(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a kidney and bladder cancers oral abstract session. Dr. Yijun Shen presented the results of a phase 2/3 trial evaluating perioperative SHR-A2102, a novel nectin-4-targeted antibody-drug conjugate (ADC), in combination with adebrelimab for patients with muscle invasive bladder cancer (MIBC).
MIBC remains an aggressive disease with a substantial recurrence risk following radical cystectomy and pelvic lymph node dissection. SHR-A2102 is a novel ADC composed of an anti–nectin-4 monoclonal antibody linked to a topoisomerase I inhibitor payload via a cleavable linker. Given the success of nectin-4 targeting in advanced urothelial carcinoma and the growing role of immune checkpoint inhibition, investigators hypothesized that perioperative SHR-A2102 + adebrelimab may improve pathologic response rates while maintaining surgical feasibility.
This multicenter, open-label phase 2/3 study (NCT06879145) enrolled patients with pathologically and radiographically confirmed T2–4aN0M0 or T1–4aN1M0 MIBC who were eligible for radical cystectomy and pelvic lymph node dissection, had an ECOG performance status of 0–1, and adequate organ function, including a creatinine clearance ≥30 mL/min.
Eligible participants were planned for the following:
- Neoadjuvant SHR-A2102 8 mg/kg plus adebrelimab 1,200 mg every 3 weeks for four cycles
- Radical cystectomy within six weeks of completion of neoadjuvant therapy
- Adjuvant SHR-A2102 8 mg/kg plus adebrelimab 1,200 mg every 3 weeks for up to 13 cycles
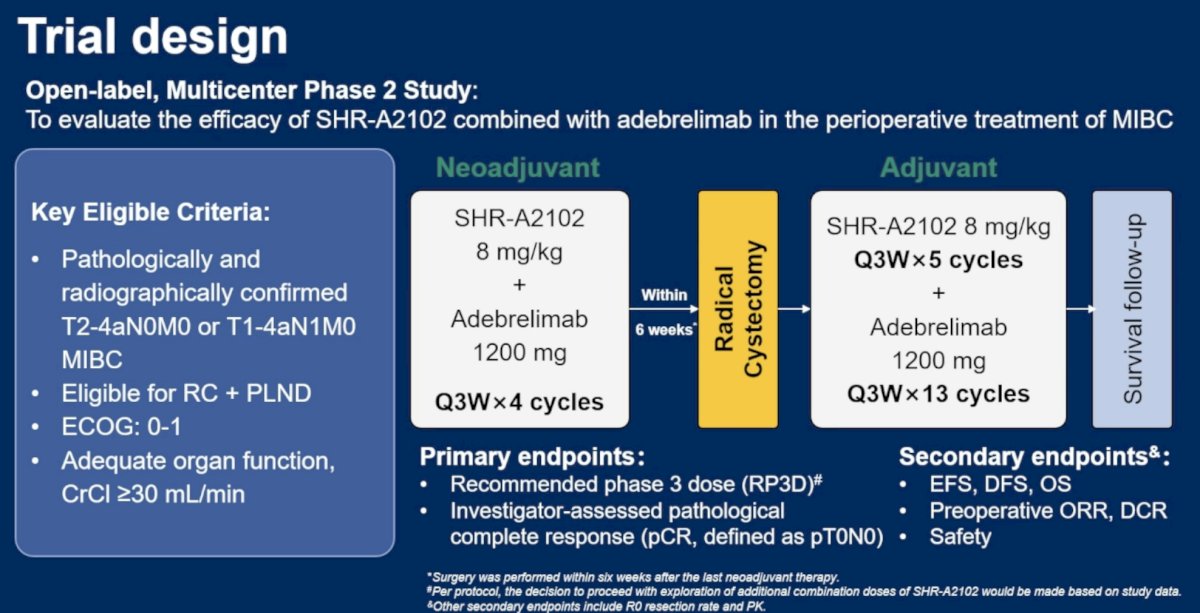
The co-primary endpoints for the phase 2 portion were determination of the recommended phase 3 dose and investigator-assessed pathologic complete response (pCR; ypT0N0). Secondary endpoints included:
- Event-free survival (EFS)
- Disease-free survival (DFS)
- Overall survival (OS)
- Preoperative objective response rate (ORR)
- Disease control rate (DCR)
- Safety.
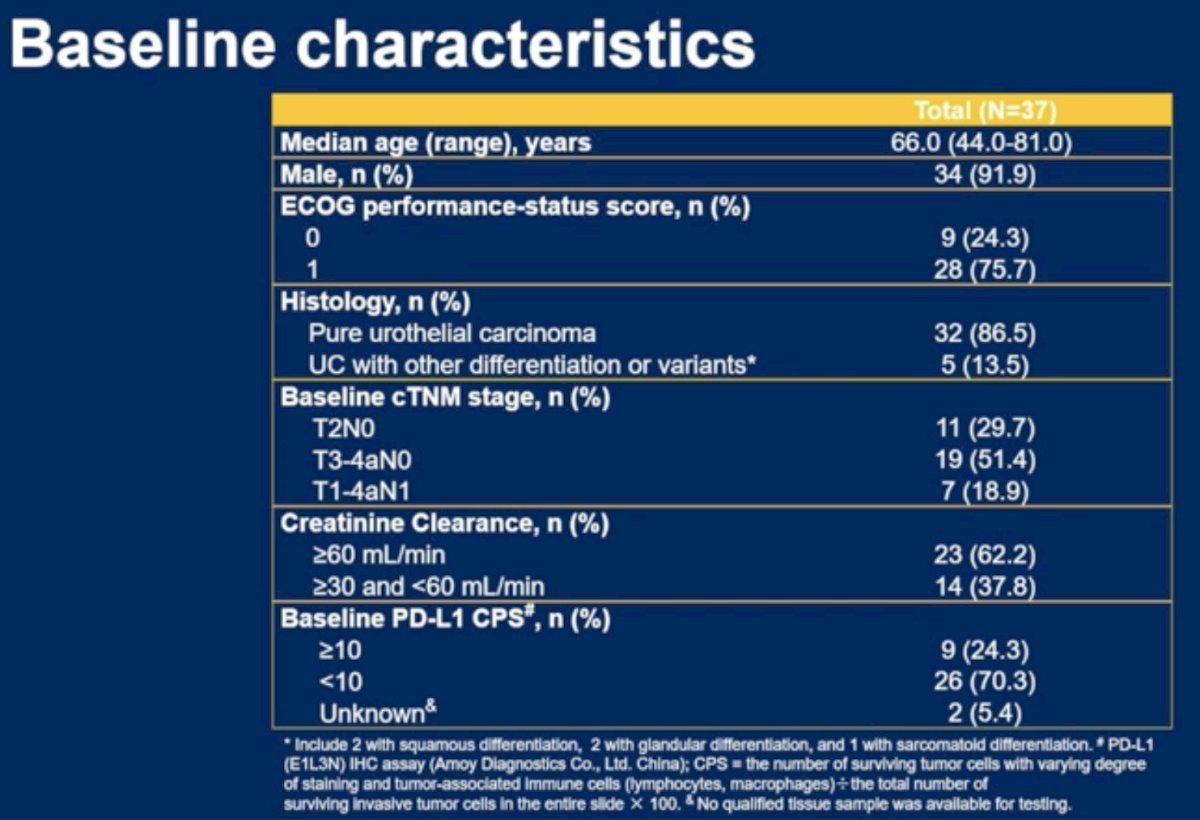
At the November 24, 2025 data cutoff, 37 patients had been enrolled. Baseline characteristics were as follows:
- Median age: 66 years (range: 44–81)
- Male: 91.9% (34/37)
- ECOG performance status:
- 0: 24.3%
- 1: 75.7%
- Histology:
- Pure urothelial carcinoma: 86.5%
- Variant histology: 13.5%
- Clinical stage:
- T2N0: 29.7%
- T3–4aN0: 51.4%
- T1–4aN1: 18.9%
- Creatinine clearance:
- ≥60 mL/min: 62.2%
- 30–59 mL/min: 37.8%
- PD-L1 CPS:
- ≥10: 24.3%
- <10: 70.3%
- Unknown: 5.4%
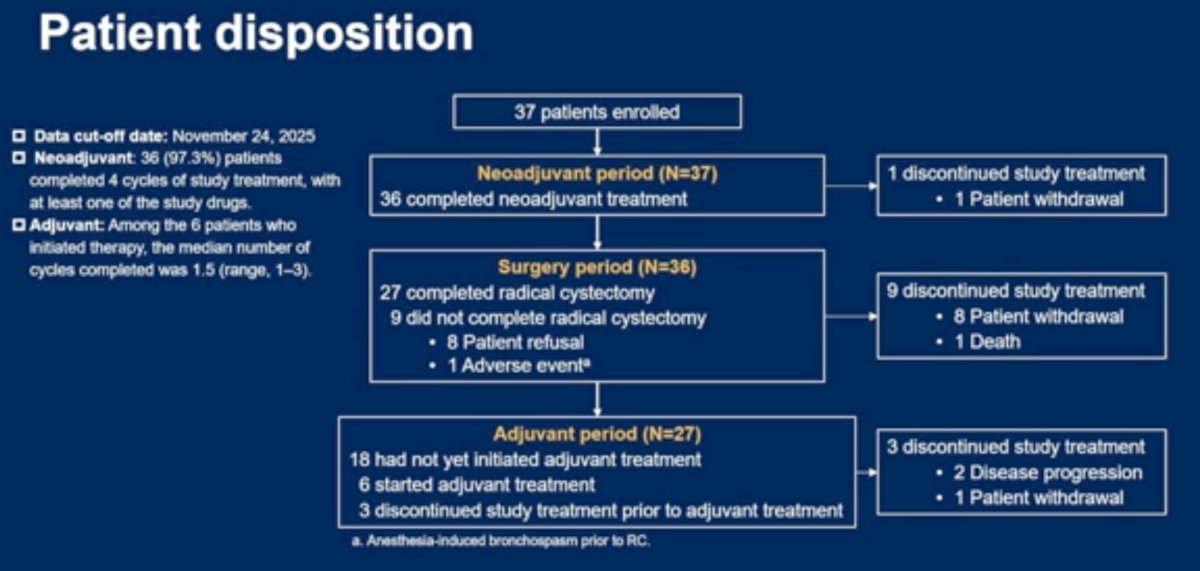
With regards to patient disposition:
- Thirty-six of 37 patients (97.3%) completed all four neoadjuvant cycles
- One patient discontinued neoadjuvant therapy due to withdrawal
- Thirty-six patients proceeded to the surgical period
- Twenty-seven patients completed radical cystectomy
- Nine patients did not undergo cystectomy:
- Eight due to patient refusal
- One due to an adverse event
Among the 27 patients who underwent surgery and were evaluable for pathologic response:
- pCR (ypT0N0): 48.1% (13/27)
- Pathologic downstaging to <ypT2N0: 59.3% (16/27)
Among the nine patients who completed neoadjuvant therapy but declined radical cystectomy, five subsequently underwent TURBT, with three patients (60%) demonstrating no evidence of residual tumor.

Radiographic responses were assessed in the seven patients with measurable target lesions at baseline:
- Complete response: 1 patient
- Partial response: 4 patients
- Stable disease: 2 patients
- Progressive disease: 0 patients
This translated into:
- ORR: 71.4% (5/7; 95% CI: 29.0–96.3)
- DCR: 100% (7/7; 95% CI: 59.0–100.0)
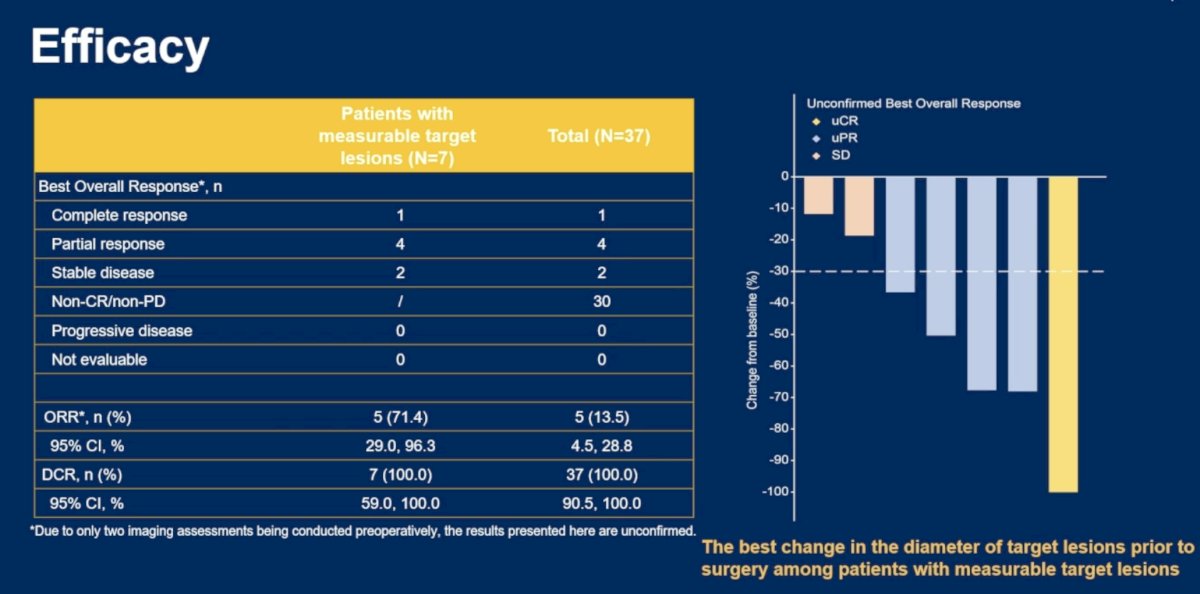
Waterfall plot analysis demonstrated tumor shrinkage in all evaluable patients with measurable disease, including one patient achieving complete radiographic resolution.
Subgroup analyses suggested pCR benefit across all predefined patient groups:
- T2N0 disease: 77.8%
- T3–4aN0 disease: 18.2%
- T1–4aN1 disease: 57.1%
- Creatinine clearance ≥60 mL/min: 47.1%
- Creatinine clearance 30–59 mL/min: 50.0%
- Renal impairment did not appear to adversely affect pathologic response rates, supporting potential applicability in cisplatin-ineligible patients.
- PD-L1 CPS ≥10: 62.5%
- PD-L1 CPS <10: 42.1%
With a median follow-up of 4.7 months (IQR: 2.1–6.6), three EFS events had occurred and median EFS had not yet been reached.
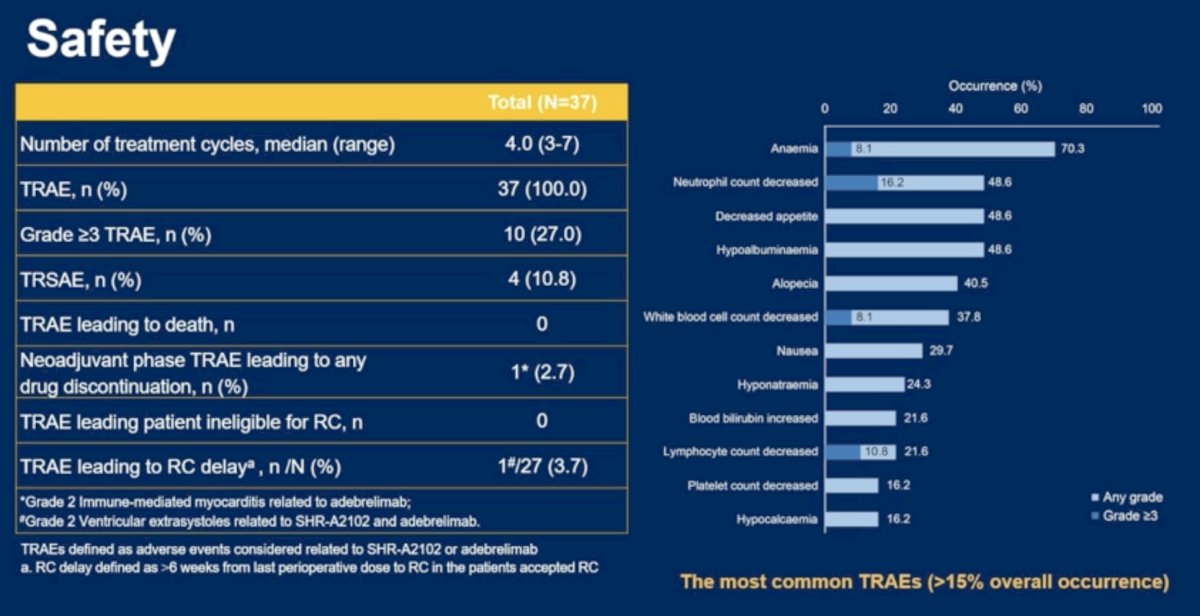
Safety outcomes were encouraging. The median number of treatment cycles administered was four (range: 3–7). The key safety findings were as follows:
- Any-grade treatment-related adverse events (TRAEs): 100%
- Grade ≥3 TRAEs: 27.0% (10/37)
- Treatment-related serious adverse events: 10.8% (4/37)
- TRAEs leading to death: 0
- TRAEs leading to treatment discontinuation during neoadjuvant therapy: 2.7% (1 patient)
- TRAEs rendering patients ineligible for surgery: 0
- TRAEs resulting in surgical delay: 3.7% (1/27)
The most common TRAEs were:
- Anemia: 70.3% (Grade ≥3: 8.1%)
- Decreased neutrophil count: 48.6% (Grade ≥3: 16.2%)
- Decreased appetite: 48.6%
- Hypoalbuminemia: 48.6%
- Alopecia: 40.5%
Importantly, no patient became ineligible for radical cystectomy because of treatment-related toxicity, highlighting the favorable perioperative tolerability of the regimen.
The investigators concluded as follows:
- In this preliminary analysis, perioperative SHR-A2102 plus adebrelimab demonstrated promising antitumor activity and manageable toxicity in patients with MIBC.
- The regimen achieved a pCR rate of 48.1% and pathologic downstaging rate of 59.3%, with consistent activity across predefined subgroups, including patients with impaired renal function.
- Furthermore, no treatment-related adverse events prevented surgery, supporting continued development of this nectin-4–targeted ADC plus PD-L1 inhibition strategy in the perioperative setting.
- Longer follow-up and completion of the ongoing phase 2/3 program will further define the durability of these responses and the impact on long-term oncologic outcomes.
Presented by: Yijun Shen, MD, Professor, Fudan University Shanghai Cancer Center, Shanghai, China
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026