(UroToday.com) The 2026 ASCO annual meeting featured a urothelial carcinoma rapid abstract session and a presentation by Dr. Shilpa Gupta discussing MAIN-CAV, a phase III randomized trial of maintenance cabozantinib and avelumab versus avelumab after first-line platinum-based chemotherapy in patients with locally advanced or metastatic urothelial carcinoma.
Maintenance avelumab is a standard of care in patients with locally advanced or metastatic urothelial carcinoma who do not progress after first-line platinum-based chemotherapy.1 However, despite improved survival, most patients ultimately progressed, indicating an opportunity to build upon the avelumab backbone. Cabozantinib is an oral inhibitor of MET, VEGFR, and TAM, active in multiple solid tumors. Thus, Dr. Gupta and colleagues hypothesized that an avelumab + cabozantinib combination would improve outcomes in patients with metastatic urothelial carcinoma with an acceptable safety profile compared to avelumab maintenance alone.
MAIN-CAV (NCT05092958) is a phase III randomized, multicenter, international trial for locally advanced or metastatic urothelial carcinoma patients who did not progress after 4-6 cycles of any platinum-based chemotherapy (gemcitabine + cisplatin, gemcitabine + carboplatin, MVAC, ddMVAC). Patients were randomized 1:1 to avelumab 800 mg IV every 2 weeks alone or with cabozantinib 40 mg daily for ≤2 years. Stratification factors were response to first-line platinum-based chemotherapy (complete response versus partial response versus stable disease) and visceral metastases: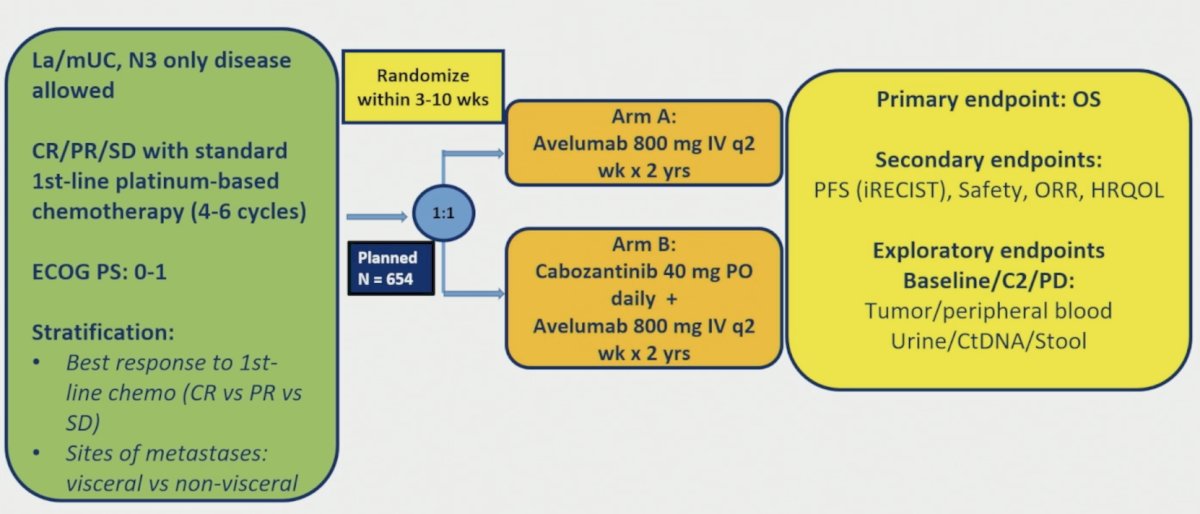
The primary endpoint was overall survival, and secondary endpoints included progression-free survival, safety, and quality of life. The target accrual was 654 patients, the trial closed early after enrollment of 68 patients following adoption of enfortumab vedotin + pembrolizumab as the new preferred first-line standard in the US [2].
From March 2022 to March 2024, 68 patients were randomized (avelumab n = 33; cabozantinib + avelumab n = 35). The patient characteristics for the trial are highlighted in the following table: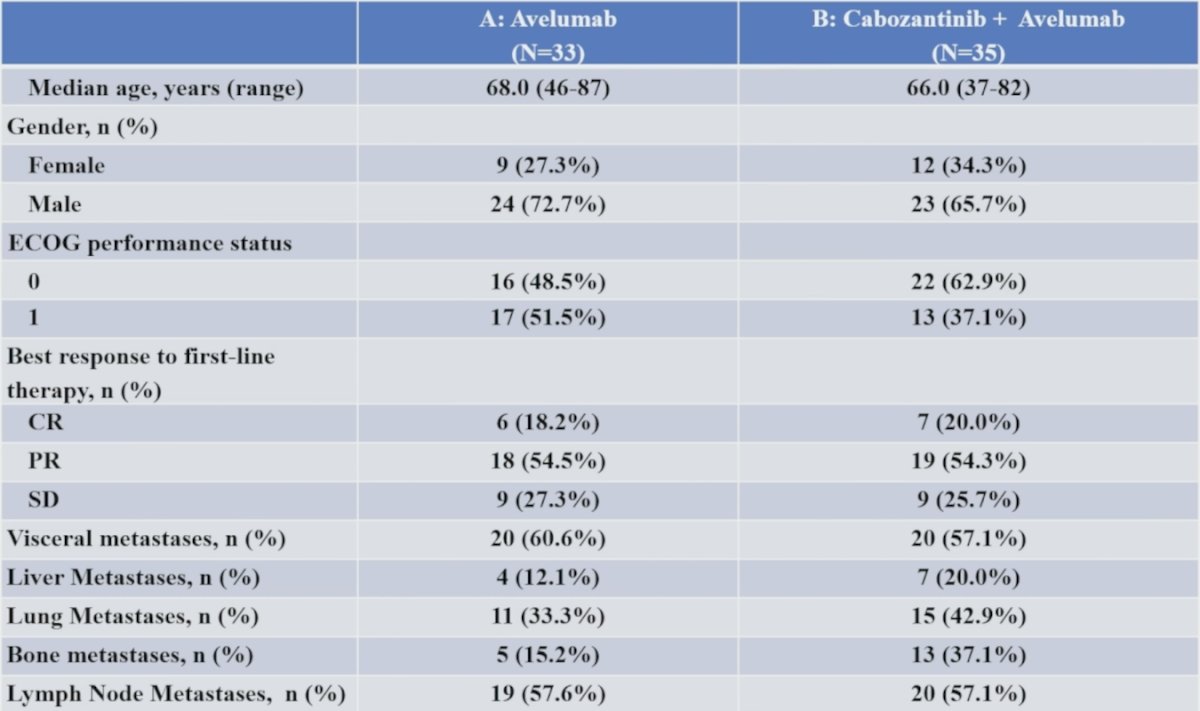
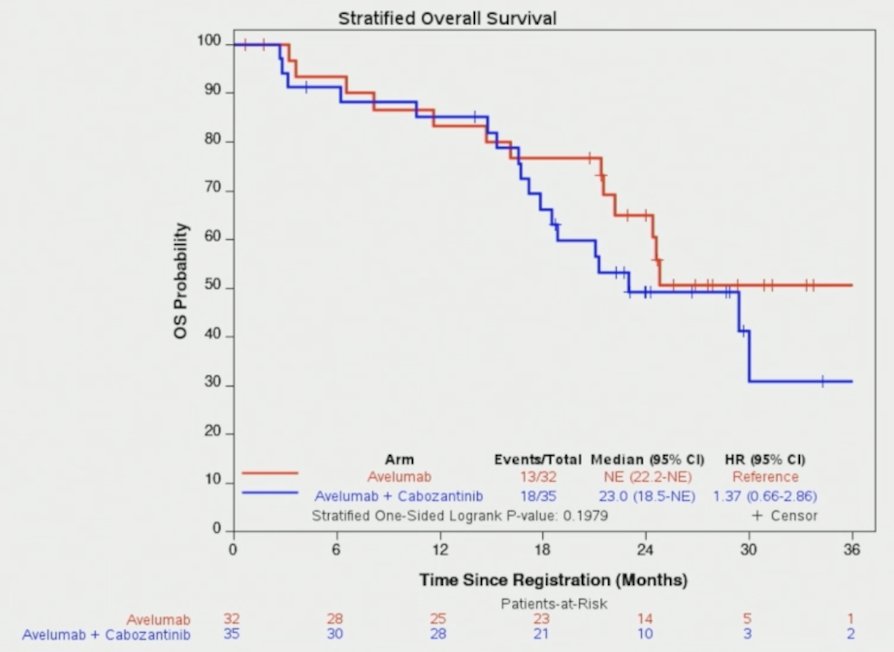
The median overall survival was not reached with avelumab and 23.0 months with avelumab + cabozantinib (HR 1.37; 95% CI 0.66–2.86):
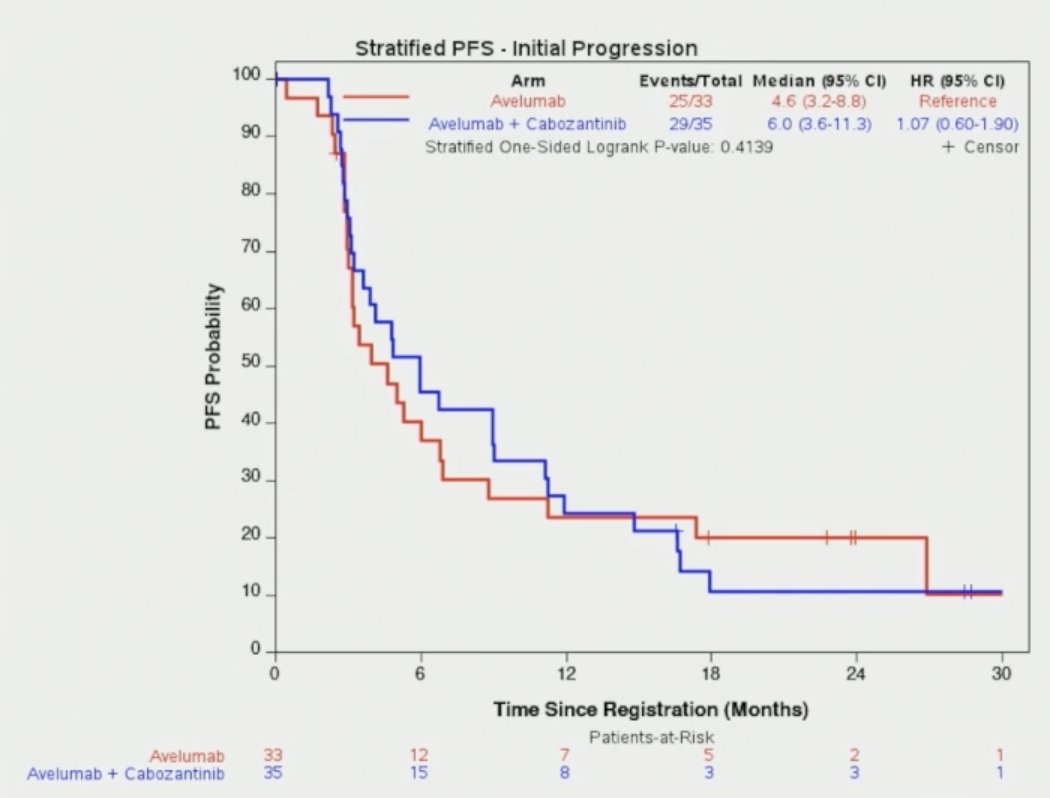
The median progression-free survival was 4.6 months with avelumab versus 6.0 months with avelumab + cabozantinib (HR 1.07, 95% CI 0.60-1.90):
Objective response rate among patients with partial response or stable disease after first-line platinum-based chemotherapy was 20.8% with avelumab versus 11.5% with avelumab + cabozantinib (adjusted OR 0.56, 95% CI 0.13-2.44; p = 0.424). Grade ≥3 treatment-related adverse events occurred in 24.2% patients on the avelumab arm versus 39.4% of patients on the avelumab + cabozantinib arm, and cabozantinib dose reductions occurred in 67% of patients: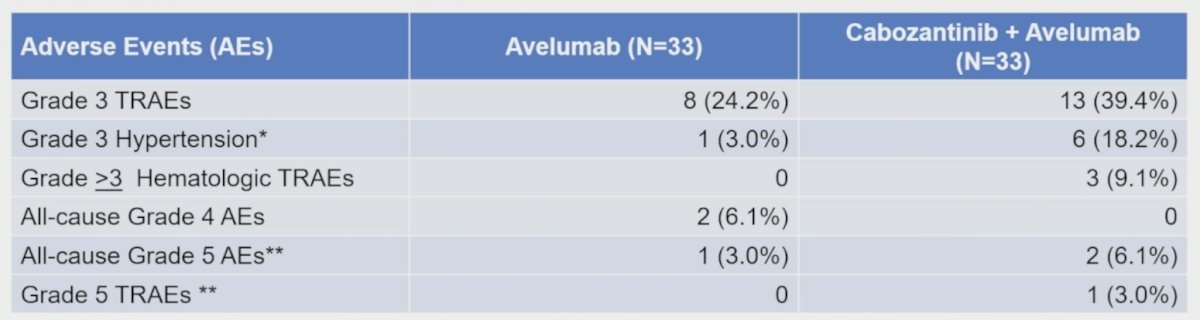
Dr. Gupta concluded her presentation discussing the results of MAIN-CAV with the following take-home points:
- In this prematurely closed, underpowered randomized trial, there was no clear efficacy benefit observed with the addition of cabozantinib to avelumab compared with avelumab alone
- Safety was consistent with the known profiles of avelumab and cabozantinib, with no new safety signals identified
- Ongoing correlative analyses may provide biologic insights into mechanisms of response and resistance
Presented by: Shilpa Gupta, MD, Director, Genitourinary Medical Oncology, Taussig Cancer Institute, Co-Leader of the Genitourinary Oncology Program, Department of Hematology and Medical Oncology, Cleveland Clinic, Cleveland, OH
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- Powles T, Park SH, Voog E, et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N Engl J Med 2020 Sept 24;383(13):1218-1230.
- Powles T, Valderrama BP, Gupta S, et al. Enfortumab Vedotin and Pembrolizumab in Untreated Advanced Urothelial Cancer. N Engl J Med. 2024 Mar 7;390(10)875-888.