(UroToday.com) The 2026 ASCO annual meeting featured a kidney cancer rapid abstract session and a presentation by Dr. Pavlos Msaouel discussing results from a multi-institutional study assessing prospective clinical activity and preclinical basis of panitumumab-based EGFR blockade in SMARCB1-deficient renal medullary carcinoma.
Renal medullary carcinoma is a rare, exceptionally aggressive malignancy that predominantly affects young individuals of African descent with sickle cell trait. Renal medullary carcinoma is defined by loss of the SMARCB1 tumor suppressor and is typically refractory to standard kidney cancer therapies, including anti-angiogenic agents and immune checkpoint inhibitors. While cytotoxic chemotherapy is the current standard, objective response rates remain low (~29%), with a median progression-free survival of ≤ 4 months in the first-line setting.
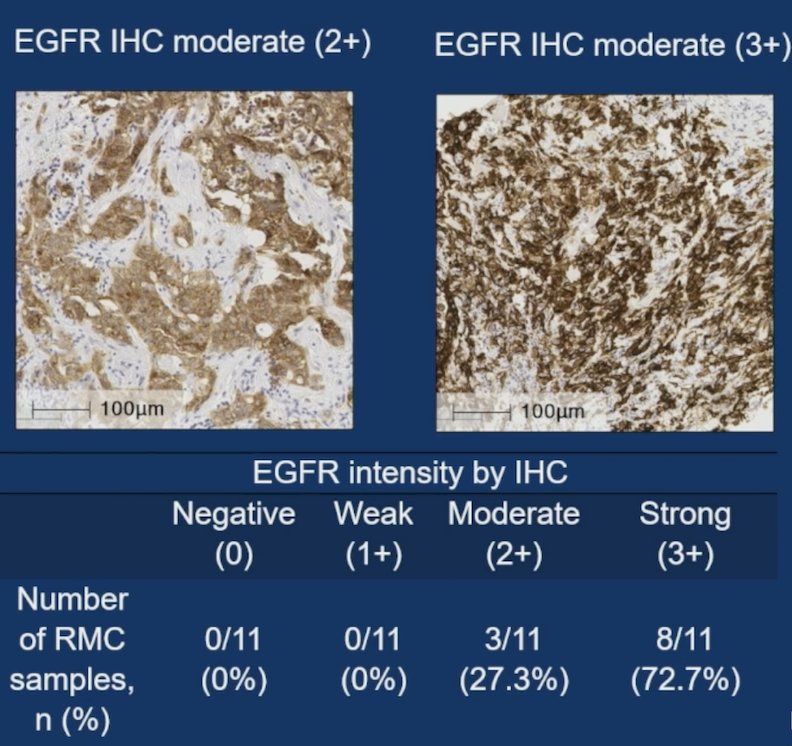
Across multiple molecular profiling studies in renal medullary carcinoma, recurrent EGFR or RAS-pathway mutations have not been observed, supporting a dependency on wild-type EGFR. In Dr. Msaouel’s work, they reported no EGFR mutations detected on WES. Renal medullary carcinoma tumors demonstrated uniformly high wild-type EGFR protein expression and enhancer-associated activation. Mechanistically, panitumumab triggered definitive lysosomal receptor degradation and suppressed AKT and ERK1/2 signaling:
Dr. Msaouel’s group noted that panitumumab (EGFR mAb) induced profound tumor regressions in two renal medullary xenograft models, significantly outperforming erlotinib (EGFR TKI). Erlotinib and other TKIs targeting the intracellular EGFR kinase domain are effective primarily in tumors such as NSCLC harboring activating EGFR kinase domain mutations. Wild-type EGFR-driven tumors, including colorectal cancer and HNSCC, respond to extracellular EGFR-blocking monoclonal antibodies such as panitumumab.
This study, presented at ASCO 2026, explored wild-type EGFR as a therapeutic dependency in renal medullary carcinoma. Following the preclinical work, a prospective multi-national registry (n = 26) evaluated panitumumab-based therapy (monotherapy or combined with nab-paclitaxel ± carboplatin) in heavily pretreated patients with renal medullary carcinoma. Among these patients, the median age was 33.5 (IQR 17, 67), and 61.5% were of black ethnicity. At treatment initiation, patients had a median of 4 metastatic disease sites (range, 2–6). The cohort was heavily pretreated with a median of 2 prior systemic therapies (range, 0–4), and 96.2% had progressed on prior platinum-based chemotherapy:

Overall, there was an observed objective response rate of 53.9% (14/26 patients), including 4 (15.4%) complete responses: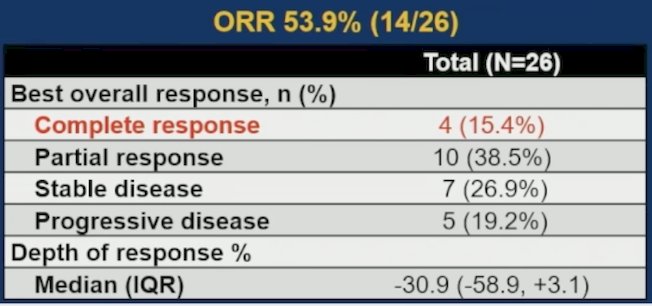

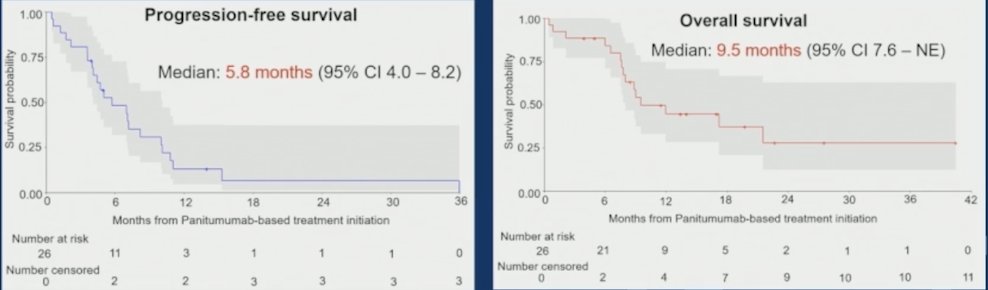
The median progression-free survival was 5.8 months (95% CI 4.0–8.2), and the median overall survival was 9.5 months (95% CI: 7.6–NE):
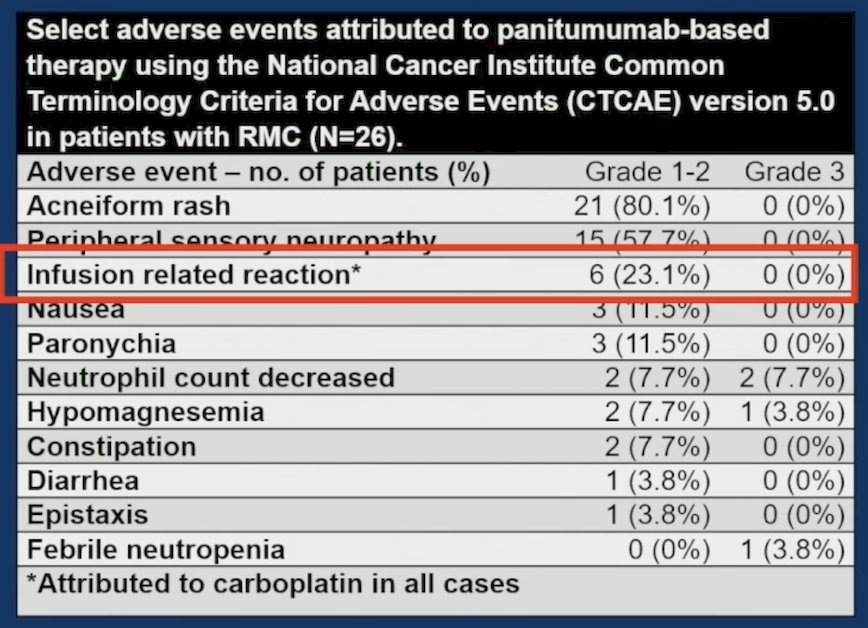
Treatment was well-tolerated, with manageable grade 1-2 acneiform rash (80.8%), no grade 3+ rash cases observed, and no treatment-related deaths:
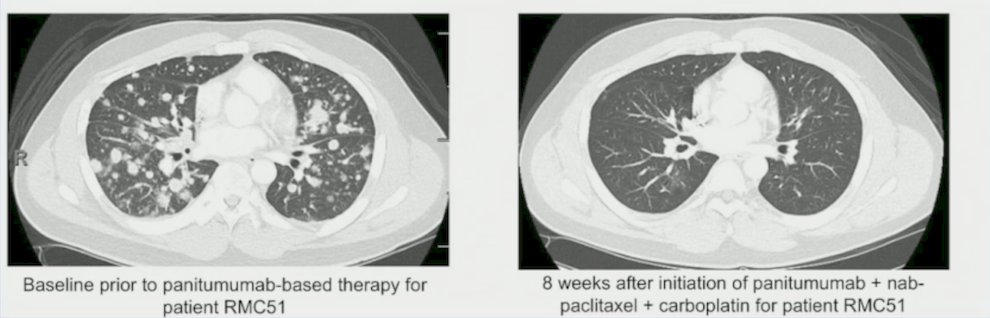
Dr. Msaouel provided the following example of effective panitumumab-based therapy in the fifth-line setting, showing before and after treatment lung CT scans:
An additional case was a renal medullary carcinoma patient with rapid progression on first-line cisplatin/carboplatin + paclitaxel + gemcitabine. The patient’s bilirubin was 24 mg/dL due to extensive metastases, including a small bowel obstruction, which resolved after two doses of panitumumab. Three months later, the bilirubin was normal, and Dr. Msaouel added nab-paclitaxel, achieving a near-complete response.
There were several limitations noted for this registry:
- It was a single arm and non-randomized
- Patients were treated off-label across multiple centers, with some heterogeneity in dosing schedules and chemotherapy backbones, and a subset of patients lacked standardized radiographic follow-up or central imaging review
- The relative contributions of panitumumab versus nab-paclitaxel cannot be definitively disentangled without randomized comparisons
Dr. Msaouel concluded this presentation discussing results from a multi-institutional study assessing prospective clinical activity and preclinical basis of panitumumab-based EGFR blockade in SMARCB1-deficient renal medullary carcinoma with the following take-home points:
- EGFR targeting with panitumumab + nab-paclitaxel is a new standard of care for renal medullary carcinoma
- Ongoing work includes identifying the mechanism of resistance to EGFR targeting:
- Phenotypic transformation
- Tumor heterogeneity
- Microenvironment upregulation of ligands/growth factors
- Bypass pathway activation/mutation
Presented by: Pavlos Msaouel, MD, PhD, The University of Texas MD Anderson Cancer Center, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026