(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a kidney and bladder cancers poster session. Dr. Robert Motzer presented the final analysis of the TiNivo-2 phase III trial evaluating long-term outcomes of tivozanib in patients with metastatic renal cell carcinoma (mRCC).
As treatment paradigms for mRCC continue to evolve, optimal sequencing after prior immune checkpoint inhibitor (ICI) exposure remains a major clinical challenge. The initial TiNivo-2 results, previously published in The Lancet in 2024,1 demonstrated that rechallenging patients with an ICI did not improve outcomes compared to VEGFR tyrosine kinase inhibitor monotherapy. However, the study highlighted encouraging activity for single-agent tivozanib in the post-ICI setting. This final analysis aimed to further characterize the long-term efficacy and safety profile of tivozanib-based therapy in this increasingly common clinical scenario.
TiNivo-2 was a randomized phase III trial enrolling patients with metastatic RCC who had previously received immune checkpoint inhibitor therapy. Patients were randomized to receive either:
- Tivozanib 0.89 mg daily (21 days on/7 days off) plus nivolumab 480 mg every 4 weeks
- Tivozanib monotherapy 1.34 mg daily (21 days on/7 days off)
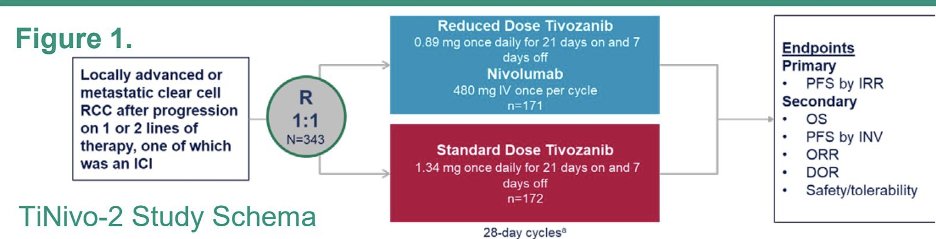
The current report focused on final progression-free survival (PFS), overall survival (OS), and long-term safety outcomes.
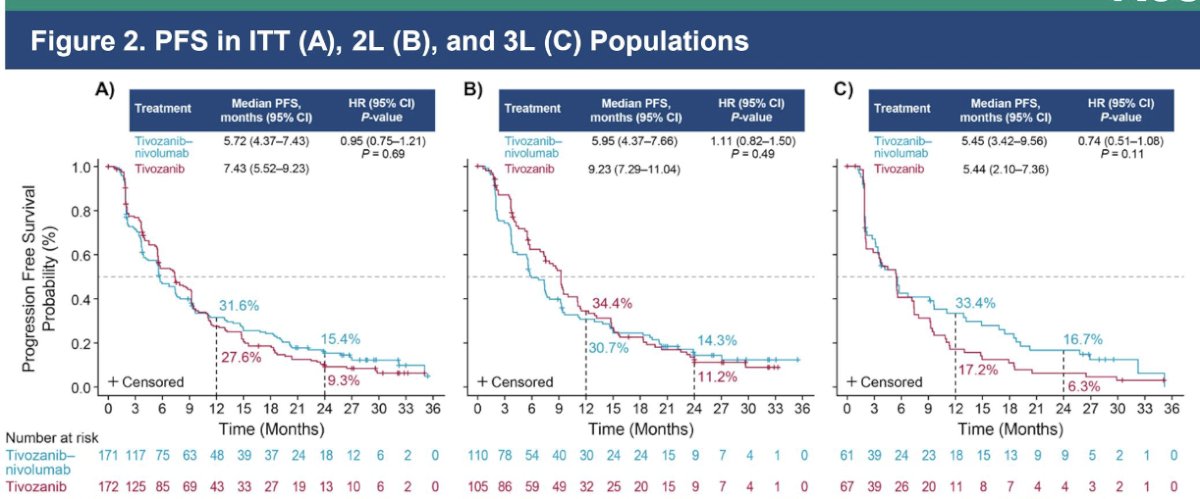
Long-term progression-free survival outcomes with standard-dose tivozanib were as follows:
- ITT population (N=172): median PFS 7.43 months (95% CI: 5.52–9.23)
- Second-line population (N=105): median PFS 9.23 months (95% CI: 7.29–11.04)
- Third-line population (N=67): median PFS 5.44 months (95% CI: 2.10–7.36)
The Kaplan-Meier curves demonstrated the most favorable disease control in the second-line setting, where median PFS exceeded 9 months.
Overall Survival
Overall survival remained durable across treatment lines:
- ITT population: median OS 22.93 months (95% CI: 18.14–NR)
- Second-line population: median OS 23.52 months (95% CI: 18.33–NR)
- Third-line population: median OS 22.70 months (95% CI: 11.79–NR)

Objective Response and Disease Control
Best overall response was assessed by the investigator per RECIST v1.1. Among patients receiving standard-dose tivozanib, the objective response rate (ORR) was:
- ITT population: 18.1% (95% CI: 12.7–24.7)
- Second-line population: 29.7% (95% CI: 18.5–36.2)
- Third-line population: 10.5% (95% CI: 4.3–20.4)
Complete responses were observed in:
- 1.7% of ITT patients
- 0.9% of second-line patients
- 1.5% of third-line patients
Partial responses occurred in:
- 18.6% of ITT patients
- 17.5% of second-line patients
- 19.7% of third-line patients
Stable disease was achieved in:
- 44.4% of ITT patients
- 49.1% of second-line patients
- 36.1% of third-line patients
Progressive disease was reported in:
- 28.1% of ITT patients
- 25.5% of second-line patients
- 32.8% of third-line patients
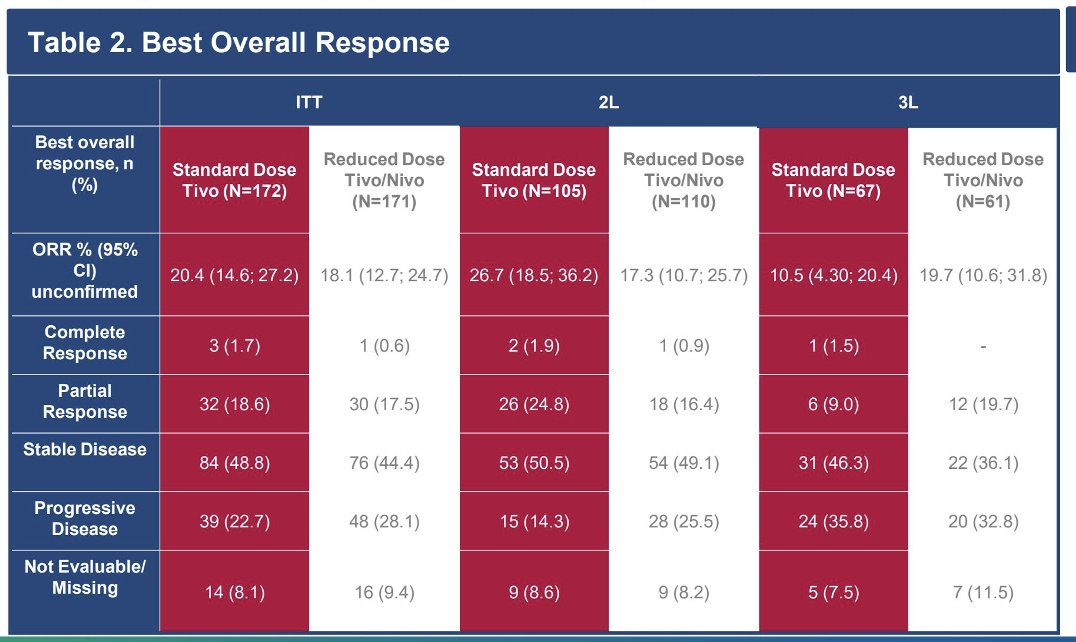
Overall, there were more patients with complete response, partial response, and stable disease in the standard-dose tivozanib arm compared with the reduced-dose tivozanib/nivolumab arm.
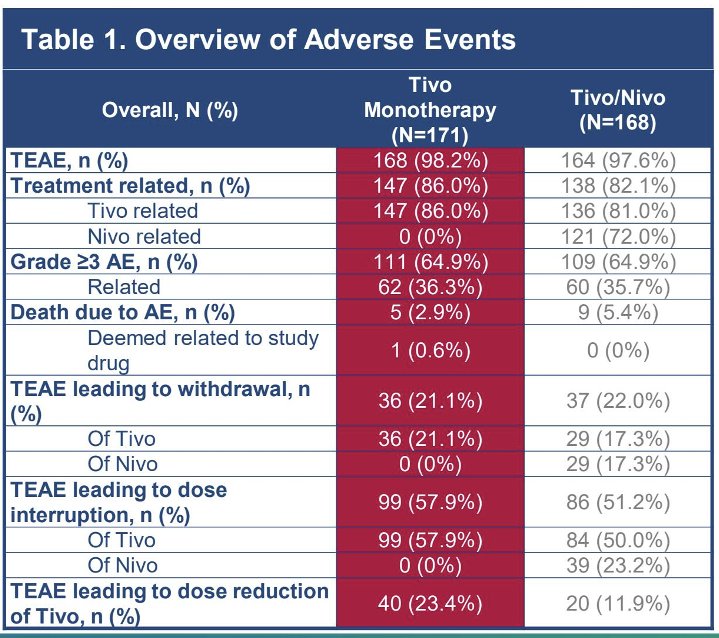
The long-term safety profile of tivozanib remained consistent with prior reports, and no new safety signals emerged.
Among patients receiving standard-dose tivozanib monotherapy (N=171):
- Any treatment-emergent adverse event (TEAE): 168 patients (98.2%)
- Treatment-related TEAE: 147 patients (86.0%
- Grade ≥3 adverse event: 111 patients (64.9%)
- Grade ≥3 treatment-related adverse event: 62 patients (36.3%)
- TEAE leading to treatment withdrawal: 36 patients (21.1%), TEAE leading to dose reduction: 40 patients (23.4%)
- Death due to adverse events: 5 patients (2.9%)
- Treatment-related death: 1 patient (0.6%)
The most common treatment-related adverse events were hypertension and dysphonia. Hypertension was the most frequent any-grade and grade ≥3 treatment-related adverse event and occurred at similar rates across treatment groups. The poster specifically notes that the type and frequency of adverse events observed with tivozanib monotherapy were consistent with the known safety profile of tivozanib reported in the original TiNivo-2 study.
The investigators concluded that this final long-term analysis demonstrates durable efficacy and a manageable safety profile for standard-dose tivozanib monotherapy in previously treated mRCC. With extended follow-up approaching 28 months, tivozanib achieved a median PFS of 7.43 months in the ITT population and 9.23 months in second-line patients, while median OS exceeded 22 months across all analyzed populations. These findings further support the role of standard-dose tivozanib as an effective treatment option for patients receiving second- and third-line therapy for metastatic renal cell carcinoma.
Presented by: Robert J. Motzer, MD, Attending Physician, Medical Oncologist, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Reference: