(UroToday.com) The 2026 ASCO annual meeting featured an oral abstract kidney cancer session and a presentation by Dr. Junru Chen discussing a prospective, multi-center, phase Ib/II trial of first line cadonilimab + axitinib in advanced non-clear cell renal cell carcinoma (RCC).
Non-clear cell RCC comprises ~20-25% of all RCC and includes papillary, chromophobe, translocation-associated, collecting duct, medullary, and unclassified subtypes. These subtypes differ substantially in biology, prognosis, and therapeutic sensitivity. Most pivotal RCC trials have been dominated by clear cell histology, leaving non-clear cell RCC supported mainly by smaller phase II studies, retrospective series, or subtype-specific extrapolation:
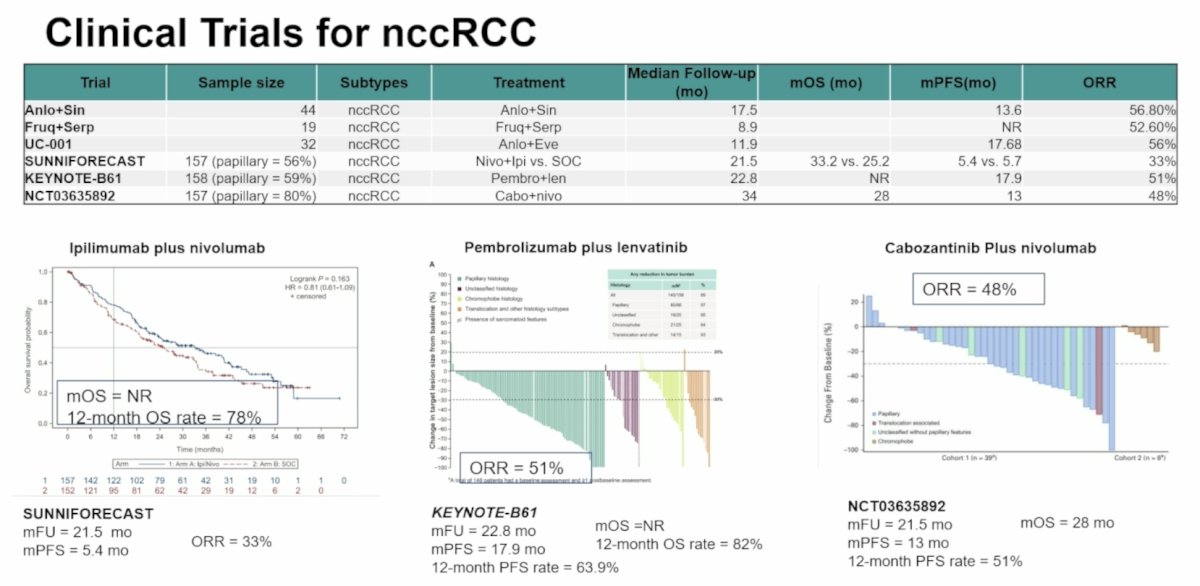
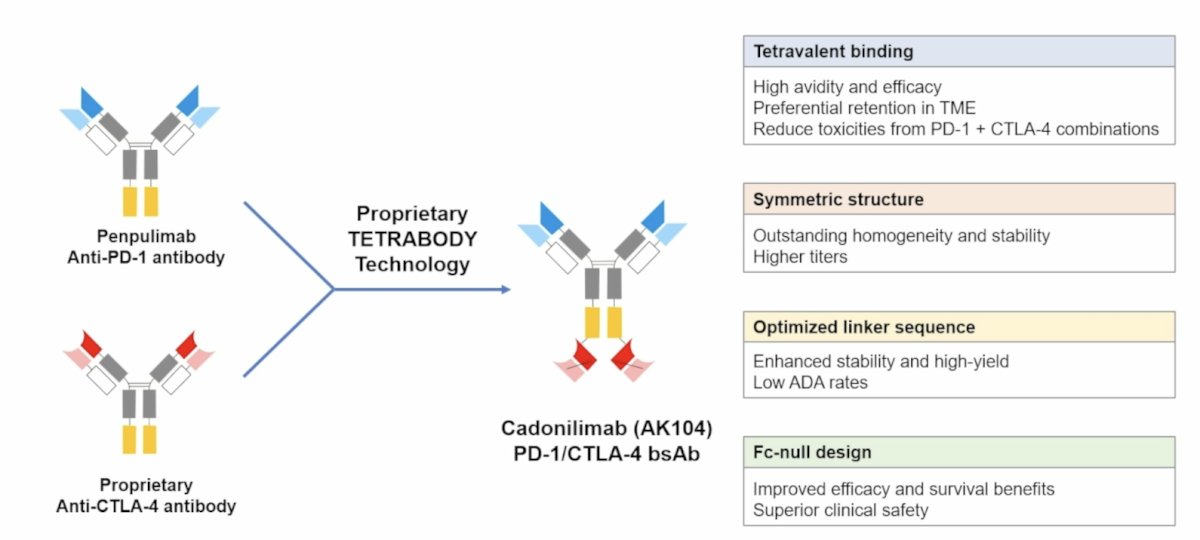
Guidelines and expert reports consistently emphasize enrollment in prospective trials whenever feasible. Prospective data support activity of IO/TKI and IO/IO combinations in advanced non-clear cell RCC, including pembrolizumab + lenvatinib and nivolumab + cabozantinib in selected populations. However, the benefit remains inconsistent across histologies, and durable disease control is still not optimized. Cadonilimab, a bispecific PD-1/CTLA-4 antibody, has shown antitumor activity in various solid tumors, but its efficacy in RCC remains unknown:
At the ASCO 2026 annual meeting, Dr. Chen and colleagues reported the initial results from a phase Ib/II trial of cadonilimab + axitinib in advanced non-clear cell RCC.
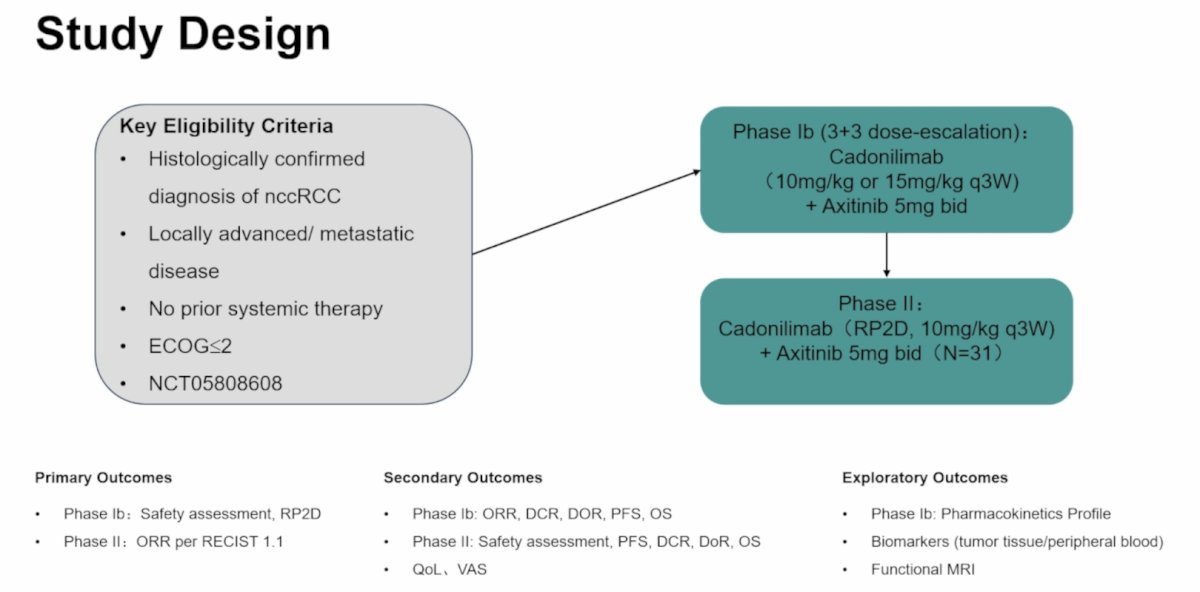
This open-label, multi-center, single-arm, phase Ib/II trial included patients with metastatic or unresectable treatment-naive non-clear cell RCC, regardless of PD-L1 status, to receive cadonilimab + axitinib 5 mg BID. In phase Ib, a 3+3 dose-escalation design was adopted, starting at 10 mg/kg every 3 weeks of cadonilimab with axitinib to evaluate safety. In phase II, an additional 31 patients were enrolled at the recommended phase II dose. The primary endpoints were safety assessment in phase Ib and objective response rate by RECIST v1.1 in phase II:
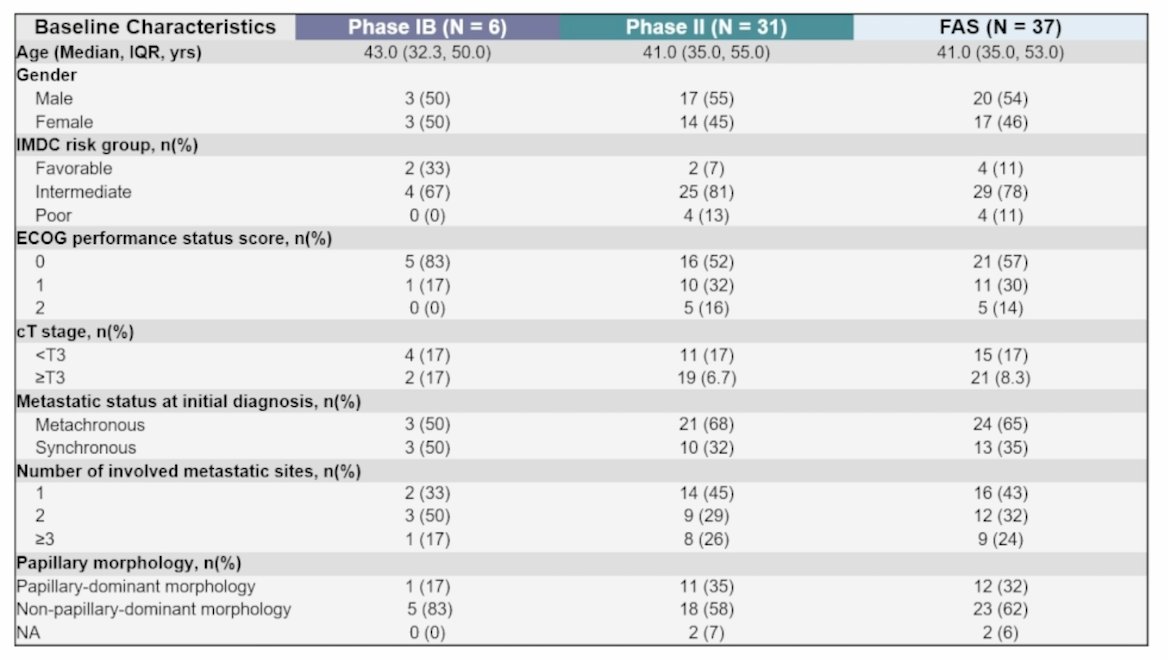
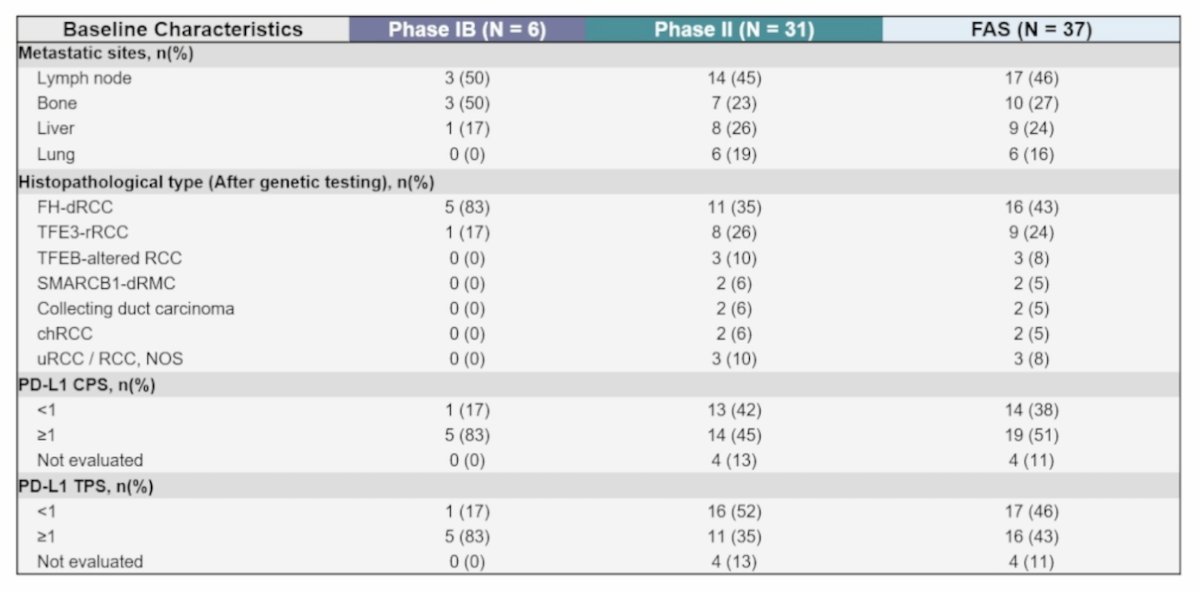
As of October 1, 2025, a total of 37 patients were enrolled (Phase Ib: n = 6; Phase II: n = 31), with the following baseline characteristics:
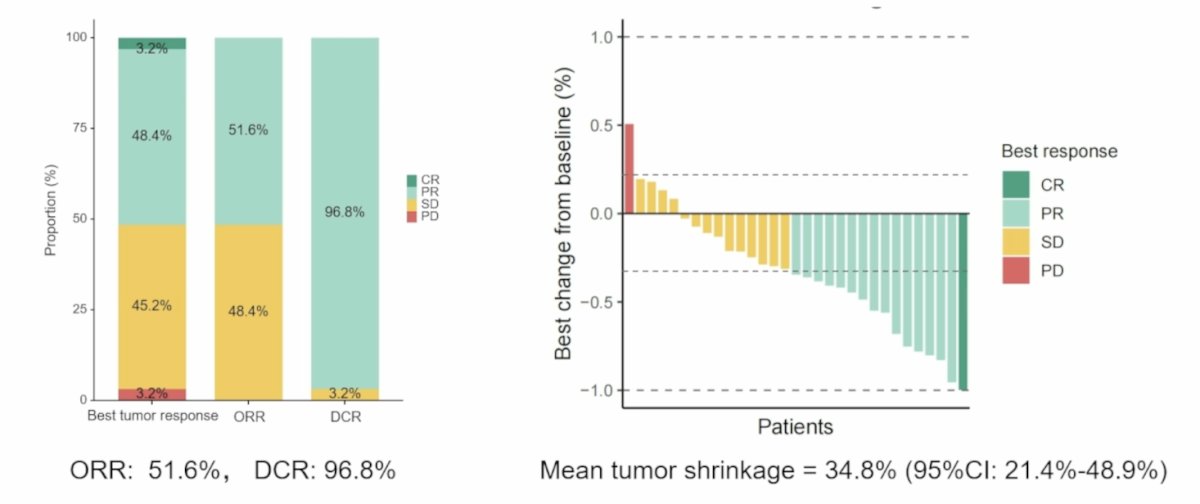
The median follow-up duration was 14.4 months. In phase Ib, no dose-limiting toxicities were observed, and adverse events were reported in 100% (6/6) of cases. Grade ≥ 3 treatment-related adverse events occurred in 66.7% (4/6) of cases, including proteinuria, hypertriglyceridemia, myasthenia gravis, diarrhea, and increased alanine aminotransferase. The recommended phase II dose for cadonilimab was 10 mg/kg. For secondary endpoints, objective response rate was 50% (2/4) and disease control rate was 100% (6/6). In phase II, the objective response rate was 51.6% (16/31), the disease control rate was 96.8% (30/31), and mean tumor shrinkage was 34.8% (95% CI 21.4%-48.9%):
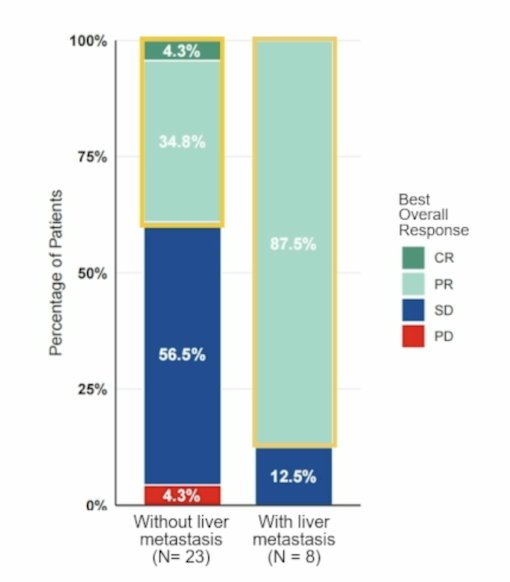
Liver metastasis at baseline was associated with a favorable objective response rate in the phase II cohort:
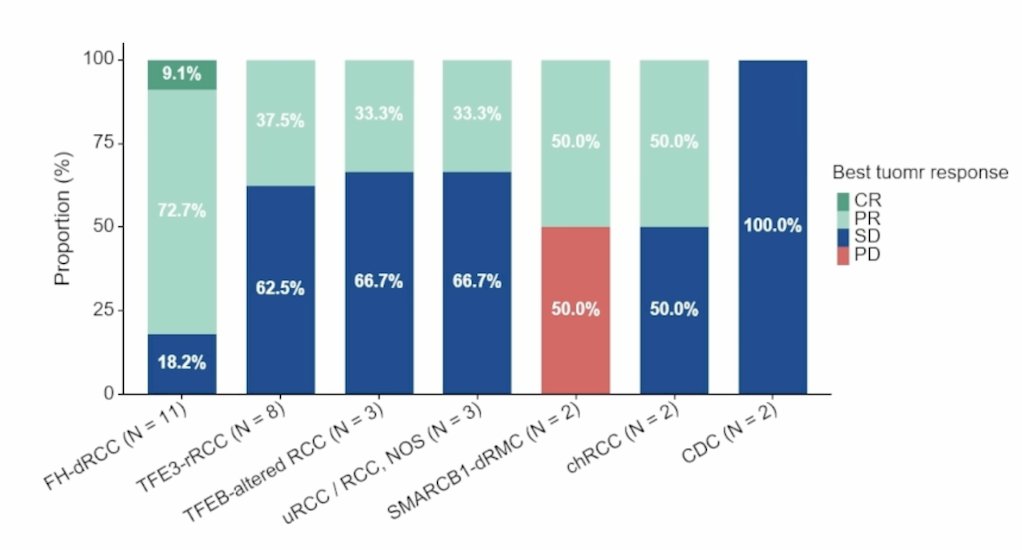
Among histopathological subtypes, the objective response rates were:
- FH-dRCC: 81.8% (9/11)
- TFE3-rRCC: 37.5% (3/8)
- TFEB-altered RCC: 33.3% (1/3)
- uRCC/RCC, NOS: 33.3% (1/3)
- SMARCB1-deficient RCC: 50% (1/2)
- chRCC: 50% (1/2)
- Collecting duct carcinoma: 0% (0/2)
The median time to response was 3.5 months (range: 2.7-9.5), and the median duration of response was 17.5 months (range: 11.2 to not reached). Overall, 61.1% of responders remained in response for 12 months, and 19 patients are still continuing treatment at the data cutoff. The median progression-free survival in the total cohort was 19.2 months (95% CI 13.9 to not reached), and in the phase II cohort was 14.2 months (95% CI 11.2 to not reached):

Amongst subgroup analyses, synchronous metastasis was associated with worse progression-free survival:

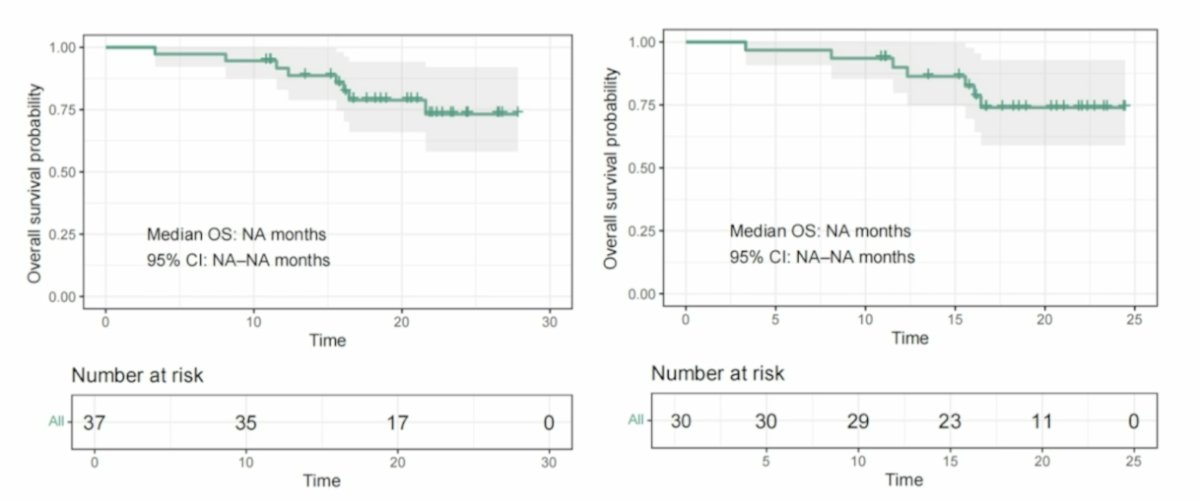
For overall survival, in the total cohort, the median overall survival was not reached, and was also not reached in the phase 2 cohort:
Adverse events were reported in 100.0% of cases, and grade ≥3 treatment-related adverse events occurred in 59.5% (22/37) of cases. All adverse events were expected and manageable. In an exploratory analysis, WES and RNA sequencing were performed in 34 (91.9%) and 34 (91.9%) of patients, respectively: TMB, SCNA burden, and NF2 mutation status were not significantly associated with therapeutic response:

Dr. Chen concluded this presentation discussing a prospective, multi-center, phase Ib/II trial of first line cadonilimab + axitinib in advanced non-clear cell RCC with the following take-home points:
- The combination of cadonilimab + axitinib showed a manageable safety profile, with no dose-limiting toxicities observed in phase Ib, supporting 10 mg/kg every 3 weeks as the recommended phase 2 dose
- First-line cadonilimab + axitinib demonstrated promising antitumor activity in patients with advanced non-clear cell RCC
- Objective response rate: 51.6%
- Median progression-free survival: 19.2 months
- Median overall survival: not reached
- Longer follow-up and biomarker analyses are ongoing
Presented by: Junru Chen, MD, PhD, West China Hospital, Sichuan University, Sichuan, China
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026