(UroToday.com) The 2026 ASCO annual meeting featured a urothelial carcinoma rapid abstract session and a presentation by Dr. Xin Gao discussing the initial results from EXCEED, a phase 1 study of LY4101174, an antibody-drug conjugate targeting Nectin-4, in participants with advanced or metastatic urothelial carcinoma. Enfortumab vedotin + pembrolizumab is the current first-line standard of care for locally advanced or metastatic urothelial carcinoma, establishing Nectin-4 as a clinically important target in urothelial carcinoma.
However, subsequent treatment options are limited, representing an urgent and growing unmet need. Preclinical data suggest that enfortumab vedotin resistance may be payload-mediated and consequently Nectin-4 remains a viable target for alternative therapies. LY4101174 is a next-generation anti-Nectin-4 antibody drug conjugate comprising a humanized IgG1 antibody conjugated to the topoisomerase I inhibitor, exatecan, via a maleimide-ß-glucuronide poly-sarcosine linker and a homogeneous drug antibody ratio of 8: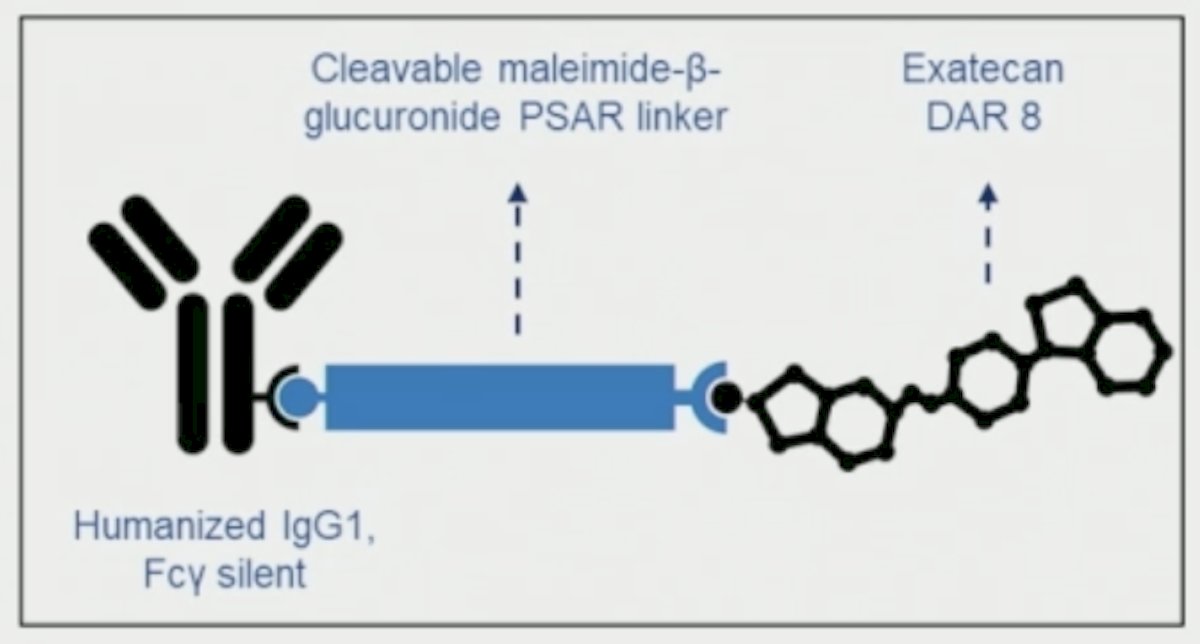
At the ASCO 2026 annual meeting, Dr. Gao reported the initial clinical data from the phase 1 dose escalation cohort of EXCEED (NCT06238479).
Adults with locally advanced or metastatic urothelial carcinoma or other selected solid tumors were eligible. Participants must have received or been ineligible for available standard therapies and have an ECOG performance status of 0-1. Dose escalation utilized a Bayesian optimal interval design: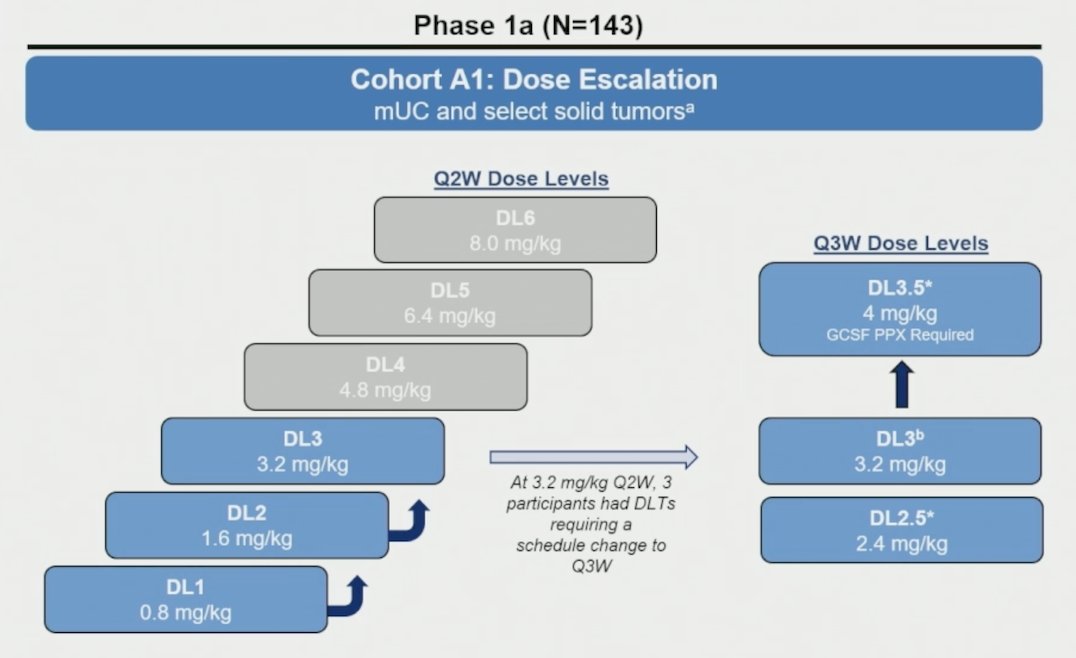
Key endpoints were safety, pharmacokinetics, and antitumor activity of LY4101174 per RECIST v1.1.
As of March 9, 2025, 143 participants (86 metastatic urothelial carcinoma, 57 non-urothelial carcinoma tumors) were treated across 6 dose levels of LY4101174 (0.8-3.2 mg/kg every 2 weeks or 2.4-4.0 mg/kg every 3 weeks IV). The median age was 68 (range: 30-85), 62% had an ECOG performance status of 1, and the median prior lines of therapy was 3 (range: 1-8). Overall, 92% of metastatic urothelial carcinoma participants had received prior enfortumab vedotin, with 19% discontinuing enfortumab vedotin due to treatment-related toxicity: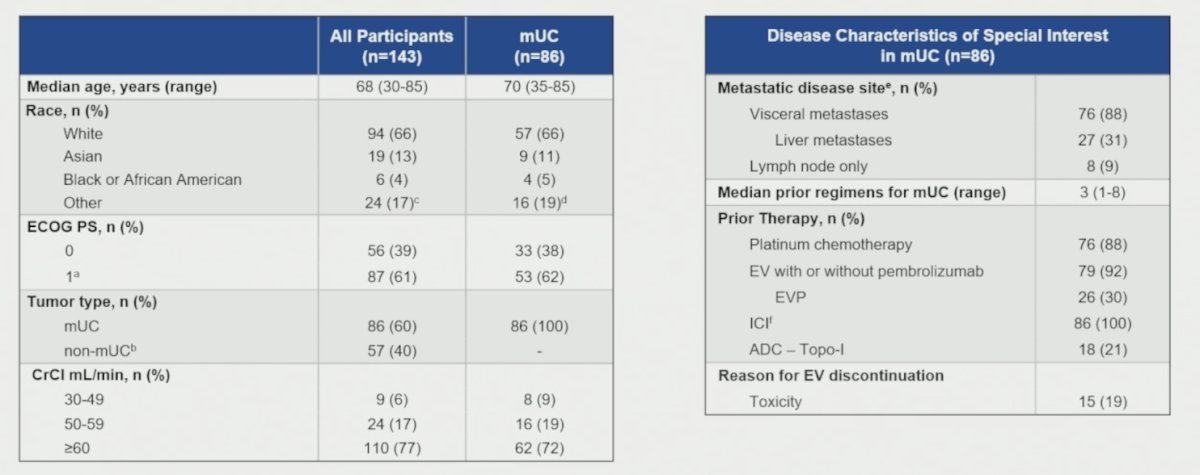
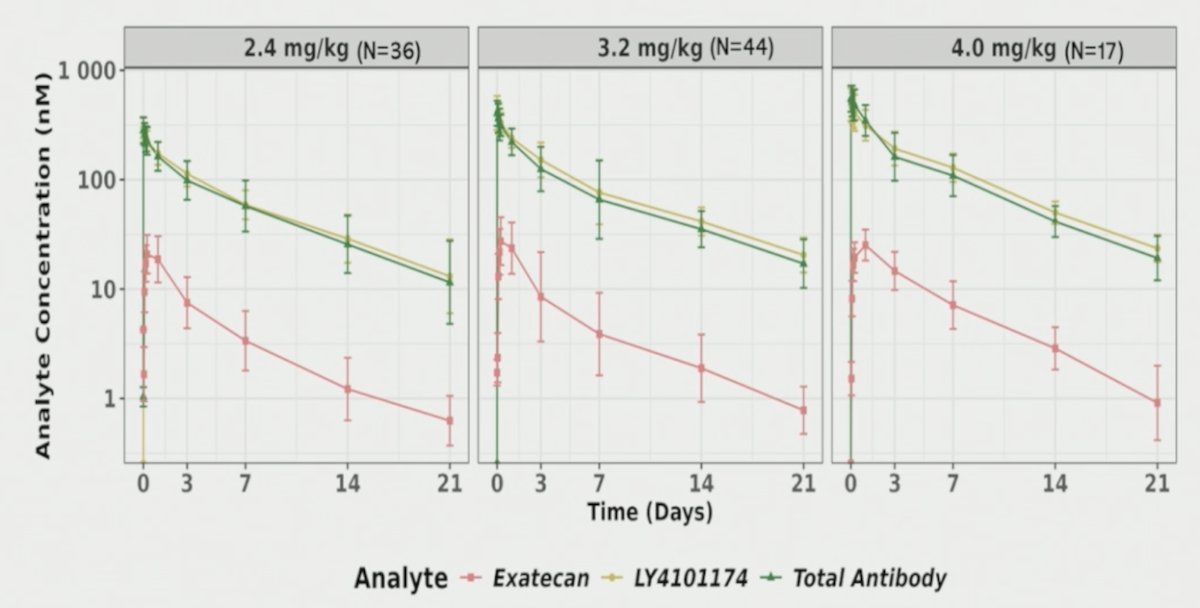
LY4101174 exhibited a mostly linear, dose-proportional pharmacokinetics up to 4.0 mg/kg, and up to 3.2 mg for exatecan. At 3.2 mg/kg every 2 weeks, 3 of 6 participants experienced dose-limiting toxicities (neutropenia [grades 3 and 4], febrile neutropenia, and thrombocytopenia [both grade 3]), prompting a schedule change to 3.2 mg/kg every 3 weeks for continued escalation. The most common treatment-emergent adverse events across every 3-week dose levels were anemia (76%), fatigue (56%), nausea (49%), neutropenia (39%), thrombocytopenia (36%), diarrhea (26%), vomiting (28%), and decreased appetite (28%). The most common grade ≥3 treatment emergent adverse events were anemia (52%), neutropenia (31%), thrombocytopenia (24%), febrile neutropenia (10%), and leukopenia (13%). Prophylactic G-CSF was required at a dose level of 4.0 mg/kg every 3 weeks:![LY4101174 exhibited a mostly linear, dose-proportional pharmacokinetics up to 4.0 mg/kg, and up to 3.2 mg for exatecan. At 3.2 mg/kg every 2 weeks, 3 of 6 participants experienced dose-limiting toxicities (neutropenia [grades 3 and 4], febrile neutropenia, and thrombocytopenia [both grade 3]), prompting a schedule change to 3.2 mg/kg every 3 weeks for continued escalation. The most common treatment-emergent adverse events across every 3-week dose levels were anemia (76%), fatigue (56%), nausea (49%), neutropenia (39%), thrombocytopenia (36%), diarrhea (26%), vomiting (28%), and decreased appetite (28%). The most common grade ≥3 treatment emergent adverse events were anemia (52%), neutropenia (31%), thrombocytopenia (24%), febrile neutropenia (10%), and leukopenia (13%). Prophylactic G-CSF was required at a dose level of 4.0 mg/kg every 3 weeks:](/images/com-doc-importer/272-asco-2026/asco-2026-initial-results-from-exceed-a-phase-1-study-of-ly4101174-an-antibody-drug-conjugate-targeting-nectin-4-in-participants-with-advanced-or-metastatic-urothelial-carcinoma/image-3.jpg)
Enfortumab vedotin-associated adverse events (ie, skin toxicities, peripheral neuropathy, ocular toxicity, and hyperglycemia) were minimal. Treatment-related adverse events led to dose reduction in 14% of patients at the 2.4 mg/kg dose, 40% at the 3.2 mg/kg dose, and 48% at the 4 mg/kg dose:
With regards to pharmacokinetics, there was an elevated plasma payload release (~8%), consistent with the observed systemic toxicities. Additionally, the maleimide-beta-glucuronide linker may be susceptible to cleavage by normal tissue proteases:
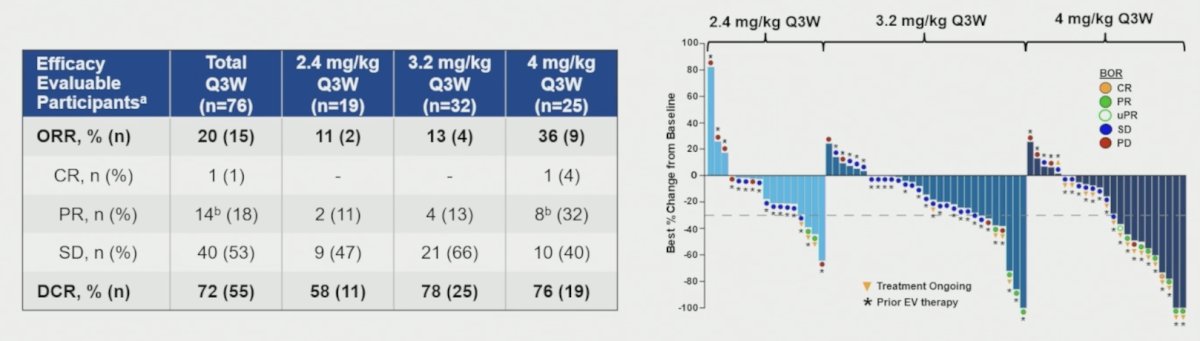
In the 76 efficacy evaluable metastatic urothelial carcinoma participants treated with 2.4-4.0 mg/kg every 3 weeks (93% enfortumab vedotin-pretreated), the objective response rate was 20%, and the disease control rate was 72%, with 14 partial responses (18%) and 40 stable disease (53%). While the 4 mg/kg dose demonstrated promising antitumor activity (objective response rate 36%), grade 3+ hematologic toxicities compromised dose intensity and precluded further dose escalation:
Dr. Gao concluded his presentation discussing the initial results from EXCEED with the following take-home points:
- LY4101174 demonstrated promising clinical activity in a predominantly enfortumab vedotin pretreated metastatic urothelial carcinoma population, suggesting that Nectin-4 remains an important and actionable therapeutic target following enfortumab vedotin-based therapy
- An objective response rate of 36% and disease control rate of 76% were observed at the highest dose level evaluated
- Tolerability of LY4101174 was primarily limited by grade 3+ hematologic toxicity, in particular neutropenia and febrile neutropenia, which persisted despite G-CSF prophylaxis
- The EXCEED study did not identify a dose that was both tolerable and sufficiently efficacious in participants with previously treated metastatic urothelial carcinoma
- Without a clear therapeutic window, development was discontinued
Presented by: Xin Gao, MD, Massachusetts General Hospital Cancer Center, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026