(UroToday.com) The 2026 American Society of Clinical Oncology (ASCO) Annual Meeting was host to a kidney and bladder cancers oral abstract session. Dr. Richard Cathomas presented the primary analysis of SAKK 06/19 evaluating intravesical recombinant BCG combined with chemotherapy + immunotherapy (chemi0IO) as perioperative therapy for patients with muscle invasive bladder cancer (MIBC).
The integration of immunotherapy in the perioperative setting of MIBC is feasible, as demonstrated in SAKK 06/17,1 and improves event-free survival (EFS) and overall survival (OS) compared to chemotherapy alone, as shown in NIAGARA.2 Although pathological complete response (pCR) rates are improved, they remain below 40%. Intravesical BCG has been used for decades in non-muscle invasive bladder cancer (NMIBC), where it induces a local inflammatory response leading to activation of the innate immune system, followed by a tumor-active immune response. A novel recombinant BCG (VPM1002BC, rBCG) has been developed, and a clinical study in BCG-exposed NMIBC previously demonstrated safety and promising efficacy (SAKK 06/14).3 Based on these observations, the study investigators hypothesized that induction therapy with intravesical rBCG would improve the efficacy of systemic perioperative chemo-immunotherapy in patients with operable MIBC.
Recombinant BCG (rBCG, VPM1002BC) was developed through the exchange of the Urease C gene with the hemolysine listeriolysin gene from Listeria monocytogenes. It was engineered for improved immunogenicity, whereby egress of antigens promotes adaptive immune responses through cross-presentation to MHC-I and egress of dsDNA induces innate immune responses. It was also engineered for improved safety through more rapid elimination by autophagy, reducing persistence.
SAKK 06/19 was designed as a prospective, single-arm, open-label, multicenter phase II trial. Eligible patients had cT2–T4a cN0/N1 urothelial carcinoma, WHO performance status 0–1, and were cisplatin fit with a GFR >50 mL/min. Histologic subtypes were permitted, although pure squamous and glandular tumors were excluded. Patients with prior intravesical BCG exposure or small-cell components were excluded.
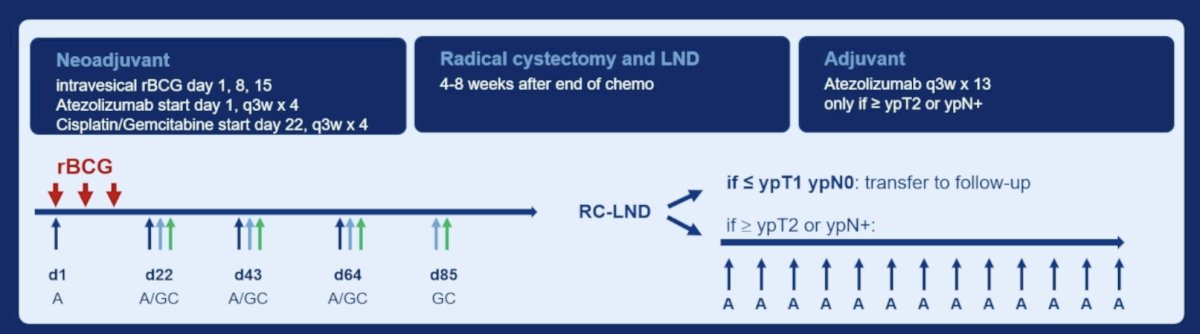
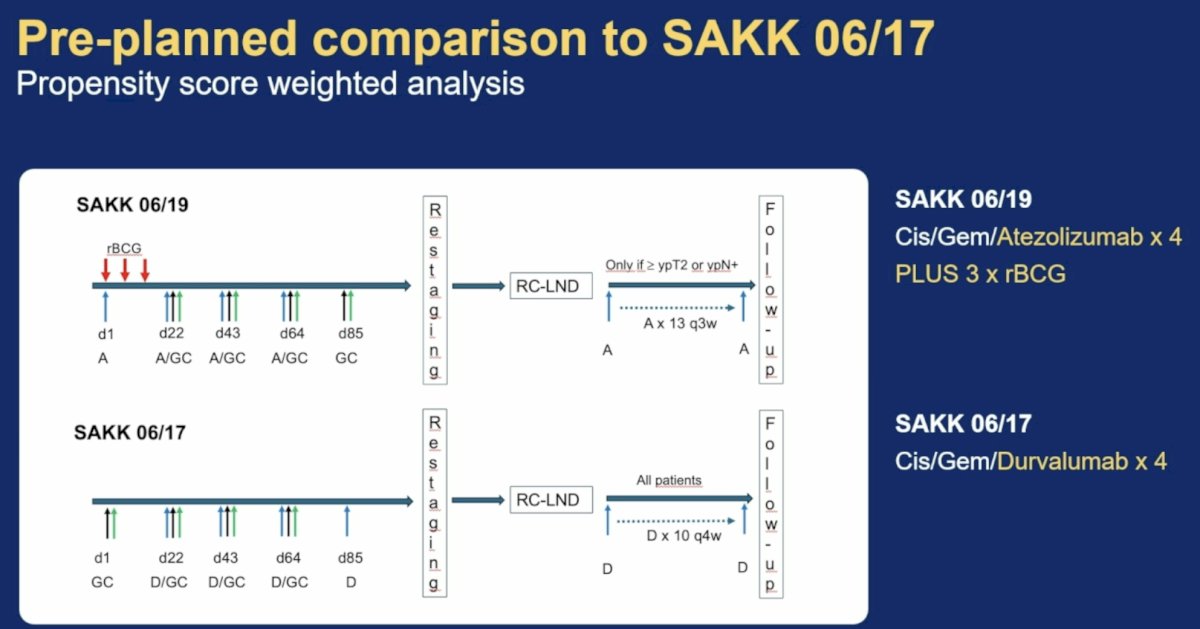
Patients received neoadjuvant intravesical rBCG on days 1, 8, and 15. Atezolizumab was initiated on day 1 and administered every three weeks for four cycles. Cisplatin/gemcitabine chemotherapy was initiated on day 22 and administered every three weeks for four cycles. Radical cystectomy and lymph node dissection were performed 4–8 weeks after completion of chemotherapy. Patients with residual ≥ypT2 disease or ypN+ disease received adjuvant atezolizumab every three weeks for 13 cycles, whereas patients with ≤ypT1 ypN0 disease proceeded to follow-up.
The primary endpoint was pCR (i.e., ypT0N0) at cystectomy with central review. The secondary endpoints included pathological response (PaR; ≤ypT1 ypN0), event-free survival, overall survival, feasibility, and safety.
The study was powered using a Simon minimax two-stage design. The null hypothesis assumed a pCR rate ≤35%, whereas the alternative hypothesis assumed a pCR rate ≥55%. With a type I error of 5% and power of 80%, 39 resected patients were required. The planned total sample size was 46 patients, accounting for a projected 15% dropout rate.
Between April 2022 and April 2025, 50 patients were screened, and 47 patients were included. Accrual was suspended between October 2022 and August 2023 due to out-of-specification rBCG requiring remanufacturing. Three patients failed screening, including one patient with localized peritoneal carcinomatosis, one patient receiving out-of-specification rBCG, and one patient withdrawal.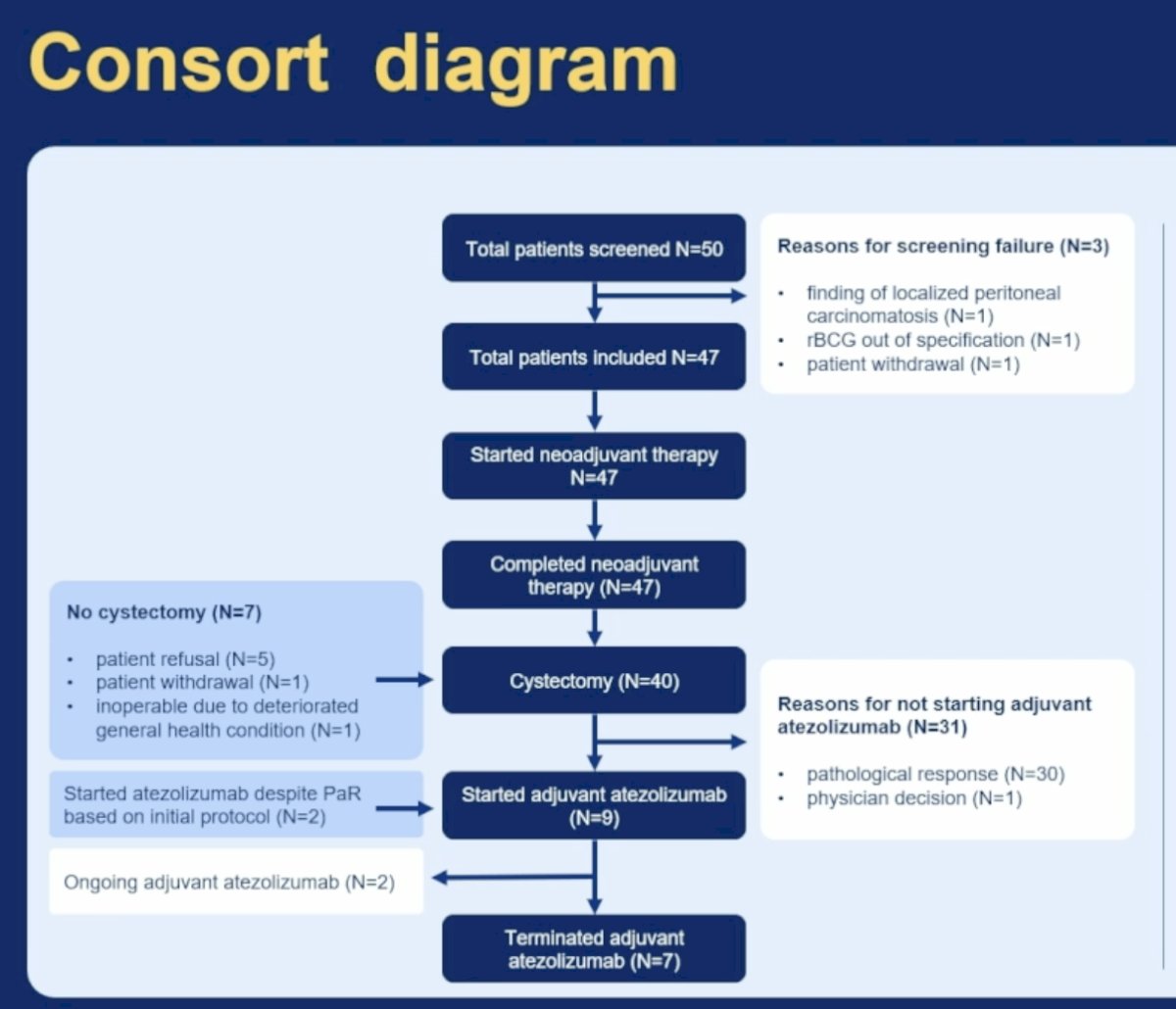
The full analysis set included 47 patients. All patients completed neoadjuvant treatment. Treatment delivery was excellent:
- 79% received all three planned doses of rBCG
- 92% received all four doses of atezolizumab
- 92% received four doses of platinum chemotherapy, including 81% who completed cisplatin and 19% who switched to carboplatin
- 87% received at least seven of eight planned gemcitabine doses
Seven patients did not undergo cystectomy, including six patients who refused surgery (one of whom withdrew consent) and one patient deemed unfit for surgery based on the physician's decision. Thirty-one patients did not receive adjuvant atezolizumab, including 30 patients according to protocol because they achieved ≤ypT1 ypN0 and one patient based on the physician's decision.
The baseline characteristics demonstrated a median age of 67 years (range 24–78). 81% were male. WHO performance status was 0 in 79% and 1 in 21%. The clinical stage at presentation was cT2 in 60%, cT3 in 32%, and cT4a in 8%. Eleven percent of patients had clinically node-positive disease. TURBT was macroscopically complete in 36% and macroscopically incomplete in 64%. Histology consisted of pure urothelial carcinoma in 77% and urothelial carcinoma with variant subtype in 23%.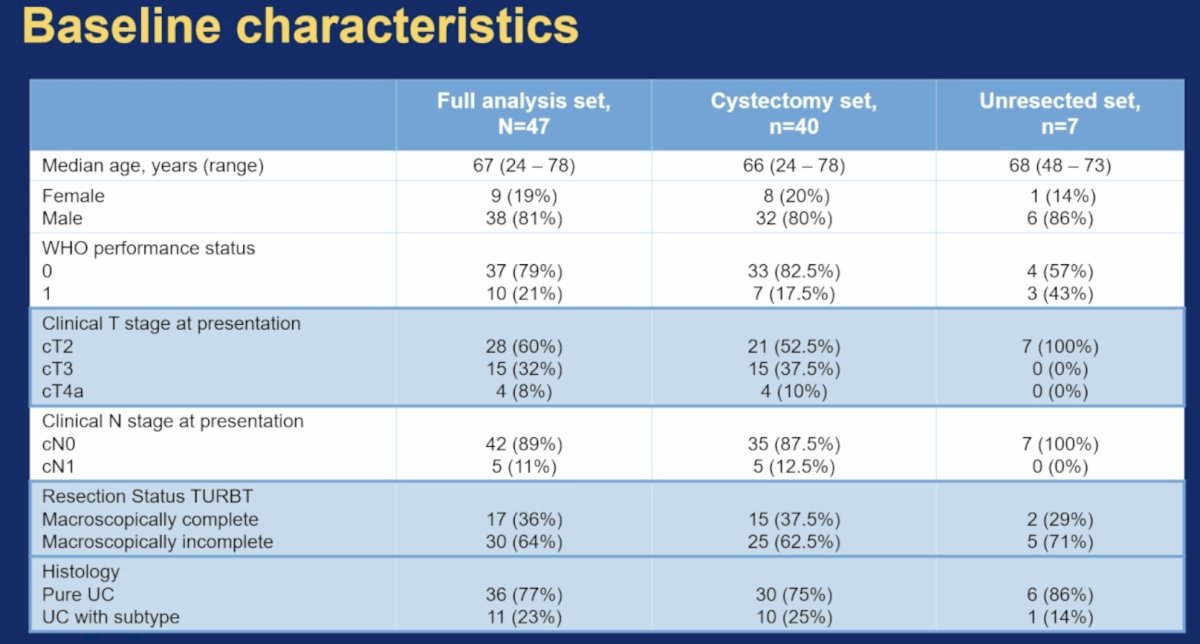
The primary endpoint analysis was performed in 40 centrally reviewed cystectomy specimens. pCR was achieved in 27 patients, corresponding to a pCR rate of 68% (27/40). The one-sided 95% confidence interval lower bound was 53%, and the null hypothesis was rejected (p<0.0001).
Pathological response (≤ypT1 ypN0) was achieved in 33 patients (83%). Seven patients (18%) did not achieve a pathological response.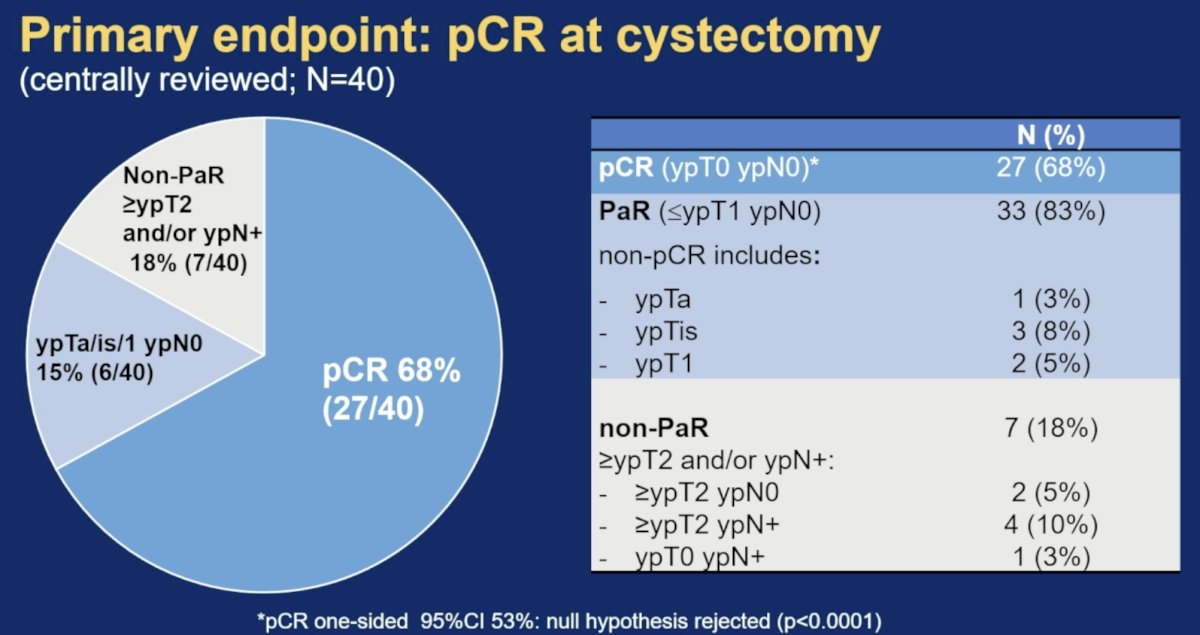
The investigators also evaluated the relationship between baseline clinical stage, clinical complete response (cCR), and pCR using a Sankey analysis. Clinical complete response was defined based on CT thorax/abdomen/pelvis, bladder MRI, cystoscopy, and urine cytology. Among 25 evaluable patients, cCR demonstrated a positive predictive value of 92% and a negative predictive value of 69% for predicting pathological complete response.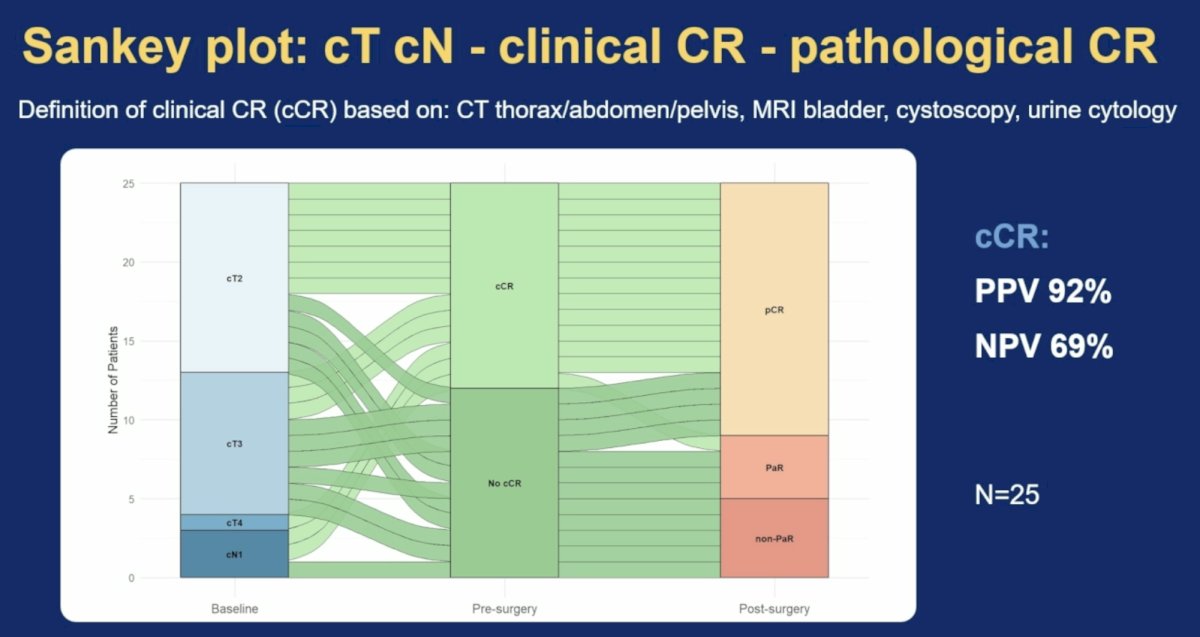
At a median follow-up of 16.7 months, secondary survival endpoints were favorable. Twelve-month EFS was 90% (95% CI 76%–96%), while 12-month OS was 96% (95% CI 84%–99%).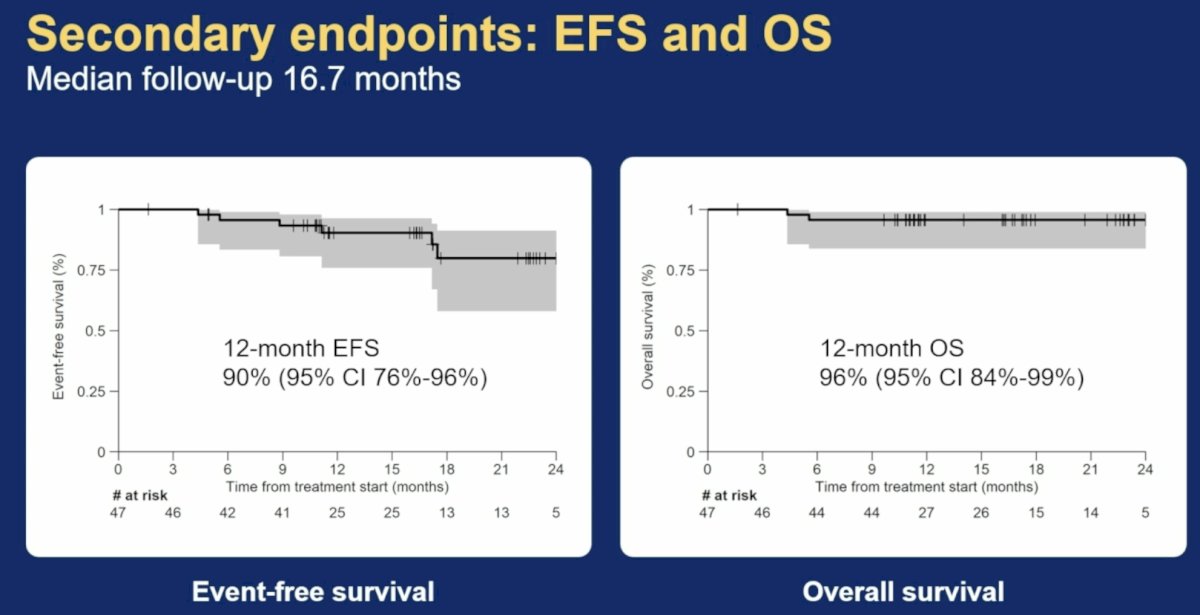
Treatment-related adverse events were evaluated according to CTCAE version 5. Among 45 patients evaluable for rBCG-related toxicity, grade 1, 2, and 3 adverse events occurred in 18%, 16%, and 9%, respectively, with no grade 4 events. For atezolizumab-related toxicity, grade 1, 2, 3, and 4 adverse events occurred in 19%, 19%, 15%, and 2% of patients, respectively. Chemotherapy-related adverse events occurred in 15%, 26%, 38%, and 17% of patients at grades 1, 2, 3, and 4, respectively. Importantly, no systemic BCG infection occurred.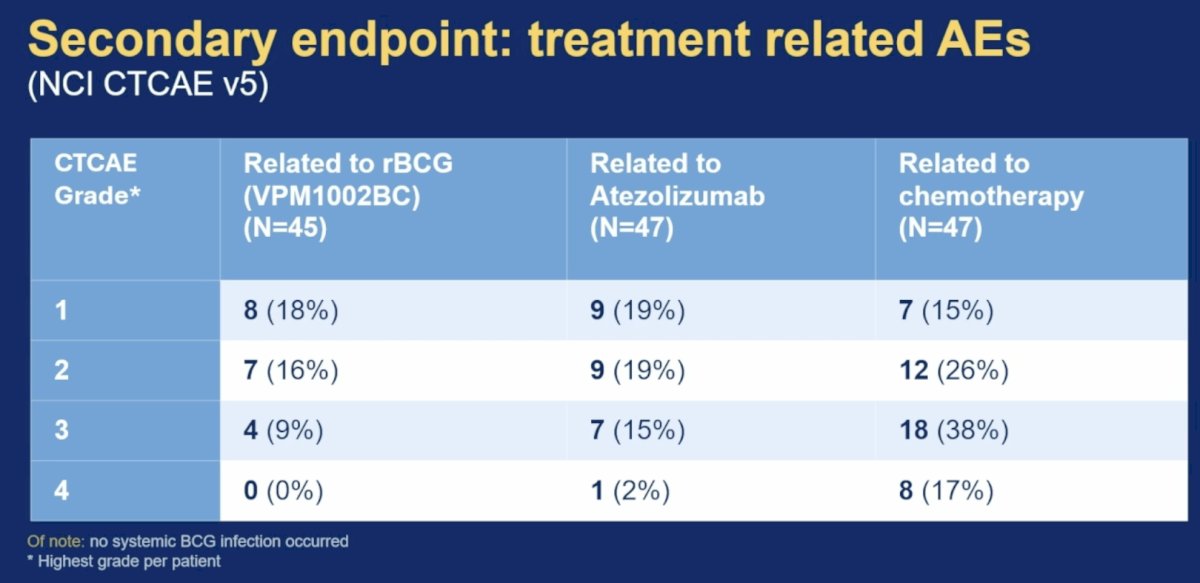
Treatment-related adverse events appeared to be largely driven by chemotherapy. Overall, the most common adverse events were decreased neutrophil count (55%), nausea (47%), fatigue (45%), renal impairment (44%), and decreased platelet count (33%). Grade 3/4 adverse events were predominantly neutropenia, thrombocytopenia, urinary tract infections, anemia, thromboembolic events, and renal impairment.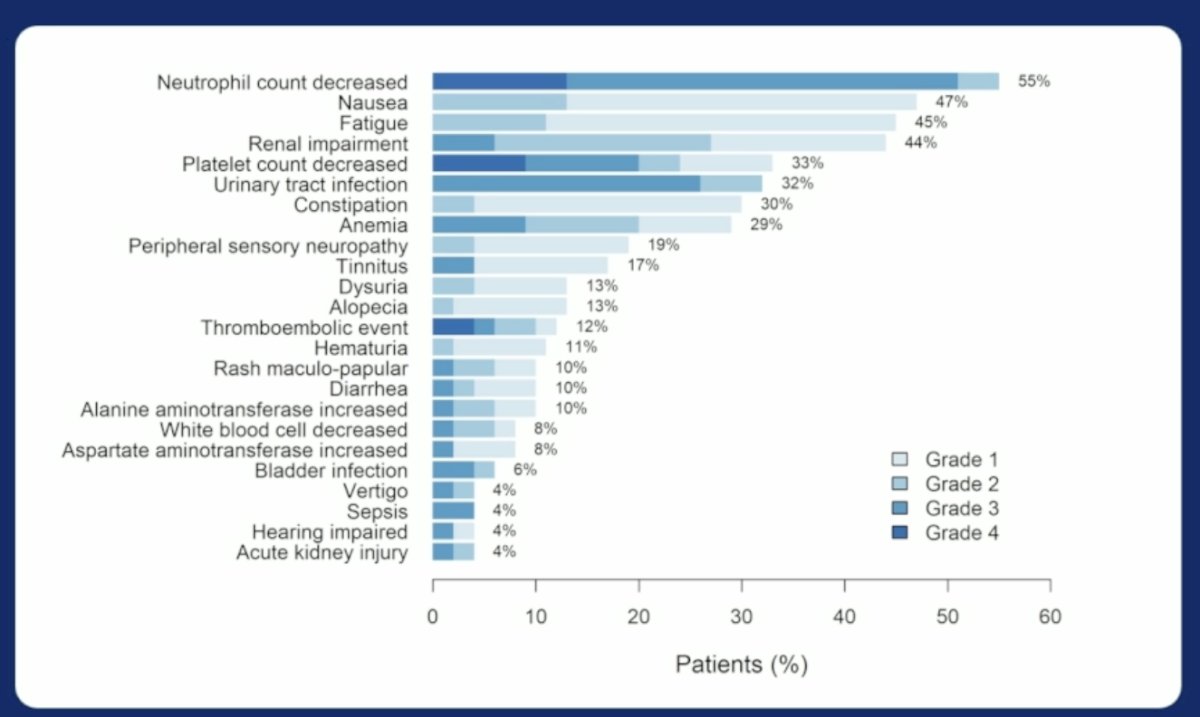
A pre-planned comparison was performed against SAKK 06/17 using propensity score weighted analysis. SAKK 06/19 evaluated cisplatin/gemcitabine/atezolizumab plus three intravesical rBCG instillations, whereas SAKK 06/17 evaluated cisplatin/gemcitabine/durvalumab without rBCG.
Compared to SAKK 06/17, pCR rates increased from 32% to 67% with the addition of rBCG. In multivariable propensity score weighted analysis, the odds ratio for pCR was 5.13 (95% CI 2.63–10.02; p<0.001).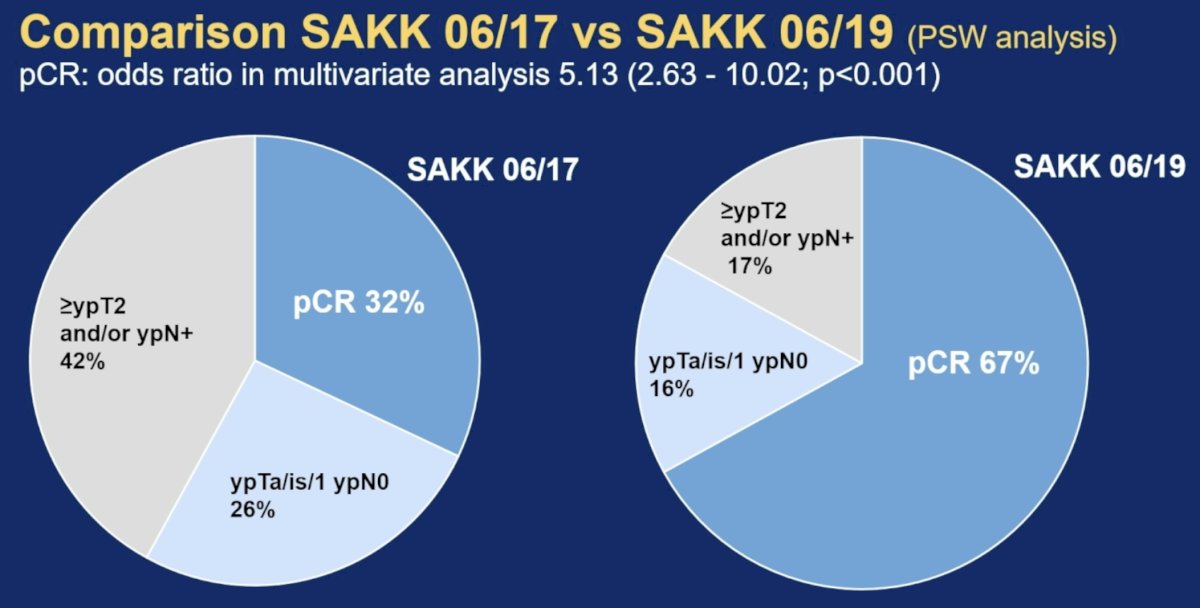
The investigators acknowledged several limitations:
- Non-randomized design
- Small sample size
- Short follow-up at the time of this primary analysis
- Potential selection bias associated with a complex interdisciplinary regimen
- 15% non-surgery rate introducing potential selection bias
- The comparison with SAKK 06/17 being limited by the use of different checkpoint inhibitors (durvalumab versus atezolizumab), as well as potential unmeasured confounders.
Dr. Cathomas concluded as follows:
- Intravesical rBCG in combination with cisplatin + gemcitabine + atezolizumab achieves promising efficacy with high pCR and partial responses
- The combination of rBCG plus chemo-immunotherapy was feasible and tolerable
- The pre-planned comparison to SAKK 06/17 supports a potential impact for rBCG.
- Future investigation of intravesical rBCG in combination with next-generation systemic regimens in randomized trials is warranted.
The key takeaway points from SAKK 06/19 were as follows:
- The addition of intravesical recombinant BCG (rBCG) to chemo-immunotherapy in MIBC is feasible, tolerable, and has promising efficacy with a high pathological complete response rate.
- Further investigation of intravesical rBCG in combination with next-generation systemic regimens in randomized trials is warranted.
Presented by: Richard Cathomas, MD, Head, Division of Oncology/Haematology, Kantonsspital Graubünden, Chur, Switzerland
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the ASCO 2026 Annual Meeting, Chicago, IL, May 29th–June 2nd, 2026
References:- Cathomas R, Rothschild SI, Hayoz S, et al. Perioperative Chemoimmunotherapy With Durvalumab for Muscle-Invasive Urothelial Carcinoma: Primary Analysis of the Single-Arm Phase II Trial SAKK 06/17. J Clin Oncol. 2023;41:5131-5139. doi:10.1200/JCO.23.00363.
- Powles T, Catto JWF, Galsky MD, et al. Perioperative Durvalumab With Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024;391:1773-1786. doi:10.1056/NEJMoa2408154.
- Rentsch CA, Thalmann GN, Lucca I, et al. A Phase 1/2 Single-Arm Clinical Trial of Recombinant Bacillus Calmette-Guérin (BCG) VPM1002BC Immunotherapy in Non-Muscle-Invasive Bladder Cancer Recurrence After Conventional BCG Therapy: SAKK 06/14. Eur Urol Oncol. 2022;5(2):195-202. doi:10.1016/j.euo.2021.12.006.