(UroToday.com) The 2026 ASCO annual meeting featured a kidney cancer rapid abstract session and a presentation by Dr. Rahul Winayak discussing microbial dysbiosis as a predictor of benefit from CBM588 as an adjunct to immune checkpoint blockade-based first-line therapies in metastatic renal cell carcinoma (RCC).
The Clostridium butyricum-based live biotherapeutic, CBM588, demonstrated signals for enhanced clinical activity with first-line immune checkpoint blockade combinations in two randomized phase I trials for metastatic RCC. However, the impact of microbial dysbiosis on the benefit of CBM588 supplementation is unclear. At ASCO 2026, Dr. Winayak and colleagues examined the prognostic and predictive value of microbial dysbiosis with CBM588.
For this analysis, the investigators analyzed clinical outcomes and stool whole-genome sequencing data from a combined cohort from two randomized phase I clinical trials. Enrolled treatment-naïve patients with metastatic RCC were randomized to receive nivolumab/ipilimumab (NCT03829111) or nivolumab/cabozantinib (NCT05122546) alone (standard of care), or with CBM588 (standard of care + CBM588). Using stool shotgun metagenomic sequencing, Dr. Winayak derived the TOPOSCORE, a stool metagenomic dysbiosis index linked to immune checkpoint blockade outcomes, and the S-score for all patients. The TOPOSCORE was analyzed continuously (S score positively correlated with dysbiosis) and categorically (SIG1+ [dysbiosis phenotype] versus SIG2+ [non-dysbiosis]). Associations with progression-free survival and objective response rate (per RECIST 1.1) with standard of care and standard of care + CBM588 were assessed.
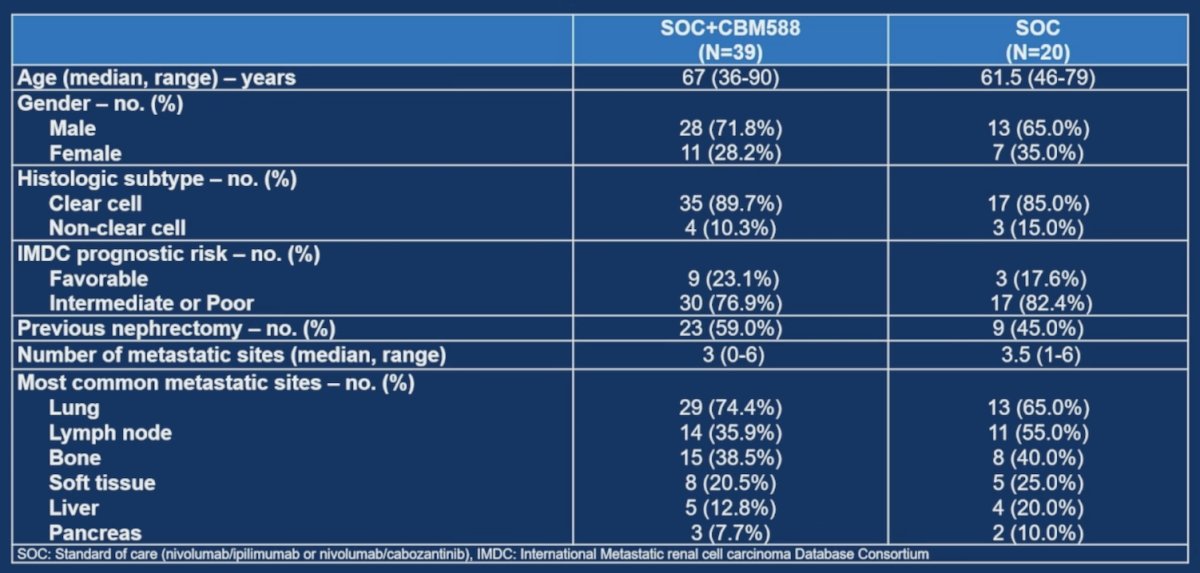
There were 59 patients included: 39 in the standard of care + CBM588 arm and 20 in the standard of care arm. The median age was 65 (range 36-90), with the majority male (69.5%), clear cell RCC (88.1%), and intermediate/poor risk (67.8%) metastatic RCC. Baseline clinical characteristics were comparable across arms:
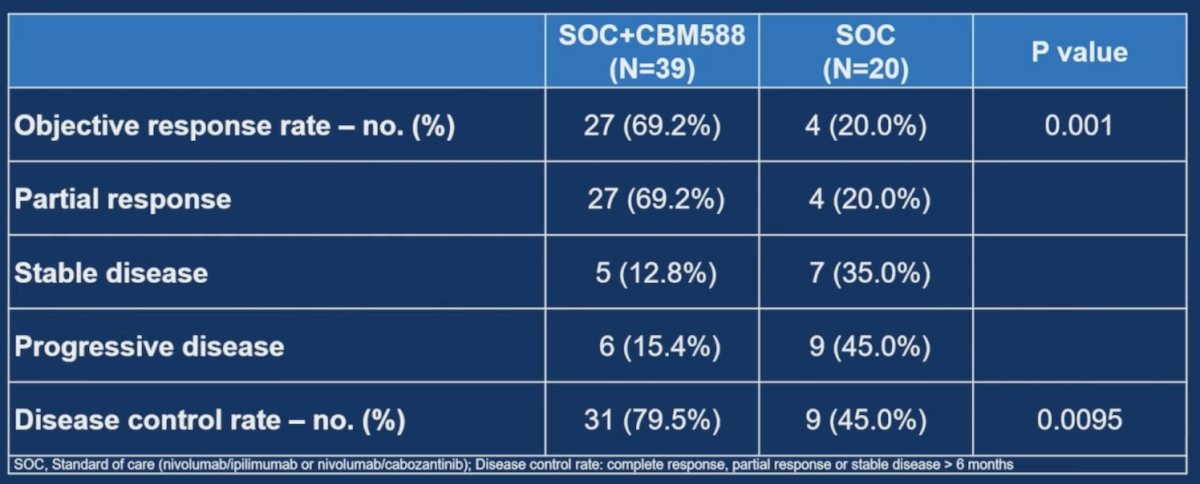
The objective response rate was 69.2% in the standard of care + CBM588 arm versus 20.0% in the standard of care arm (p = 0.001):
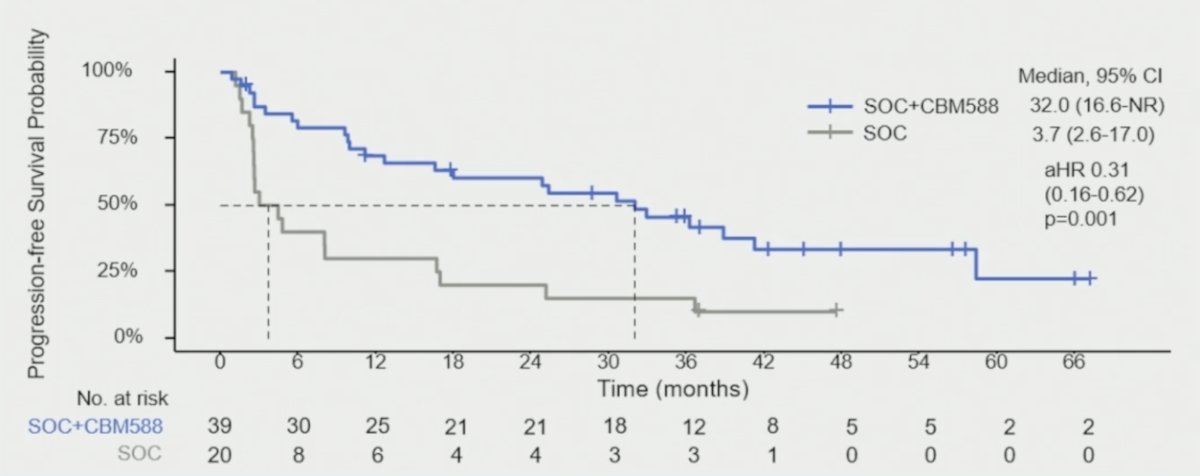
The median progression-free survival was 32.0 months (95% CI 16.6-NR) with standard of care + CBM588 versus 3.7 months (95% CI 2.6-17.0) with standard of care (HR 0.31, 95% CI 0.16, 0.62, p = 0.001):
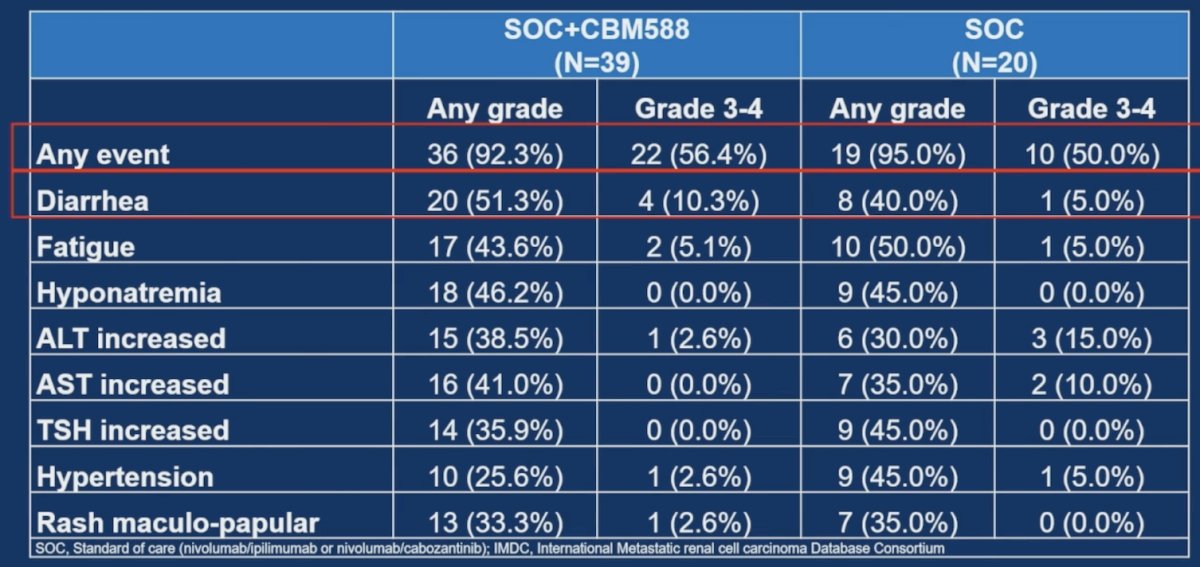
Regarding safety, in the standard of care + CBM588 arm, any grade adverse events occurred in 92.3% of patients and grade 3-4 in 56.4%. Diarrhea was the most common any grade (51.3%) and grade 3-4 (10.3%) adverse event:
At baseline, S score was similar across arms (p = 0.16), and SIG1+ was seen in 55.6% of patients in the standard of care + CBM588 arm versus 44.4% in the standard of care arm (p = 0.441). While differences in progression free survival were not statistically significant in the SIG2+ cohort between standard of care + CBM588 and standard of care alone (32.0 versus 10.9 months, HR 0.58 [95% CI 0.19-1.73]), in the SIG1+ setting, a progression free survival improvement was seen for standard of care + CBM588 versus standard of care alone (24.9 versus 2.8 months, HR 0.17 [95% CI 0.05-0.54]):
![At baseline, S score was similar across arms (p = 0.16), and SIG1+ was seen in 55.6% of patients in the standard of care + CBM588 arm versus 44.4% in the standard of care arm (p = 0.441). While differences in progression free survival were not statistically significant in the SIG2+ cohort between standard of care + CBM588 and standard of care alone (32.0 versus 10.9 months, HR 0.58 [95% CI 0.19-1.73]), in the SIG1+ setting, a progression free survival improvement was seen for standard of care + CBM588 versus standard of care alone (24.9 versus 2.8 months, HR 0.17 [95% CI 0.05-0.54]):](/images/com-doc-importer/273-asco-2026/asco-2026-microbial-dysbiosis-as-predictor-of-benefit-from-cbm588-as-an-adjunct-to-immune-checkpoint-blockade-based-first-line-therapies-in-metastatic-rcc/image-4.jpg)
Notablythe , S score was associated with response to standard of care + CBM588 among patients who received nivolumab/ipilimumab backbone (median S score 0.668 in response versus 0.540 in no response, p = 0.044), while no such association was observed in patients treated with nivolumab/cabozantinib backbone:

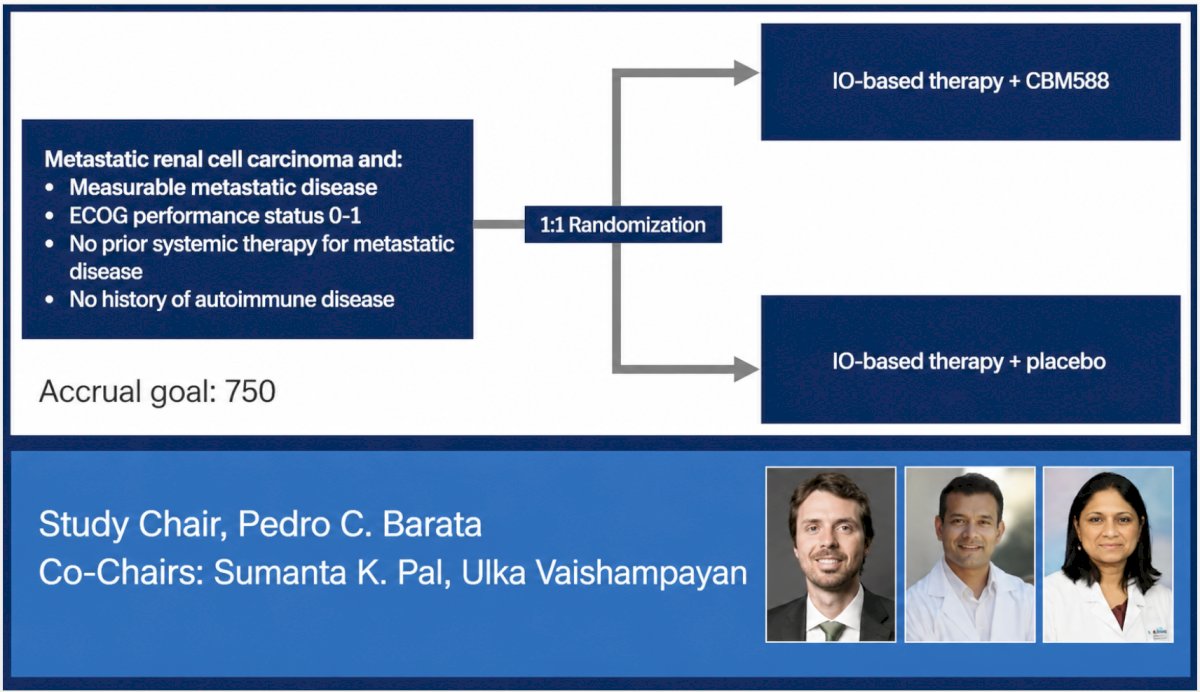
CBM588 with front-line immune checkpoint blockade regimens showed improved clinical outcomes relative to standard of care alone, with no new safety concerns, which substantiates the recently activated SWOG BIOFRONT study (S2419; NCT07383441):
Dr. Winayak concluded this presentation discussing microbial dysbiosis as a predictor of benefit from CBM588 as an adjunct to immune checkpoint blockade-based first-line therapies in metastatic RCC with the following take-home points:
- CBM588 showed enhanced clinical activity with first-line immune checkpoint blockade for metastatic RCC
- CBM588 with first-line immune checkpoint blockade conferred a greater benefit with dysbiotic stool genotypes
- The upcoming phase III randomized placebo-controlled BIOFRONT trial will assess the clinical activity of CBM588 and advance microbiome-based predictive biomarker development in metastatic RCC
Presented by: Rahul Winayak, City of Hope Comprehensive Cancer Center, Duarte, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026