(UroToday.com) The 2026 ASCO annual meeting featured a urothelial carcinoma trials in progress session and a presentation by Dr. Matthew Galsky discussing TROPION-Urothelial03, a phase 2/3 study of datopotamab deruxtecan + platinum based chemotherapy versus gemcitabine + platinum based chemotherapy in participants with locally advanced or metastatic urothelial carcinoma with progression on or after enfortumab vedotin + pembrolizumab. Although first line enfortumab vedotin + pembrolizumab has improved outcomes for patients with locally advanced or metastatic urothelial carcinoma, most experience disease progression, highlighting an unmet need for novel therapies. While there is limited evidence to guide the optimal selection of second line therapies post disease progression on or after first line enfortumab vedotin, current guideline recommendations include platinum based chemotherapy, which has demonstrated modest efficacy in studies to date. Complete response rates range from 2.9-10%, the median duration of response is ~4 months, the median progression free survival is 3.4-4.4 months, and the median overall survival is <1 year.
TROP2 is a glycoprotein highly expressed in several epithelial tumors, including urothelial carcinoma. Datopotamab deruxtecan is a TROP2-directed antibody–drug conjugate comprising an anti-TROP2 monoclonal antibody, a tetrapeptide-based cleavable linker, and a topoisomerase I inhibitor payload (DXd), designed to induce selective tumor-cell death and reduce systemic exposure to the payload. Datopotamab deruxtecan has demonstrated durable efficacy and a manageable safety profile in patients with locally advanced or metastatic urothelial carcinoma, both as monotherapy (TROPION-PanTumor01 [NCT03401385]) and in combination with immunotherapy (TROPION-PanTumor03 [NCT05489211]). At the ASCO 2026 annual meeting, Dr. Galsky and colleagues described a phase 2/3 trial comparing the efficacy and safety of datopotamab deruxtecan + platinum chemotherapy (carboplatin or cisplatin) versus gemcitabine + platinum chemotherapy in participants with locally advanced or metastatic urothelial carcinoma with disease progression on or after enfortumab vedotin + pembrolizumab.
TROPION-Urothelial03 (NCT07129993) is a global, multicenter, randomized, open-label, Phase 2/3 trial. In Part A (Phase 2), ~60 participants will be randomized 1:1 to receive datopotamab deruxtecan 4 or 6 mg/kg + platinum chemotherapy. In Part B (Phase 3), ~570 participants will be randomized 1:1 to receive datopotamab deruxtecan at the recommended Phase 3 dose (determined using Part A data) + platinum chemotherapy versus gemcitabine + platinum chemotherapy. Randomization in Part A is stratified by assignment of platinum chemotherapy (carboplatin versus cisplatin), and in Part B, by assignment of platinum chemotherapy, presence versus absence of liver metastasis at screening, and time to progression on first line enfortumab vedotin + pembrolizumab (<6 versus ≥6 months). Study treatment continues until disease progression, unacceptable toxicity, withdrawal of consent, death, loss to follow-up, or other reasons per protocol.
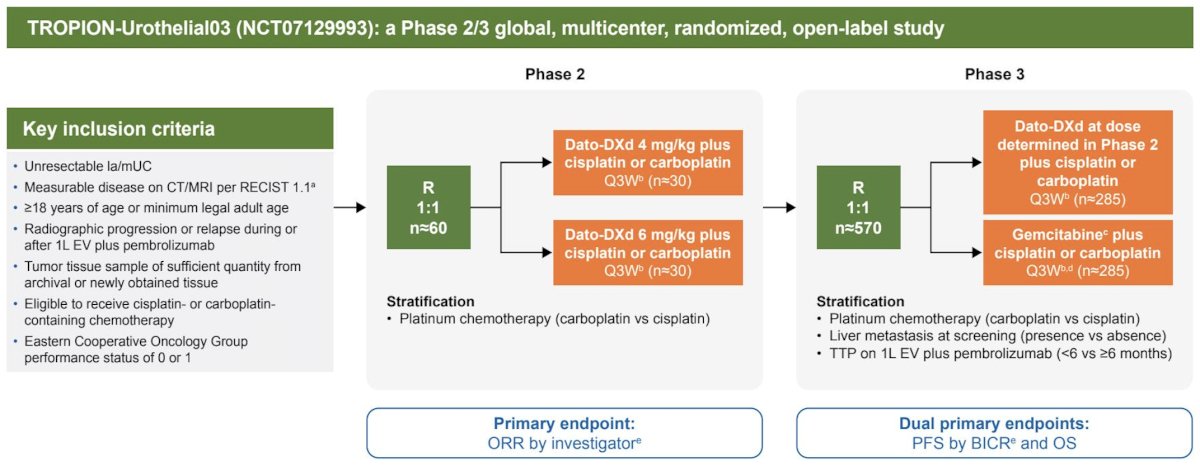
Radiographic tumor assessments occur every 6 weeks for 54 weeks, then every 12 weeks. The primary endpoint of Part A is objective response rate by investigator per RECIST, version 1.1 (RECIST 1.1). The dual primary endpoints of Part B are progression free survival by blinded independent central review per RECIST 1.1 and overall survival. Secondary endpoints include duration of response by investigator per RECIST 1.1 (Part A), and progression free survival by investigator per RECIST 1.1 and objective response rate by blinded independent central review and investigator per RECIST 1.1 (Part B). In Part A, objective response rate will be summarized with 2-sided 95% exact confidence intervals using the Clopper–Pearson method by trial group. In Part B, progression free survival and overall survival will be compared between trial groups using a log-rank test stratified by randomization stratification factors, with hazard ratios from the stratified Cox regression model.
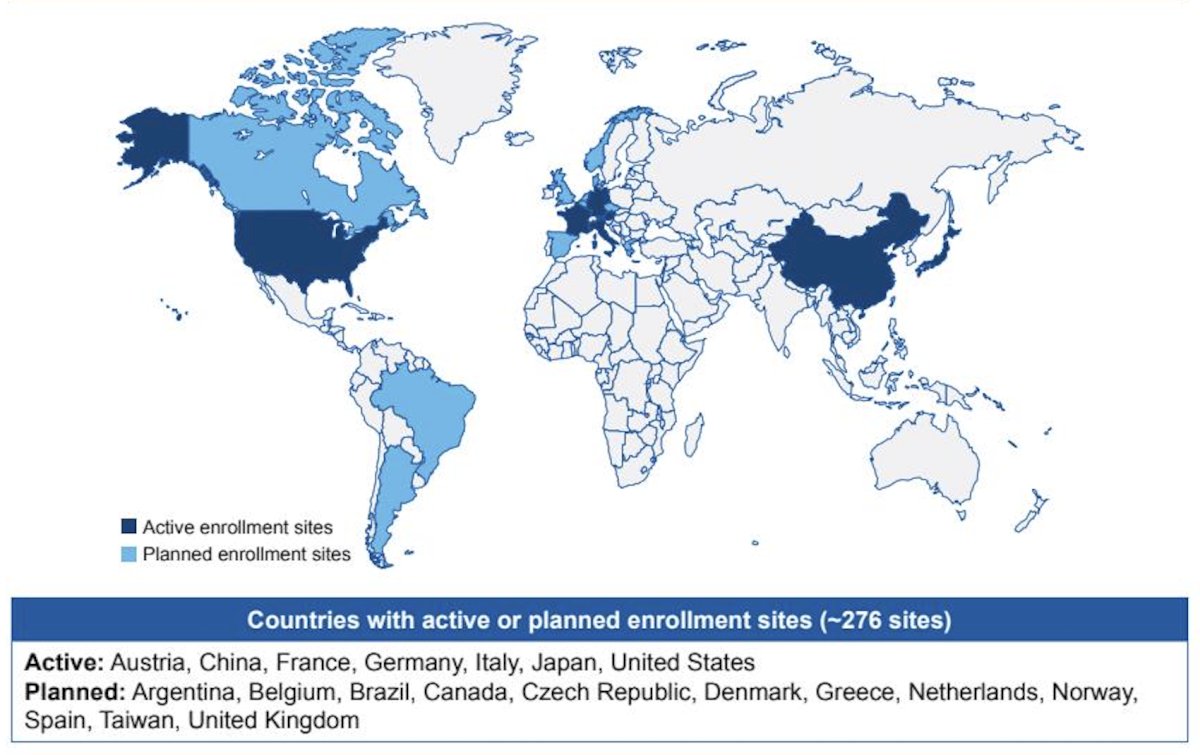
Enrollment started in September 2025, and is ongoing at ~276 sites at the following active and planned countries:
Presented by: Matthew Galsky, MD, Icahn School of Medicine, Mount Sinai Medical Center, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026