(UroToday.com) The 2026 ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Abhishek Srivastava discussing UTOPIA, a phase 3 trial of UGN-103, an intravesical mitomycin reverse thermal hydrogel, in recurrent low-grade intermediate risk non-muscle invasive bladder cancer. Management of recurrent low-grade, intermediate risk non-muscle invasive bladder cancer remains challenging due to frequent recurrence following standard surgical management with TURBT.
UGN-102 is an intravesical mitomycin reverse thermal hydrogel, approved by the FDA for treatment of adults with recurrent low-grade, intermediate-risk non-muscle invasive bladder cancer based on the phase 3 ENVISION trial.1 ENVISION demonstrated a complete response rate of 80% (95% CI 74, 85) at 3 months, with an 82% (95% CI 76, 87) and 72% (95% CI 64, 79) probability of remaining in response 12 and 24 months from initial complete response at 3 months, respectively. UGN-103 is a novel formulation of UGN-102 developed to simplify drug preparation and shorten manufacturing time.
UTOPIA (NCT06331299) is an ongoing, multicenter, single-arm, phase 3 study evaluating UGN-103 as primary treatment for adults with recurrent low-grade, intermediate risk non-muscle invasive bladder cancer. Eligible patients provided written informed consent and received six once-weekly intravesical instillations of UGN-103 (mitomycin 75 mg in 56 mL admixture). Disease assessment was performed 3 months after the start of treatment. Patients with no detectable disease entered a follow-up period, with evaluations every 3 months until recurrence, progression, death, or completion of follow-up (12 months after the 3-month visit):
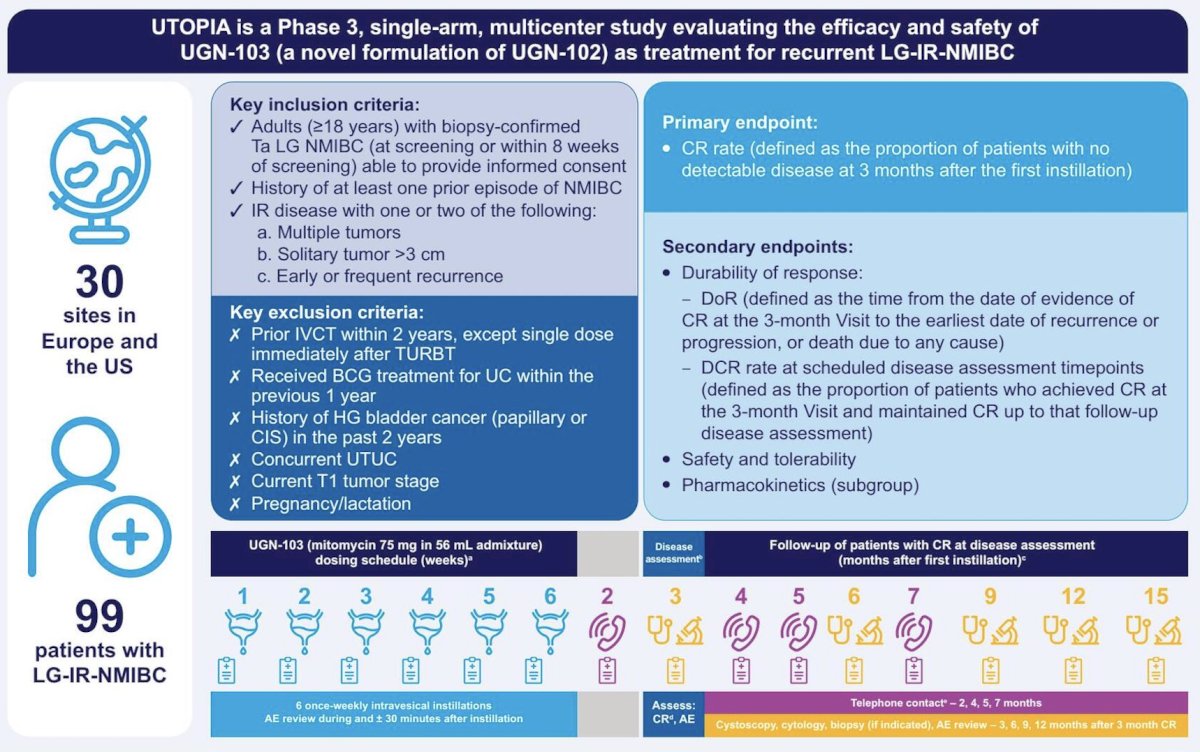
The primary endpoint was complete response rate (defined as the proportion of patients assessed as having no evidence of disease at the 3-month visit) based on cystoscopy, for-cause biopsy, and urine cytology. Secondary endpoints include durability of response, safety and tolerability, and pharmacokinetics. For this analysis, the data cut-off was September 3, 2025.
A total of 99 patients received ≥1 instillation of UGN-103. Among these patients, 97% (n = 96) received all 6 instillations. At baseline, the median patient age was 71 years (range: 46, 93), with 78% (n = 77) being ≥65 years old. Most patients were male (72%; n = 71), and 99% (n = 98) were White. Most patients had multiple tumors (83.2%; n = 79), with the longest tumor diameter being ≤3 cm in 86.7% (n = 78):

At 3 months, 77 of 99 patients in the intent-to-treat population achieved a complete response (complete response rate: 77.8% [95% CI 68.3, 85.5]). Non-complete response outcomes included 22.2% of patients, and were most commonly due to residual disease:
![At 3 months, 77 of 99 patients in the intent-to-treat population achieved a complete response (complete response rate: 77.8% [95% CI 68.3, 85.5]). Non-complete response outcomes included 22.2% of patients, and were most commonly due to residual disease:](/images/com-doc-importer/272-asco-2026/asco-2026-utopia-a-phase-3-trial-of-ugn-103-an-intravesical-mitomycin-reverse-thermal-hydrogel-in-recurrent-low-grade-intermediate-risk-nmibc/image-2.jpg)
The median following in the intention-to-treat population, measured from treatment initiation to data cutoff, was 6.1 months (IQR 3.2, 7.2), and the median duration of response is not yet estimable. The median follow-up for the duration of response was 2.43 months (95% CI 0.03, 2.83). Treatment-emergent adverse events were reported in 59.6% of patients, with the most common treatment-emergent adverse events being mild to moderate in severity and were resolved/resolving:

Treatment-emergent adverse events leading to treatment discontinuation occurred in 3.0% of patients, and no events led to study discontinuation or death. Serious treatment-emergent adverse events were reported in 2.0% of patients, including atrial fibrillation, osteoarthritis, and respiratory failure, of which none were treatment-related:

The most frequently reported treatment-emergent adverse events (>= 5%) were dysuria (19.2%), fatigue (9.1%), pollakiuria (8.1%), urinary tract infection (7.1%), and hematuria (6.1%):
Dr. Srivastava concluded his presentation discussing UTOPIA, a phase 3 trial of UGN-103 in recurrent low-grade intermediate risk non-muscle invasive bladder cancer, with the following take-home points:
- UGN-103 demonstrated a safety and efficacy profile similar to that observed with UGN-102 in patients with recurrent low-grade, intermediate-risk non-muscle invasive bladder cancer
- 78% complete response rate achieved at 3 months, similar to UGN-102 (80%)
- A consistent safety profile was observed, with low serious adverse event incidence
- These results support further evaluation of UGN-103 as an intravesical treatment option for recurrent low-grade, intermediate-risk non-muscle invasive bladder cancer
Presented by: Abhishek Srivastava, MD, Carolina Urologic Research Center, Myrtle Beach, SC
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
Reference: