(UroToday.com) The 2026 ASCO annual meeting featured a urothelial carcinoma rapid abstract session and a presentation by Dr. Yohann Loriot discussing an interim analysis from Duravelo-2 assessing zelenectide pevedotin + pembrolizumab in patients with previously untreated locally advanced or metastatic urothelial carcinoma.
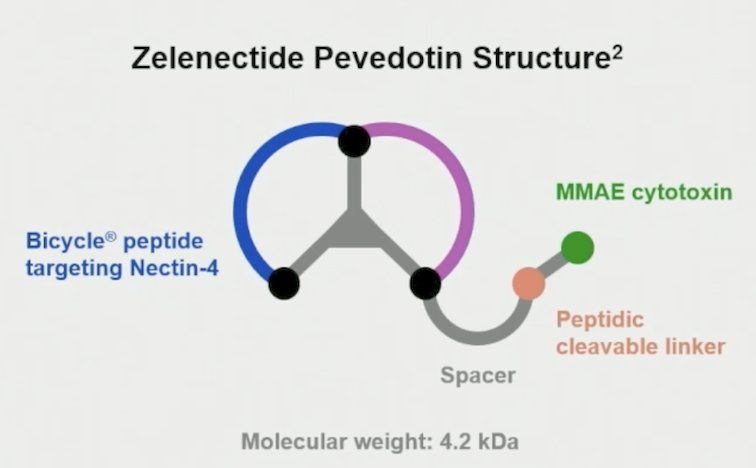
First line options for locally advanced or metastatic urothelial carcinoma may be limited by tolerability, and there remains an unmet need for safer treatments. The current standard of care antibody drug conjugate is associated with high rates of grade ≥3 skin reactions, and antibody drug conjugate-related events led to 30% of patients discontinuing therapy. Zelenectide pevedotin is a highly selective bicycle drug conjugate targeting Nectin-4, a protein overexpressed in locally advanced or metastatic urothelial carcinoma:
In an expansion cohort of the phase 1 Duravelo-1 study in cisplatin-ineligible patients, many with poor performance status, zelenectide pevedotin + pembrolizumab showed promising preliminary anti-tumor activity (50% clinical objective response rate), and a potentially differentiating safety profile from currently available antibody drug conjugates. At ASCO 2026, Dr. Loriot reported an interim analysis for zelenectide pevedotin + pembrolizumab dosage selection from the Phase 2/3 Duravelo-2 study (NCT06225596/BT8009-230) in previously untreated patients with locally advanced or metastatic urothelial carcinoma.
Adults with locally advanced or metastatic urothelial carcinoma were enrolled into 2 cohorts: previously untreated patients eligible for platinum-based chemotherapy (Cohort 1) or patients with ≥1 prior systemic therapy (cohort 2). Interim analysis was conducted to determine the optimized dosage of zelenectide pevedotin + pembrolizumab (cohort 1) or zelenectide pevedotin monotherapy (cohort 2). Specific to ASCO 2026, Dr. Loriot and colleagues reported the interim analysis results from cohort 1. Patients in cohort 1 were randomized 1:1:1 to: zelenectide pevedotin 5 mg/m² on Days [D]1/8/15 + pembrolizumab 200 mg on D1 versus zelenectide pevedotin 6 mg/m² on D1/8 + pembrolizumab 200 mg on D1 versus gemcitabine + cisplatin/carboplatin ± avelumab on a 21-D cycle:
![Adults with locally advanced or metastatic urothelial carcinoma were enrolled into 2 cohorts: previously untreated patients eligible for platinum-based chemotherapy (Cohort 1) or patients with ≥1 prior systemic therapy (cohort 2). Interim analysis was conducted to determine the optimized dosage of zelenectide pevedotin + pembrolizumab (cohort 1) or zelenectide pevedotin monotherapy (cohort 2). Specific to ASCO 2026, Dr. Loriot and colleagues reported the interim analysis results from cohort 1. Patients in cohort 1 were randomized 1:1:1 to: zelenectide pevedotin 5 mg/m² on Days [D]1/8/15 + pembrolizumab 200 mg on D1 versus zelenectide pevedotin 6 mg/m² on D1/8 + pembrolizumab 200 mg on D1 versus gemcitabine + cisplatin/carboplatin ± avelumab on a 21-D cycle:](/images/com-doc-importer/272-asco-2026/asco-2026-interim-analysis-from-duravelo-2-zelenectide-pevedotin-pembrolizumab-in-patients-with-previously-untreated-locally-advanced-or-metastatic-urothelial-carcinoma/image-1.jpg)
Dosage optimization included safety, efficacy, and pharmacokinetic data in pharmacometric and utility score analyses to quantify benefit-risk.
The interim analysis was performed at 27 weeks of follow-up (n = 30 each zelenectide pevedotin dose group). The baseline characteristics of this cohort are highlighted in the following table:

Zelenectide pevedotin-related adverse events were reported in 97% (47% grade ≥3) of patients at 5 mg/m² and 90% (40% grade ≥3) at 6 mg/m²:
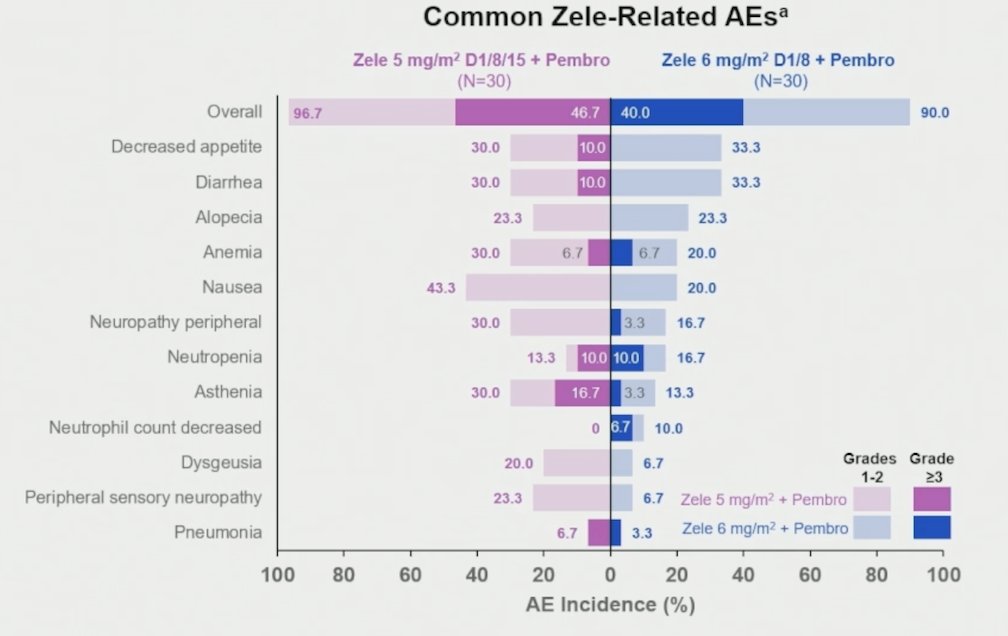
Grade ≥3 zelenectide pevedotin-related adverse events for 6 mg/m² (≥5% patients) included neutropenia (10%), neutrophil count decreased (7%), and anemia (7%). Adverse events related to pembrolizumab were reported in 80% (37% grade ≥3) and 53% (13% grade ≥3), respectively. Zelenectide pevedotin-related adverse events of clinical interest for 6 mg/m² are summarized in the following table:
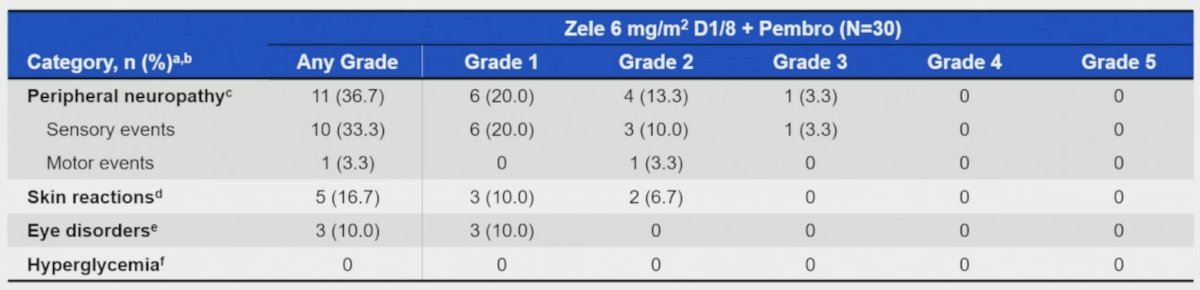
Notably, no zelenectide pevedotin-related severe skin reactions of any grade were reported at the 6 mg/m² dosage. Zelenectide pevedotin dose reductions and discontinuations due to zelenectide pevedotin-related adverse events occurred in 20% and 3%, respectively, for 6 mg/m².
The median zelenectide pevedotin treatment duration was 6.3 months (range: 0.7-10.6). Confirmed objective response rates by BICR among randomized, dosed patients with measurable disease at baseline were 55% (16/29; 7 complete responses, 9 partial responses; 95% CI 35.7–73.6) and 58% (15/26; 8 complete responses, 7 partial responses; 95% CI 36.9–76.6) with zelenectide pevedotin 5 mg/m² and 6 mg/m², respectively:
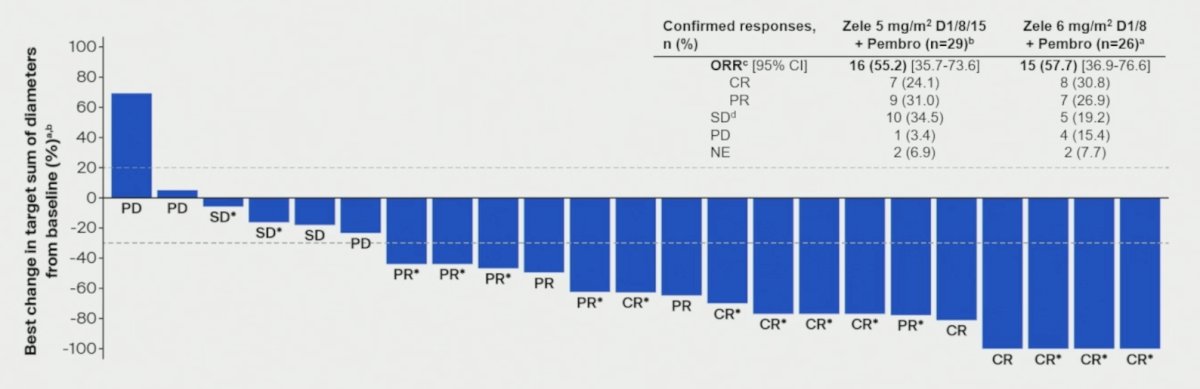
The duration of response and change from baseline in tumor size with zelenectide pevedotin 6 mg/m2 D1/8 + pembrolizumab is noted in the following plot:

There were 15/23 (65.2%) efficacy evaluable patients receiving a 6 mg/m² dosage that remained on treatment at the data extraction.
Dr. Loriot concluded his presentation discussing an interim analysis from Duravelo-2 with the following take-home points:
- Zelenectide pevedotin at 5 mg/m² on D1/8/15 + pembrolizumab and 6 mg/m² on D1/8 + pembrolizumab demonstrated encouraging response rates and favorable safety profiles with the potential to differentiate from antibody drug conjugates in previously untreated patients with locally advanced or metastatic urothelial carcinoma
- The 6 mg/m² on D1/8 dosage of zelenectide pevedotin was identified as the optimized dosage, demonstrating a favorable benefit-risk profile, and meeting the need for safer and more tolerable treatments.
- Zelenectide pevedotin + pembrolizumab had low rates of adverse events, especially those that limit the administration of other antibody drug conjugates used in locally advanced or metastatic urothelial carcinoma
- Tolerability was improved with 6 mg/m² over the 5 mg/m² dose, with increased potential for combinability and enhanced convenience
- Skin toxicity with zelenectide pevedotin + pembrolizumab was low grade and manageable
- As of 18 June 2025, in 595 patients treated with zelenectide pevedotin, no events of Stevens-Johnson syndrome or toxic epidermal necrolysis were reported, demonstrating an improved safety profile compared with currently available antibody drug conjugate regimens.
Presented by: Yohann Loriot, MD, PhD, Gustave Roussy, Paris, France
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026