(UroToday.com) The 2025 ASCO annual meeting featured a penile cancer rapid oral abstract session and a presentation by Dr. Aditya Dhanawat discussing an open label randomized non-inferiority trial comparing adjuvant platinum + paclitaxel to platinum + 5-FU after curative resection in high-risk penile carcinoma. Globally, penile cancer is rare, with an age adjusted standardized incidence rate of 0.79 per 100,000, which is much lower compared to 1.6 per 100,000 in India. Previous studies have suggested that patients with >1 inguinal lymph node, those with bulky lymph nodes, pelvic lymph nodes, or peri-nodal extension, confers a poor prognosis. To date, there is no randomized evidence to guide neoadjuvant/adjuvant chemotherapy in penile cancer, thus, there is a clear evidence gap. The aim of this trial was to compare the safety and efficacy of adjuvant platinum + 5-FU versus platinum + paclitaxel chemotherapy in high risk penile cancer.
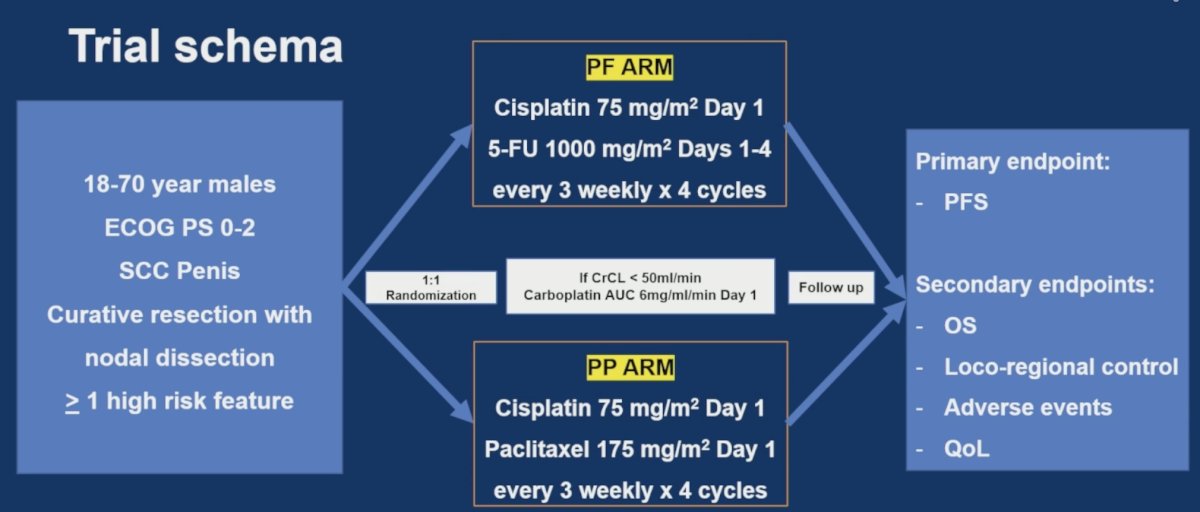
This was a prospective, open-label, phase 3, randomized controlled trial at Tata Memorial Centre in Mumbai, India, from March 2017 to October 2024. Patients with high-risk penile cancer (> 1 inguinal lymph node, perinodal extension, pelvic lymph node, or lymph node > 4 cm) who underwent curative resection were randomized 1:1 to receive 4 cycles of platinum + 5-FU or platinum + paclitaxel, followed by concurrent chemoradiotherapy (50 Gy/25# followed by boost 5-10 Gy in the regions of perinodal extension). The primary endpoint was progression free survival, and secondary endpoints were overall survival, toxicities, and quality of life. The trial schema is as follows:
Exclusion criteria for the trial are as follows:
- R2 resection of the groin or pelvic lymph nodes
- Unhealthy wound/significant local infection/discharging mass
- Prior invasive malignancy in remission < 3 years
- Peripheral neuropathy > grade 2
- History of severe hypersensitivity to paclitaxel, carboplatin or cisplatin and 5-FU
- Uncontrolled co-morbidities
- Distant metastatic disease
- Life expectancy < 6 months
From a sample size calculation standpoint, the investigators assumed a median progression free survival of platinum + paclitaxel of 8 months, assuming a non-inferiority margin of 1 month in the median progression free survival for the paclitaxel arm compared to the 5-FU arm. This provided 90% power (95% one-sided CI), assuming 10% attrition per year, for an estimated sample size of 150 patients. Recruitment began in March 2017 but closed prematurely due to slow accrual. The following highlights the patient enrollment, allocation, and follow-up for the trial:
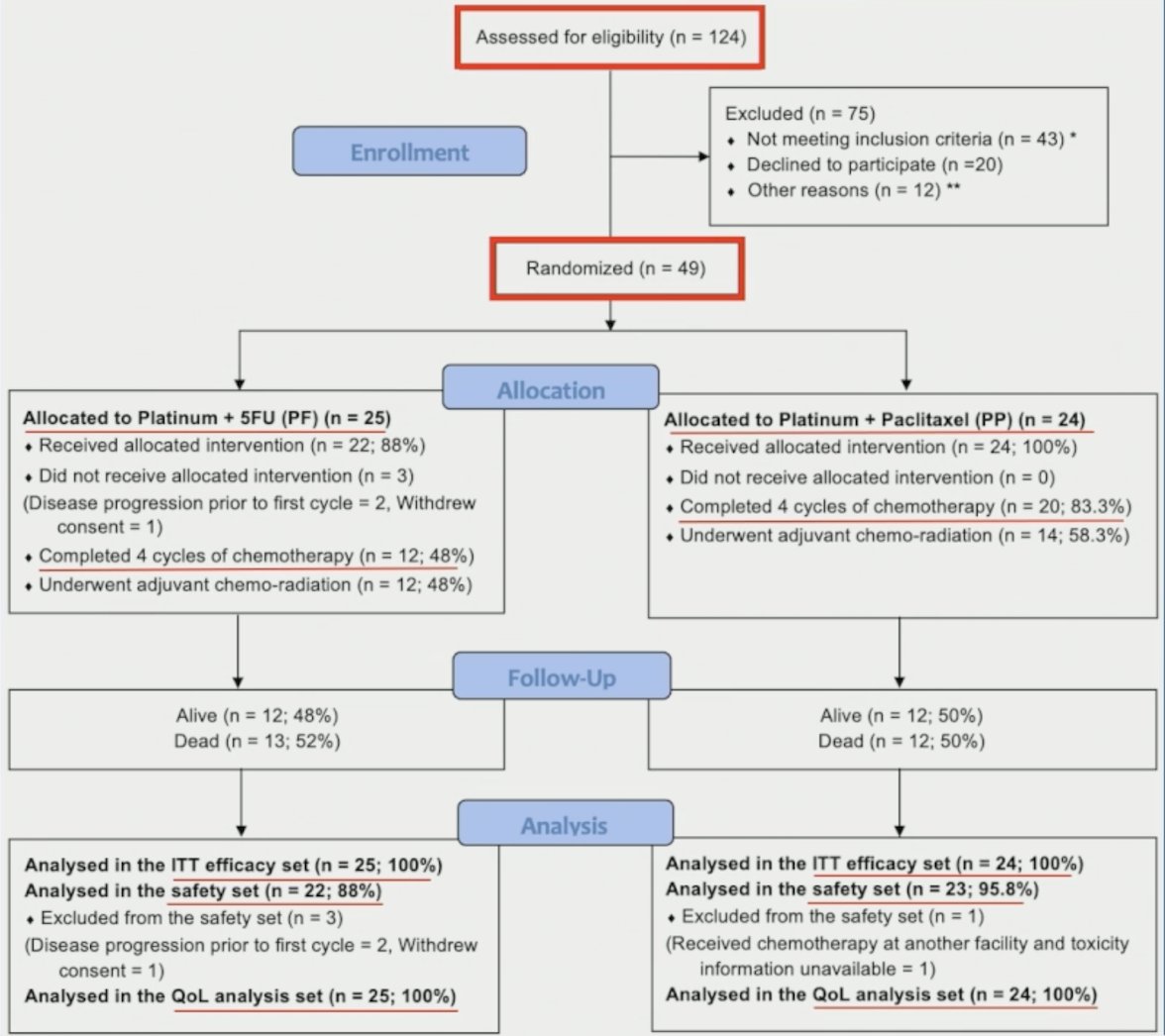
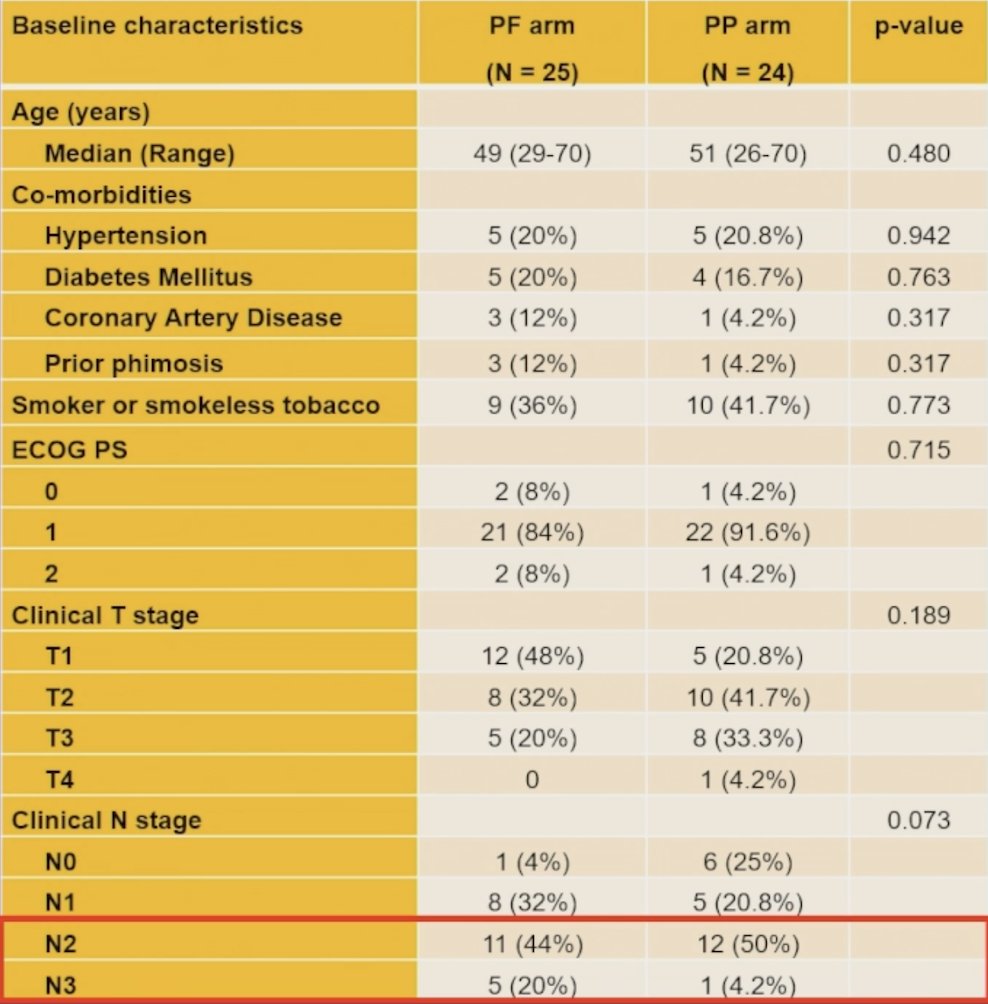
Between March 2017 and October 2024, 49 patients were randomized, including 25 to the platinum + 5-FU arm and 24 to the platinum + paclitaxel arm. The baseline demographics are highlighted in the following table:
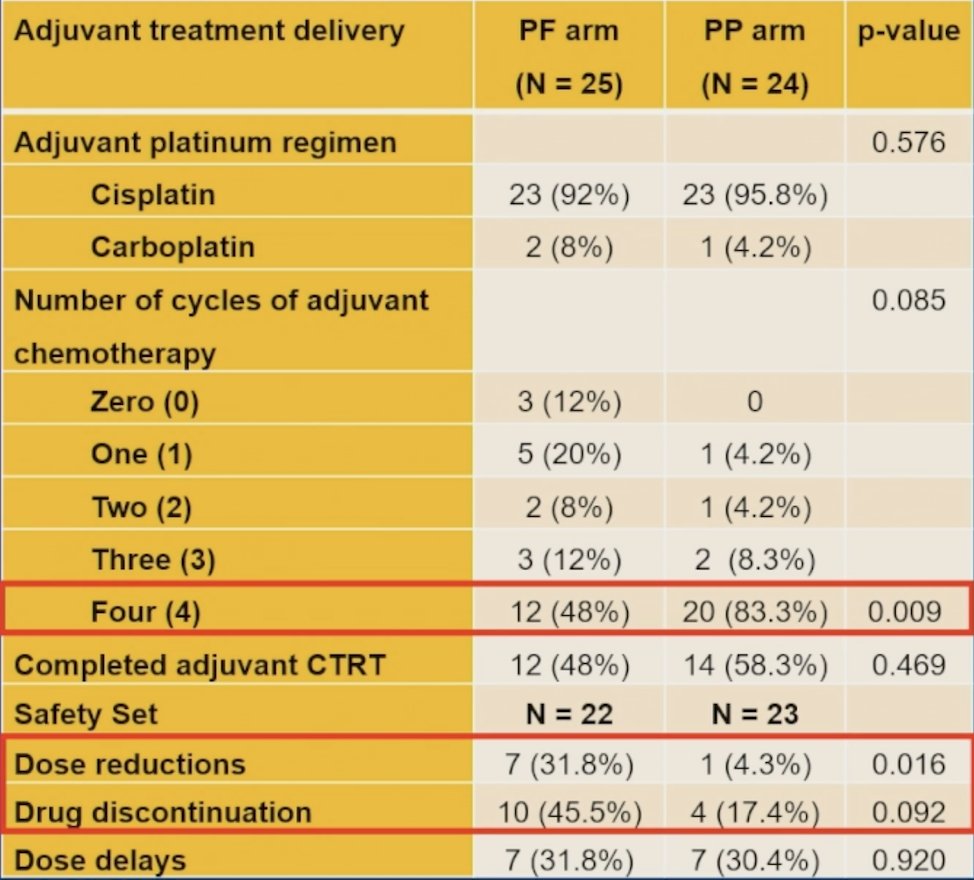
The median follow-up was 60.1 months. Dose reductions were higher (31.8% versus 4.3%, p = 0.016), there were similar dose delays (31.8% versus 30.4%, p = 0.920), and a non-significant increase in drug discontinuation (45.5% versus 18.4%, p = 0.092) in the platinum + 5-FU arm:
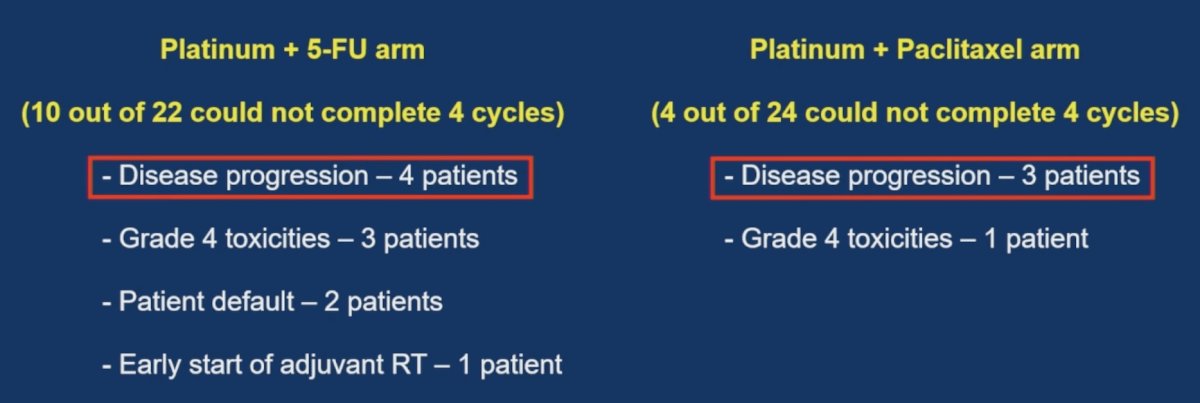
Reasons for discontinuation by arm are listed as follows:
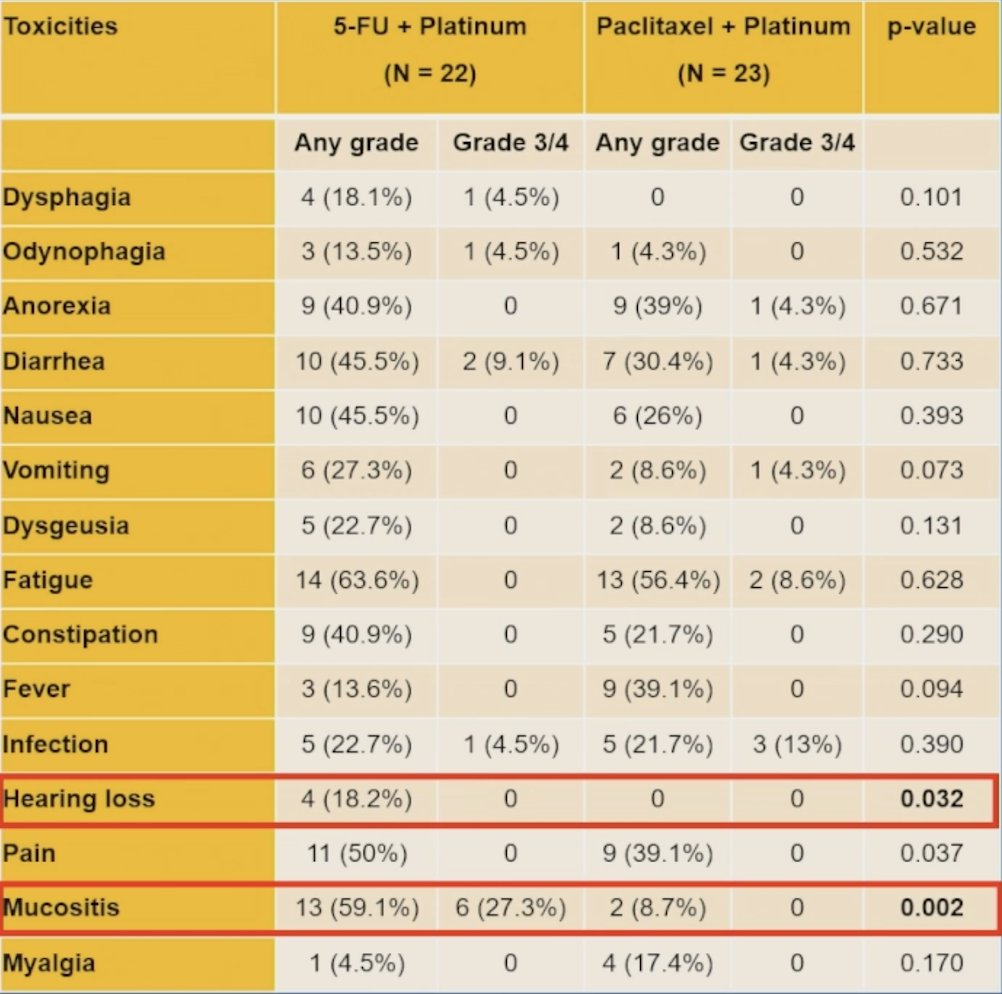
Grade 3/4 hematological (31.8% versus 13.0%, p = 0.130) and gastrointestinal (31.8% versus 4.3%, p = 0.016) toxicities were higher in platinum + 5-FU arm, but there was no overall difference in grade 3/4 toxicities (54.5% versus 39.1%, p = 0.30). Specific any grade toxicities that were higher in the platinum + 5-FU arm included hearing loss (18.2% versus 0%; p = 0.0320) and mucositis (59.1% versus 8.7%; p = 0.002):
There was no significant difference in median progression free survival (12.5 versus 35.9 months, p=0.46), 5-year progression free survival (36.1% versus 38.5%), median overall survival (21.6 versus 37.2 months, p = 0.53), and 5-year overall survival (45.3% versus 41.1%) between the platinum + 5-FU and platinum + paclitaxel arm, respectively. Distant metastases occurred in 28% of patients treated with platinum + 5-FU compared to 33% of patients treated with platinum + paclitaxel, with the most common sites being the lung (18.4%), skin (6.1%), and bones (6.1%). Subsequent treatment included palliative chemotherapy in 28.6% of patients and best supportive care in 18.4%. Quality of life (EORTC QLQ-C30 and MSHQ) analysis showed no difference in global health status, functional, and symptom scales. Additionally, all MSHQ domains were similar between the two groups.
A strength of the current trial is that it is the first randomized data to assess adjuvant treatment of high risk penile cancer patients. Limitations include (i) the open label design potentially introducing bias, however, blinding was not feasible given that 5-FU administration requires central venous access, (ii) the small sample size led to under-powered results, and (iii) longer follow-up data is needed to assess late toxicities and long-term survival outcomes.
Dr. Dhanawat concluded his presentation discussing an open label randomized non-inferiority trial comparing adjuvant platinum + paclitaxel to platinum + 5-FU after curative resection in high-risk penile carcinoma with the following take home points:
- There was a numerically higher median progression free survival and median overall survival with paclitaxel versus 5-FU, but there was no statistical significance
- There was increased gastrointestinal and hematological toxicities with 5-FU
- There was increased neuropathy and liver dysfunction with paclitaxel
- Quality of life results showed similar EORTC QLQ C-30 and MSHQ domains
Presented by: Aditya Dhanawat, MBBS, MD, DM, Tata Memorial Centre, Mumbai, India
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.