(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a kidney and bladder cancers poster session. Dr. Prateek Jain presented a cost-effectiveness analysis comparing contemporary first-line treatment strategies for advanced urothelial carcinoma (aUC) from a U.S. payer perspective. Specifically, the study evaluated gemcitabine/cisplatin followed by avelumab maintenance (GC+AVEL), gemcitabine/cisplatin plus nivolumab (GC-NIVO), and enfortumab vedotin plus pembrolizumab (EV + pembro).
Management of advanced urothelial carcinoma has evolved substantially following the approval of EV + pembro and GC-NIVO in the frontline setting.1,2 While these regimens have improved clinical outcomes, their relative economic value remains uncertain, particularly given the high costs associated with novel combination therapies. This study sought to evaluate the comparative cost-effectiveness of currently available first-line regimens using updated 2026 U.S. pricing data.
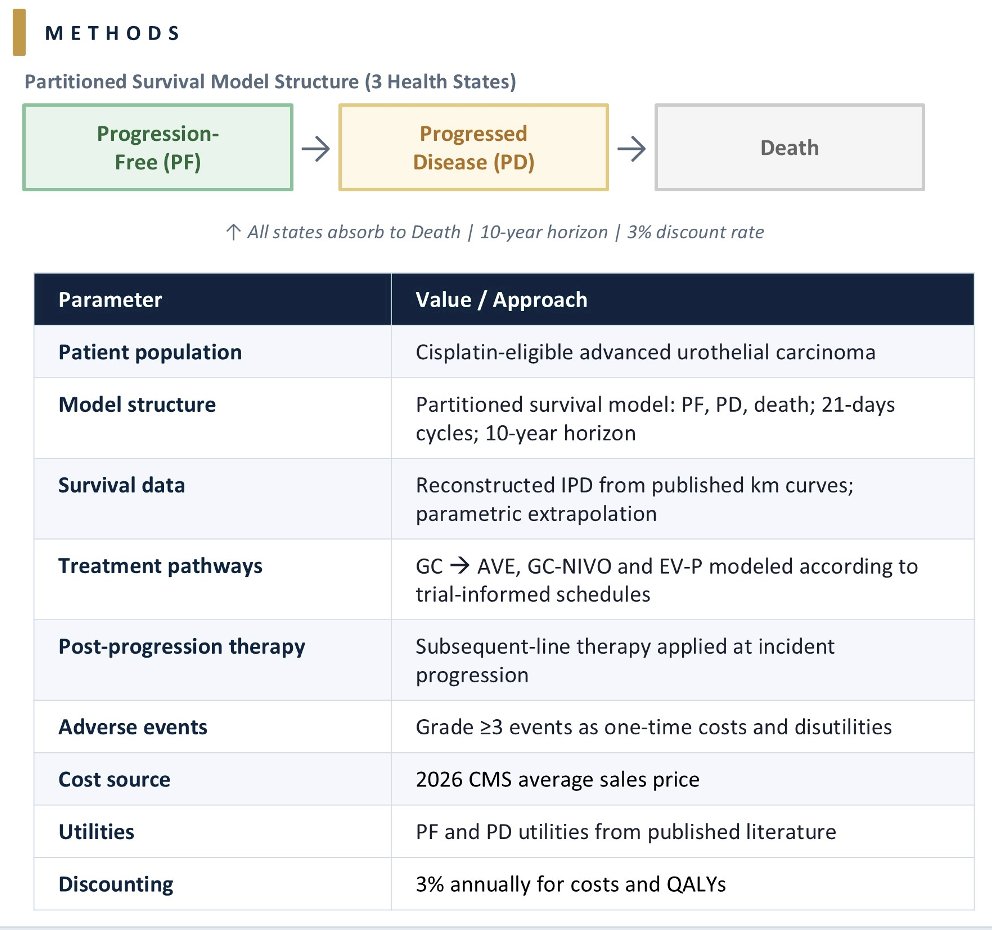
Investigators developed a partitioned survival model incorporating three health states:
- Progression-free disease
- Progressed disease
- Death
The analysis was conducted from a U.S. payer perspective over a 10-year time horizon and focused on cisplatin-eligible patients. Survival outcomes were reconstructed from published Kaplan–Meier curves and extrapolated using parametric survival models. Treatment schedules and duration were modeled according to clinical trial protocols. Patients receiving gemcitabine/cisplatin without progression were modeled to subsequently receive avelumab maintenance therapy.
Additional modeling assumptions included:
- Subsequent-line therapy costs applied at progression
- Grade ≥3 adverse event costs and disutilities incorporated as one-time events
- Drug acquisition costs based on the 2026 Centers for Medicare & Medicaid Services average sales prices
- Costs and quality-adjusted life years (QALYs) discounted annually at 3%
The primary economic endpoints included:
- Incremental cost-effectiveness ratios (ICERs)
- Net monetary benefit (NMB)
These were evaluated using willingness-to-pay (WTP) thresholds of:
- $100,000/QALY
- $150,000/QALY
- $200,000/QALY
In the base-case analysis:
- GC+AVEL:
- Total discounted cost: $90,269
- QALYs: 1.62
- GC-NIVO:
- Total discounted cost: $131,836
- QALYs: 2.09
- EV + pembro:
- Total discounted cost: $1,451,885
- QALYs: 2.77

Compared with GC+AVEL:
- GC-NIVO gained 0.46 QALYs
- Incremental cost: $41,567
- ICER: $89,501/QALY
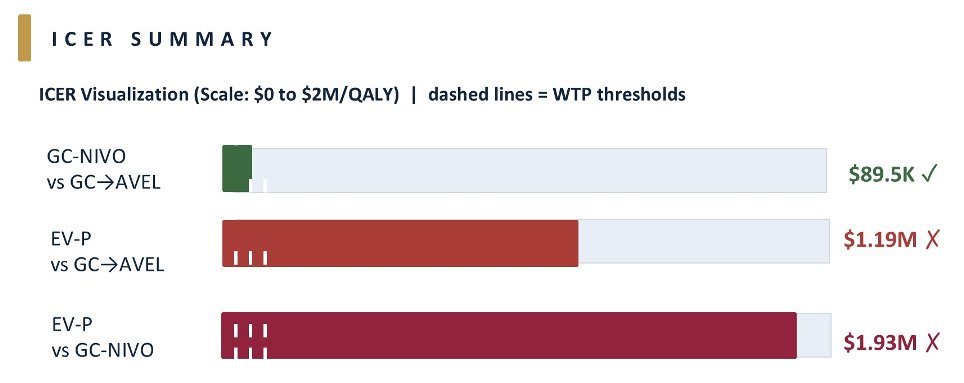
Importantly, GC-NIVO demonstrated positive net monetary benefit across all evaluated willingness-to-pay thresholds, supporting its cost-effectiveness relative to GCAVEL.
In contrast, EV + pembro demonstrated substantially higher costs:
- Compared with GC+AVEL:
- QALY gain: 1.15
- Incremental cost: $1.36 million
- ICER: $1.19 million/QALY
- Compared with GC-NIVO:
- QALY gain: 0.68
- Incremental cost: $1.32 million
- ICER: $1.93 million/QALY
These ICERs substantially exceeded all evaluated willingness-to-pay thresholds, indicating that EV + pembro was not cost-effective at the current pricing despite providing the greatest clinical benefit.
The investigators additionally performed a scenario analysis limiting EV + pembro treatment duration to 10 cycles. Under this model:
- Total EV + pembro costs decreased to $287,360
- ICER versus GCAVEL: $172,000/QALY
- ICER versus GC-NIVO: $225,000/QALY
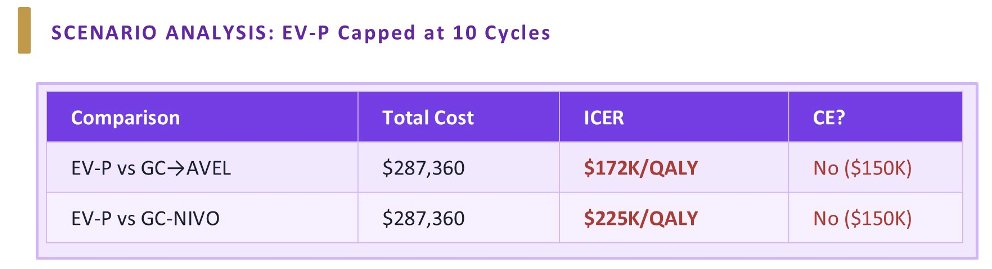
However, even with shortened treatment duration, EV + pembro remained above the commonly utilized $150,000/QALY willingness-to-pay threshold.
The investigators concluded that, using updated 2026 U.S. pricing data, GC-NIVO is likely the most cost-effective frontline regimen for cisplatin-eligible patients with advanced urothelial carcinoma. Although EV + pembro provided the greatest clinical benefit, it was not cost-effective at current prices. The authors emphasized that an important limitation of this analysis was cross-trial variability in study populations and trial design, which limits the strength of indirect economic comparisons across regimens.
Presented by: Prateek Jain, MBBS, Tata Medical Center, Kolkata, India
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:- Powles T, Valderrama BP, Gupta S, et al. Enfortumab Vedotin and Pembrolizumab in Untreated Advanced Urothelial Cancer. N Engl J Med. 2024;390:875-888.
- van der Heijden MS, Sonpavde G, Powles T, et al. Nivolumab Plus Gemcitabine-Cisplatin in Advanced Urothelial Carcinoma. N Engl J Med. 2023;389:1778-1789.