed in 30.6% of patients receiving apalutamide plus ADT compared with 11.7% in the placebo plus ADT arm (OR 3.36; 95% CI 2.67–4.23; p<0.0001), further supporting the substantial pathologic downstaging achieved with intensified perioperative systemic therapy.
The PROTEUS trial also met its second dual coprimary endpoint of metastasis-free survival by conventional or PSMA PET imaging. Perioperative treatment with apalutamide plus ADT in combination with radical prostatectomy resulted in a 20% reduction in the risk of metastasis or death compared with placebo plus ADT (HR 0.80; 95% CI 0.67–0.96; p=0.02). Dr. Taplin emphasized that this benefit emerged despite the already intensive multimodality management received by these very high-risk patients. She further highlighted that investigator-assessed metastasis-free survival findings were consistent with the blinded independent central review analysis, demonstrating an even greater relative benefit favoring apalutamide plus ADT (HR 0.74; 95% CI 0.62–0.87; p=0.0004).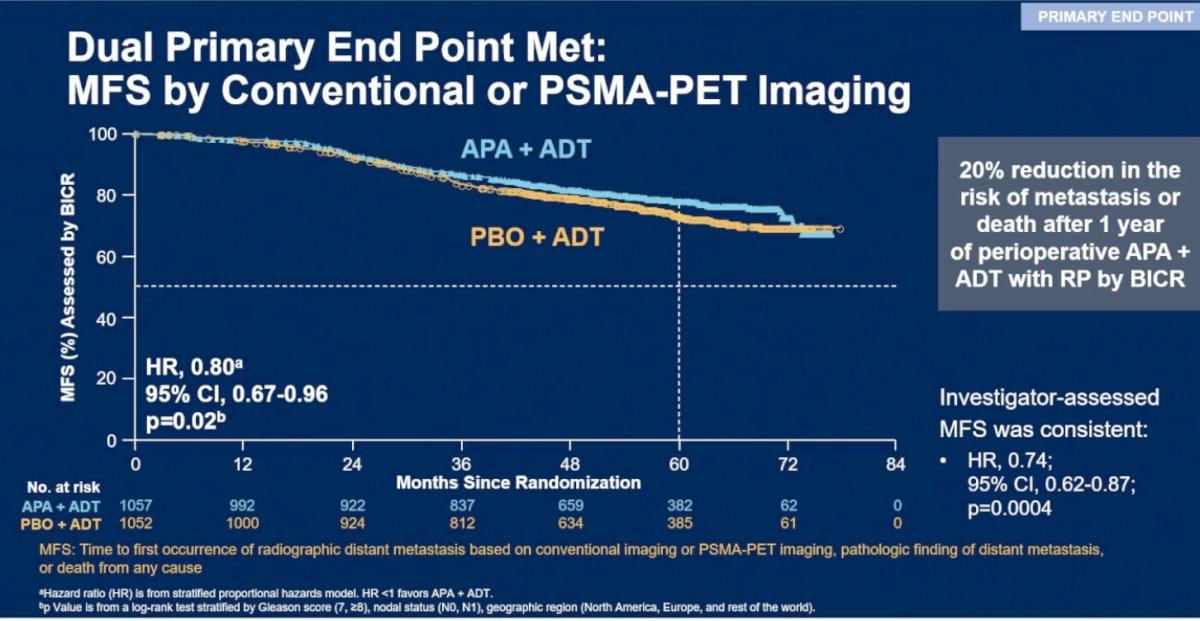
Secondary endpoints
Event-free survival was also significantly improved with perioperative apalutamide plus ADT. Dr. Taplin highlighted a 29% reduction in the risk of oncologic events or death compared with placebo plus ADT (HR 0.71; 95% CI 0.63–0.80; p<0.0001). Median event-free survival was prolonged from 38.4 months in the placebo plus ADT arm to 57.1 months with apalutamide plus ADT, representing a clinically meaningful improvement in disease control for this high-risk population.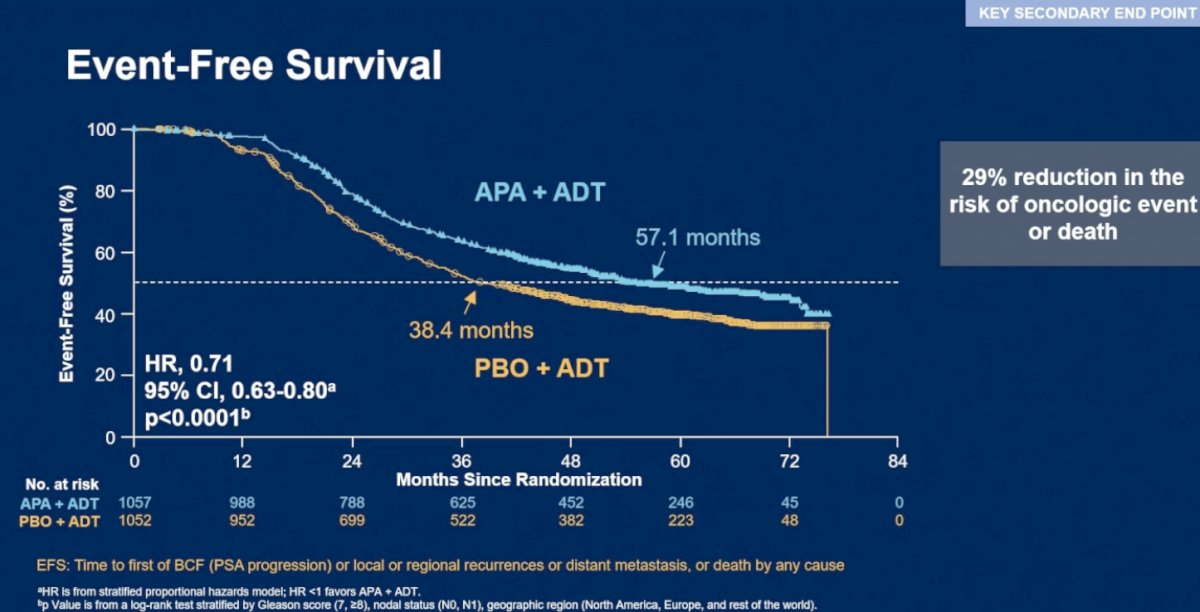
Time to first subsequent therapy was also significantly prolonged with perioperative apalutamide plus ADT. Dr. Taplin highlighted that patients receiving combination therapy experienced a nearly 3-year longer treatment-free interval compared with placebo plus ADT. Median time to first subsequent therapy was 74.2 months in the apalutamide plus ADT arm versus 41.5 months in the placebo plus ADT arm, corresponding to a 35% reduction in the risk of requiring subsequent local or systemic therapy, including reinitiation of ADT (HR 0.65; 95% CI 0.57–0.73; p<0.0001).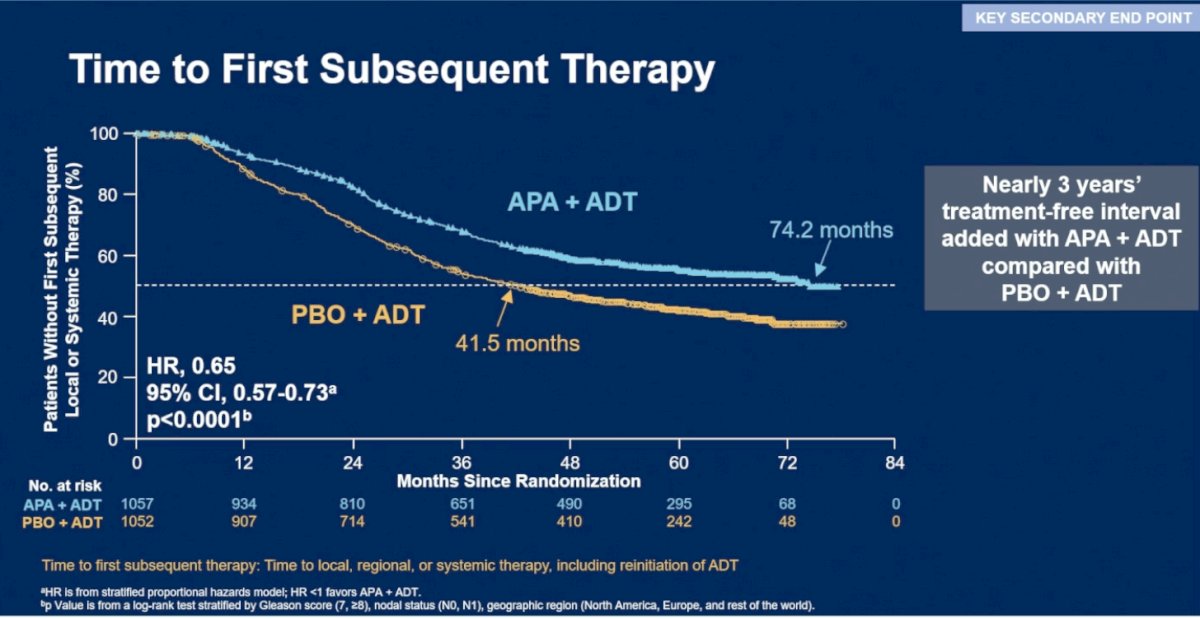
Dr. Taplin further detailed the types of subsequent therapies received after disease progression or recurrence. Overall, fewer patients in the apalutamide plus ADT arm required additional treatment compared with placebo plus ADT (42.4% vs 56.7%). This difference was primarily driven by lower rates of subsequent systemic therapy (26.7% vs 36.4%) and postoperative radiotherapy (13.0% vs 18.4%) in the apalutamide-treated cohort. Rates of other radiotherapy and subsequent surgery were low and generally similar between treatment arms.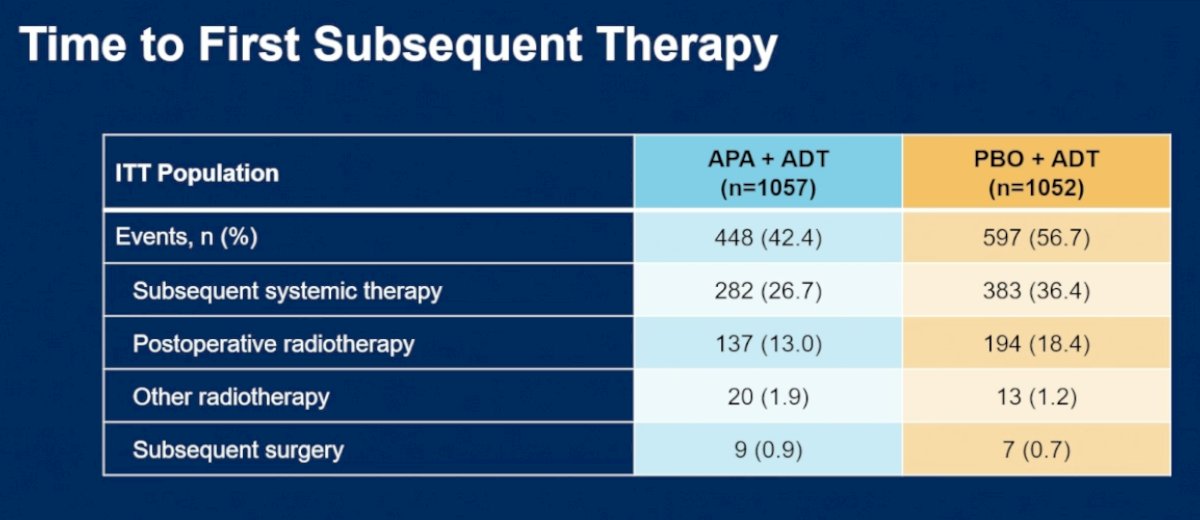
Time to distant metastasis was significantly improved with perioperative apalutamide plus ADT. Dr. Taplin highlighted a 32% reduction in the risk of developing distant metastatic disease compared with placebo plus ADT (HR 0.68; 95% CI 0.55–0.83; p=0.0002). Importantly, at 5 years, 82.8% of patients treated with apalutamide plus ADT remained free of distant metastases compared with 76.2% in the placebo plus ADT arm.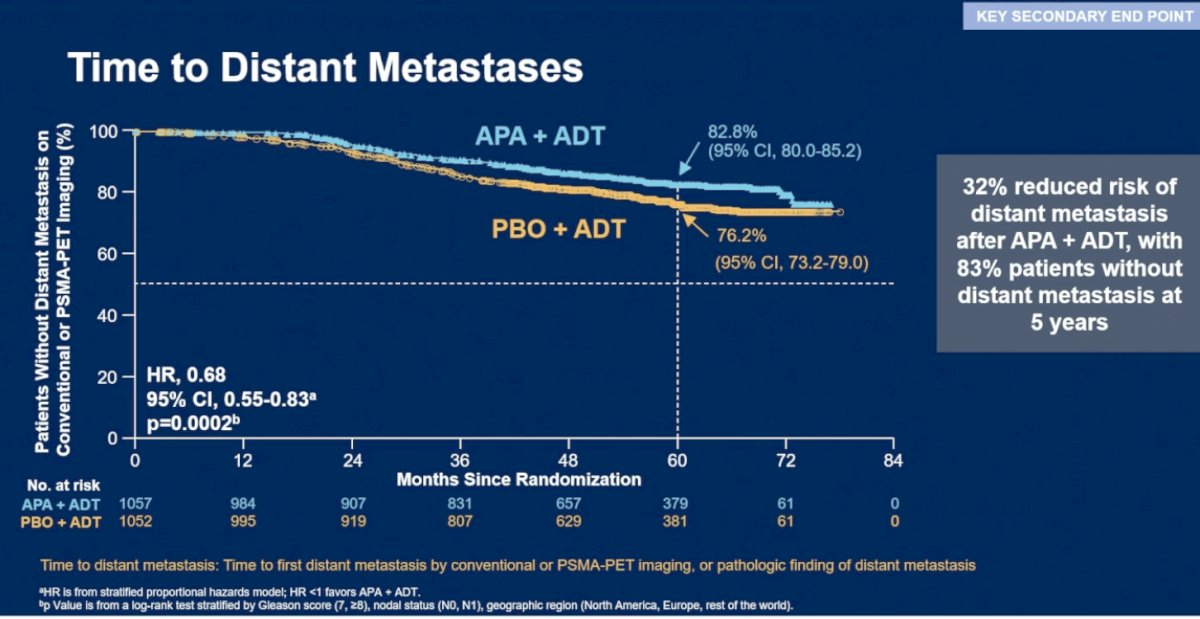
Notably, metastasis-free survival by conventional imaging alone did not reach statistical significance (HR 0.84; 95% CI 0.67–1.07; p=0.15). Dr. Taplin emphasized that the incorporation of PSMA PET imaging likely contributed to earlier detection of metastatic disease and earlier initiation of subsequent therapies, which may have affected conventional imaging-based metastasis-free survival analyses. Nevertheless, at 5 years, 87.1% of patients in the apalutamide plus ADT arm remained metastasis-free by conventional imaging compared with 83.9% in the placebo plus ADT arm.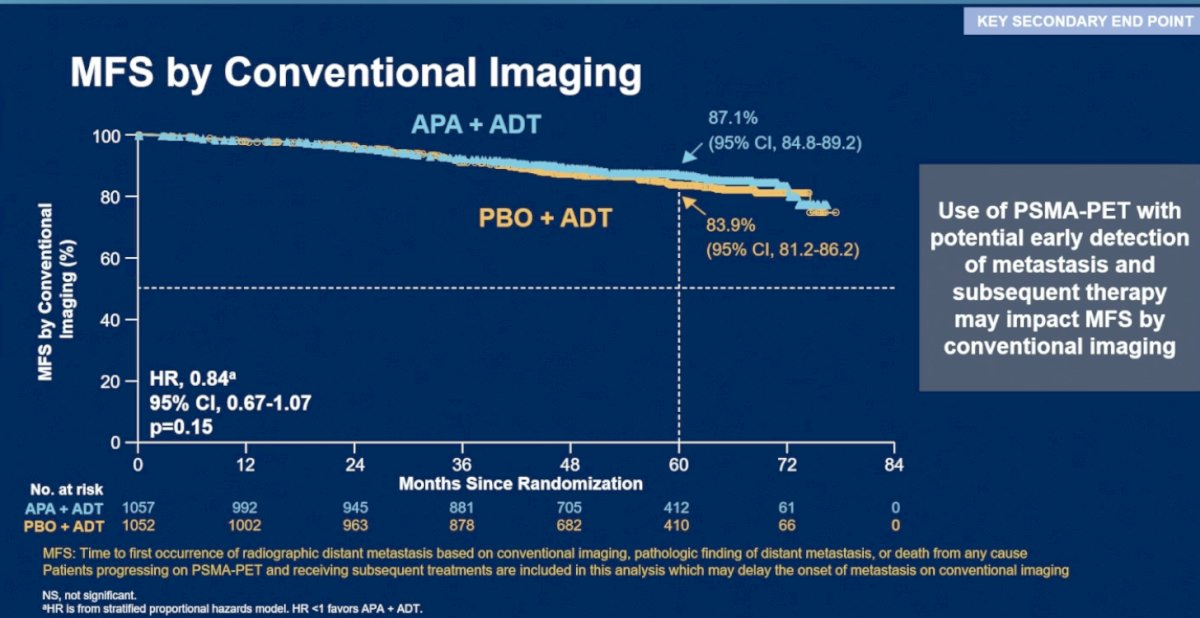
Dr. Taplin also presented testosterone recovery outcomes following completion of therapy. Among patients who achieved testosterone recovery to ≥200 ng/dL, median testosterone levels were 270 ng/dL (range, 200–1797) in the apalutamide plus ADT arm compared with 290 ng/dL (range, 200–1134) in the placebo plus ADT arm. Median time from end of treatment to testosterone recovery was 8.1 months with apalutamide plus ADT versus 6.6 months with placebo plus ADT.
Overall, testosterone recovery to ≥200 ng/dL was achieved in the majority of patients in both groups, occurring in 81.6% of patients receiving apalutamide plus ADT and 83.0% receiving placebo plus ADT.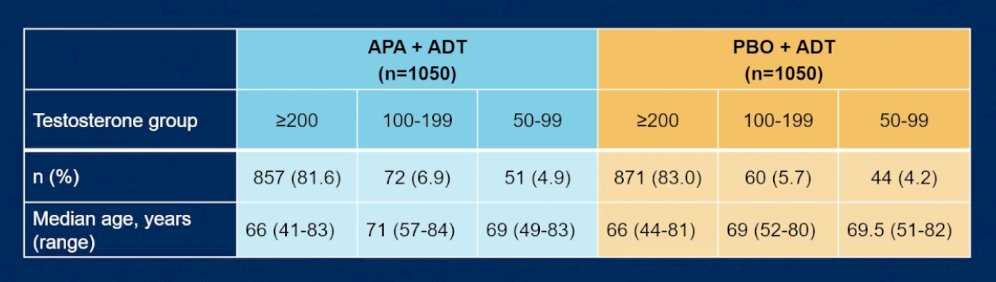
Treatment-related adverse events of any grade occurred frequently in both groups, reported in 95.2% of patients receiving apalutamide plus ADT and 93.8% receiving placebo plus ADT. However, grade 3/4 treatment-related adverse events were more common with apalutamide intensification (27.5% vs 18.9%).
Treatment-related adverse events leading to dose reduction and treatment interruption were also more frequent in the apalutamide arm, occurring in 11.2% and 12.0% of patients, respectively, compared with 2.3% and 4.4% in the placebo arm. Treatment-related adverse events leading to death were uncommon overall, although numerically higher with apalutamide plus ADT (0.7% vs 0.1%).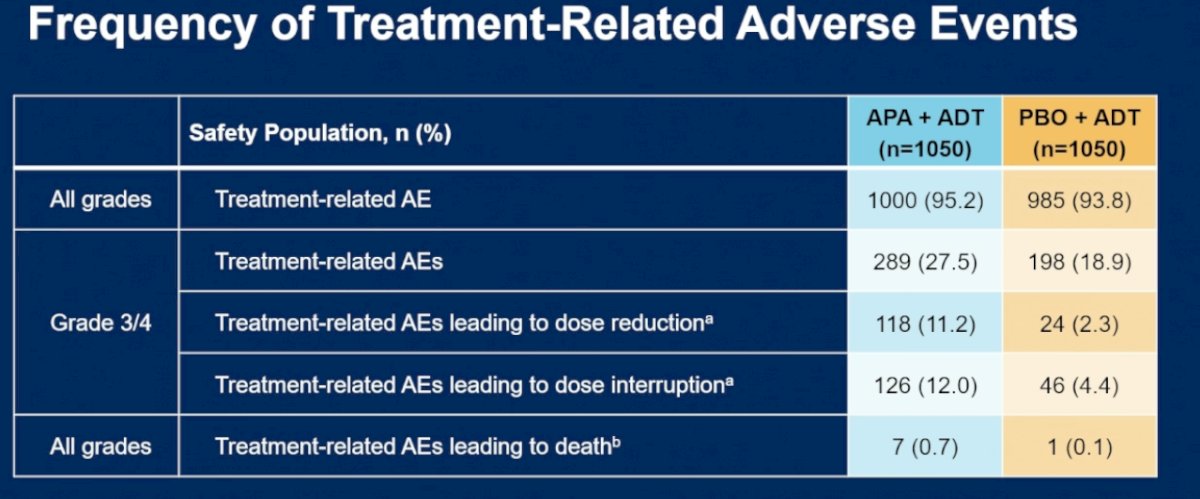
Notably, skin rash was an important adverse event associated with apalutamide. Rash events were more common in the apalutamide plus ADT arm, although the majority were manageable with supportive care measures, dose interruptions, and dose reductions when necessary. She emphasized that despite the increased incidence of rash, overall treatment discontinuation rates remained relatively low, and the safety profile was considered manageable within the context of the substantial efficacy benefits observed with perioperative apalutamide intensification.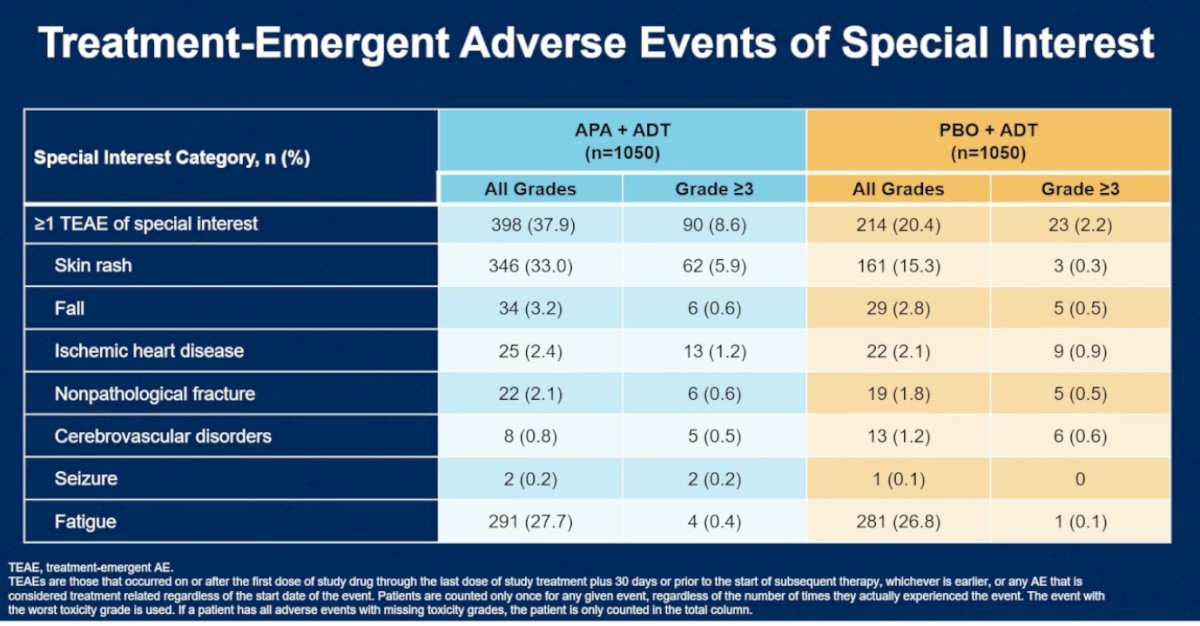
Dr. Taplin concluded her presentation discussing the final analysis of PROTEUS with the following take-home points:
- PROTEUS establishes a new standard of care for patients with high-risk localized prostate cancer
- She emphasized that PROTEUS represents an unprecedented study design in localized prostate cancer, being the largest therapeutic trial conducted to date in this disease space, while also incorporating novel endpoints and PSMA PET imaging into the trial design
- Perioperative apalutamide plus ADT significantly enhanced disease control after radical prostatectomy, including:
- A 9-fold improvement in pCR/MRD rates
- A 20% reduction in the risk of metastasis or death
- A 29% reduction in the risk of recurrence or death
- Nearly 3 additional years before requiring subsequent therapy
- Dr. Taplin noted that the safety profile and tolerability of apalutamide plus ADT were consistent with prior studies evaluating apalutamide in advanced prostate cancer settings
- She also highlighted that additional analyses from PROTEUS are still ongoing, including:
- The substudy directly comparing the PROTEUS regimen with radical prostatectomy alone
- Biomarker analyses
- Surgical outcome assessments
- Pathologic correlatives
Concurrent publication in the NEJM: DOI: 10.1056/NEJMoa2603878
Presented by: Mary-Ellen Taplin, MD, Oncologist, Chair of Executive Committee for Clinical Research, Director of Clinical Research at Lank Center for Genitourinary Oncology, Dana-Farber Cancer Institute, Boston, MA
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Related content: PROTEUS Trial: Neoadjuvant Apalutamide and Androgen Deprivation Therapy in High-Risk Localized Prostate Cancer - Mary-Ellen Taplin
References:
- Cooley LF, Shore ND. Historic progression of prostatectomy techniques and associated outcomes. Transl Androl Urol. 2025 Mar 30;14(3):493-495. doi: 10.21037/tau-2025-3. Epub 2025 Mar 26. PMID: 40226072; PMCID: PMC11986561.
- Stattin P, Fleming S, Lin X, Lefresne F, Brookman-May SD, Mundle SD, Pai H, Gifkins D, Robinson D, Styrke J, Garmo H. Population-based study of disease trajectory after radical treatment for high-risk prostate cancer. BJU Int. 2024 Jul;134(1):96-102. doi: 10.1111/bju.16362. Epub 2024 Apr 15. PMID: 38621388.
- Chi KN, Agarwal N, Bjartell A, Chung BH, Pereira de Santana Gomes AJ, Given R, Juárez Soto Á, Merseburger AS, Özgüroğlu M, Uemura H, Ye D, Deprince K, Naini V, Li J, Cheng S, Yu MK, Zhang K, Larsen JS, McCarthy S, Chowdhury S; TITAN Investigators. Apalutamide for Metastatic, Castration-Sensitive Prostate Cancer. N Engl J Med. 2019 Jul 4;381(1):13-24. doi: 10.1056/NEJMoa1903307. Epub 2019 May 31. PMID: 31150574.
- Smith MR, Saad F, Chowdhury S, Oudard S, Hadaschik BA, Graff JN, Olmos D, Mainwaring PN, Lee JY, Uemura H, Lopez-Gitlitz A, Trudel GC, Espina BM, Shu Y, Park YC, Rackoff WR, Yu MK, Small EJ; SPARTAN Investigators. Apalutamide Treatment and Metastasis-free Survival in Prostate Cancer. N Engl J Med. 2018 Apr 12;378(15):1408-1418. doi: 10.1056/NEJMoa1715546. Epub 2018 Feb 8. PMID: 29420164.
- Giesen A, Devos G, Tosco L, Goffin K, Ahmadi Bidakhvidi N, Laenen A, Baldewijns M, Gevaert T, Petit V, Mai C, Raskin Y, Van Haute C, Goeman L, De Meerleer G, Berghen C, Devlies W, Claessens F, Van Poppel H, Everaerts W, Joniau S. Final Results of the Randomised Phase 2 Trial of Neoadjuvant Degarelix with or Without Apalutamide Prior to Radical Prostatectomy for High-risk Prostate Cancer (ARNEO). Eur Urol Oncol. 2025 Dec 29:S2588-9311(25)00331-1. doi: 10.1016/j.euo.2025.12.005. Epub ahead of print. PMID: 41469270.
- McKay RR, Xie W, Ye H, Fennessy FM, Zhang Z, Lis R, Calagua C, Rathkopf D, Laudone VP, Bubley GJ, Einstein DJ, Chang PK, Wagner AA, Parsons JK, Preston MA, Kilbridge K, Chang SL, Choudhury AD, Pomerantz MM, Trinh QD, Kibel AS, Taplin ME. Results of a Randomized Phase II Trial of Intense Androgen Deprivation Therapy prior to Radical Prostatectomy in Men with High-Risk Localized Prostate Cancer. J Urol. 2021 Jul;206(1):80-87. doi: 10.1097/JU.0000000000001702. Epub 2021 Mar 8. PMID: 33683939; PMCID: PMC9807004.