(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30 and June 3 was host to the Session State of the Art Lecture: Personalizing treatment for patients with metastatic castration resistant prostate cancer (mCRPC) in 2025. Dr. Ruben Raychaudhuri delivered a presentation discussing How to Get Lutetium-177 PSMA to Those That Will Most Benefit?
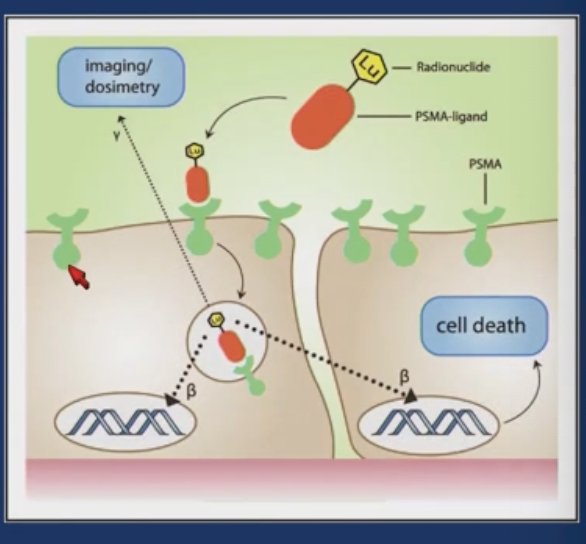
Lutetium-177–PSMA-617 is a targeted radioligand therapy directed against prostate-specific membrane antigen (PSMA), a surface protein expressed on most prostate cancer cells and, to a lesser extent, some benign tissues contributing to the treatment’s toxicity profile. Lu-177 PSMA-617 delivers beta radiation specifically to PSMA-expressing cells, enabling targeted cytotoxicity. PSMA PET imaging is used to assess antigen expression and determine patient eligibility for therapy, allowing for more personalized treatment selection.
The VISION trial was a Phase III randomized study evaluating Lu-177–PSMA-617 (LuPSMA) versus standard-of-care (SOC) therapy in patients with metastatic castration-resistant prostate cancer (mCRPC) who had previously received both an androgen receptor pathway inhibitor and at least one taxane-based chemotherapy regimen. All patients were required to have PSMA-positive disease on Ga-68 PSMA-11 PET imaging and an ECOG performance status of 0–2. Patients were randomized 2:1 to receive protocol-permitted SOC with or without LuPSMA. The primary endpoints were overall survival (OS) and radiographic progression-free survival (rPFS).1
The trial demonstrated significant OS and rPFS benefits for LuPSMA compared to SOC alone. The control arm was limited and experienced a high rate of dropout. Despite this, the OS benefit was clearly observed, confirming LuPSMA as a highly effective therapy in this heavily pretreated population. These findings led to FDA approval of LuPSMA in the post-chemotherapy setting in March 2022.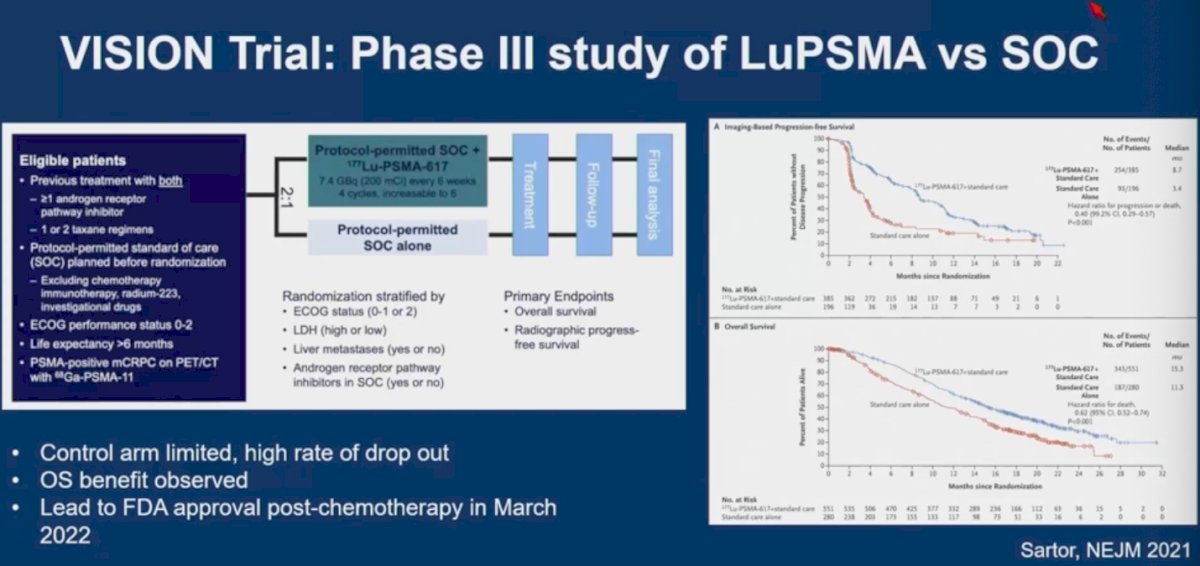
The TheraP trial was a Phase II Australian study comparing LuPSMA to cabazitaxel in patients with mCRPC previously treated with docetaxel. All patients had PSMA-positive disease confirmed by PSMA and FDG PET/CT. Eligible patients were randomized 1:1 to LuPSMA or cabazitaxel, with treatment stratified by disease burden and prior ARPI use. The trial showed improved PSA response and evidence of overall survival benefit with LuPSMA, supporting its use in this setting.2
Notably, the TheraP trial was not powered to detect an overall survival (OS) difference, and no OS benefit was observed. However, the objective response rate (ORR) favored LuPSMA at 49%, compared to 24% with cabazitaxel.
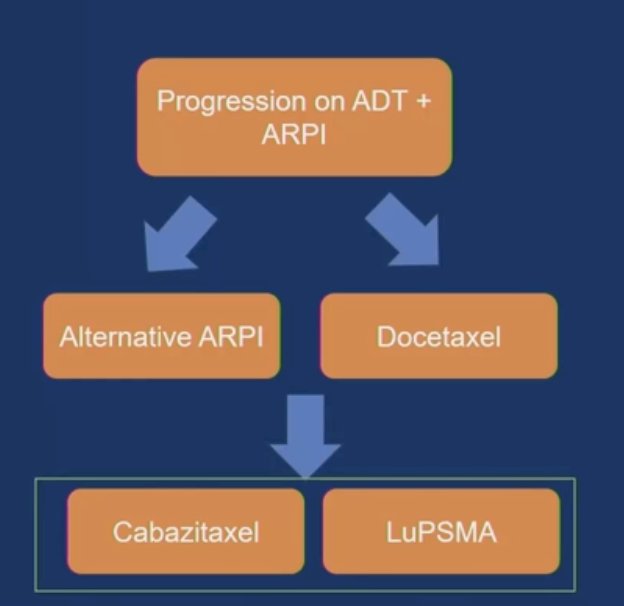
Dr. Raychaudhuri presented a simplified treatment algorithm in 2024 to help guide decision-making in the post-taxane setting for metastatic prostate cancer. A key consideration in this space is toxicity profile, as many patients prefer to delay or avoid further chemotherapy if feasible. Biomarkers and imaging eligibility play a critical role in treatment selection specifically, whether patients meet criteria similar to those used in the VISION and TheraP trials. These include PSMA PET positivity and, in the case of TheraP, exclusion of discordant FDG-positive/PSMA-negative disease.1,2
Targeted radioligand therapies like LuPSMA require specific imaging-based eligibility criteria. As shown in the comparison table, the VISION trial relied solely on PSMA PET imaging, while TheraP used both PSMA and FDG PET to screen patients more stringently. In VISION, patients were eligible if they had at least one lesion with PSMA uptake greater than liver, and were excluded if they had any lesion that met CT size criteria but had lower PSMA uptake than liver. In contrast, TheraP required at least one lesion with a SUVmax ≥20 and excluded patients with discordant lesions FDG-positive but PSMA-negative or any lesion with SUVmax <10.
As a result of these stricter thresholds, 27.4% of screened patients failed imaging eligibility in TheraP, compared to only 12.6% in VISION. PSA₅₀ response was also higher in TheraP (66% vs 46%), likely reflecting more selective inclusion criteria and tumor biology.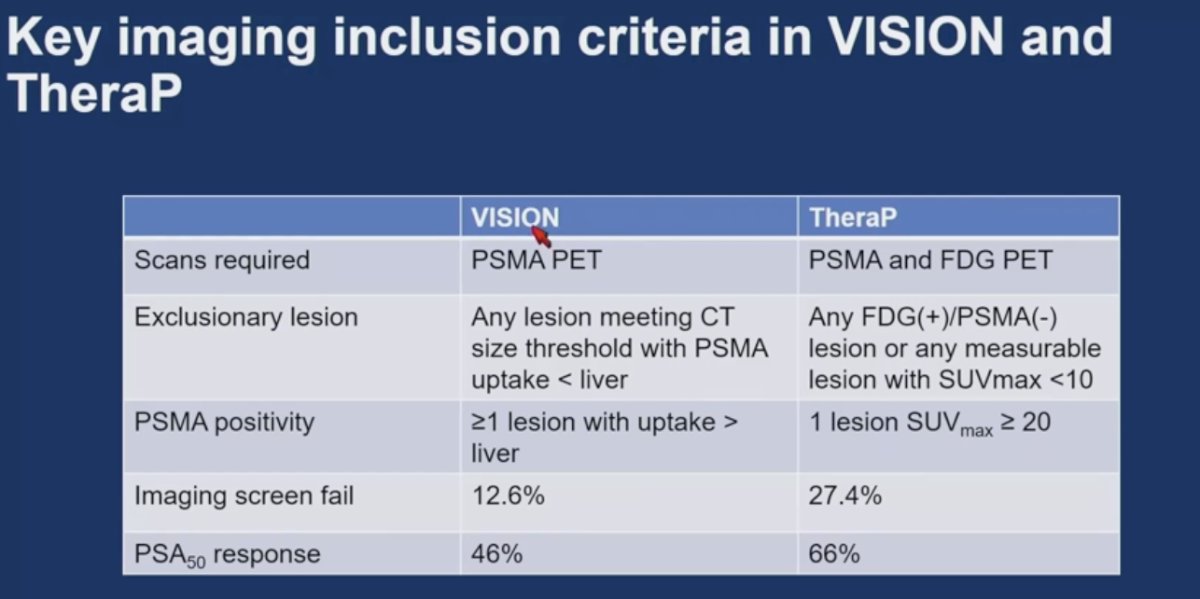
A multicenter retrospective cohort study evaluated outcomes in 301 patients treated with standard-of-care LuPSMA, including those who would not have met VISION trial eligibility. Among VISION-ineligible patients, the PSA₅₀ response rate was only 21%, compared to 50% in the VISION-eligible cohort. Notably, this analysis did not include the 10–15% of patients pre-excluded from treatment based on imaging criteria. Overall, VISION-ineligible patients experienced significantly poorer outcomes with LuPSMA, underscoring the importance of appropriate patient selection.3
Biomarkers of response in the VISION Trial include higher PSMA expression associated with increased radioligand uptake and may correlate with improved treatment response to LuPSMA. Among patients eligible for therapy in the VISION trial, a wide range of whole-body PSMA mean standardized uptake values (SUVmean) was observed. A secondary analysis revealed that patients in the highest SUVmean quartile experienced the best progression-free survival (PFS) and OS. Notably, each 1-unit increase in SUVmean was associated with a 12% reduction in risk of a PFS event and a 10% reduction in risk of death.
In the TheraP trial, higher PSMA SUVmean was associated with improved outcomes following LuPSMA treatment. Patients with a SUVmean ≥10 had a PSA₅₀ response rate of 91%, compared to 52% in those with SUVmean <10. Additionally, high FDG tumor volume was prognostic for worse outcomes across both treatment arms LuPSMA and cabazitaxel highlighting the value of dual-tracer imaging in predicting response and prognosis.4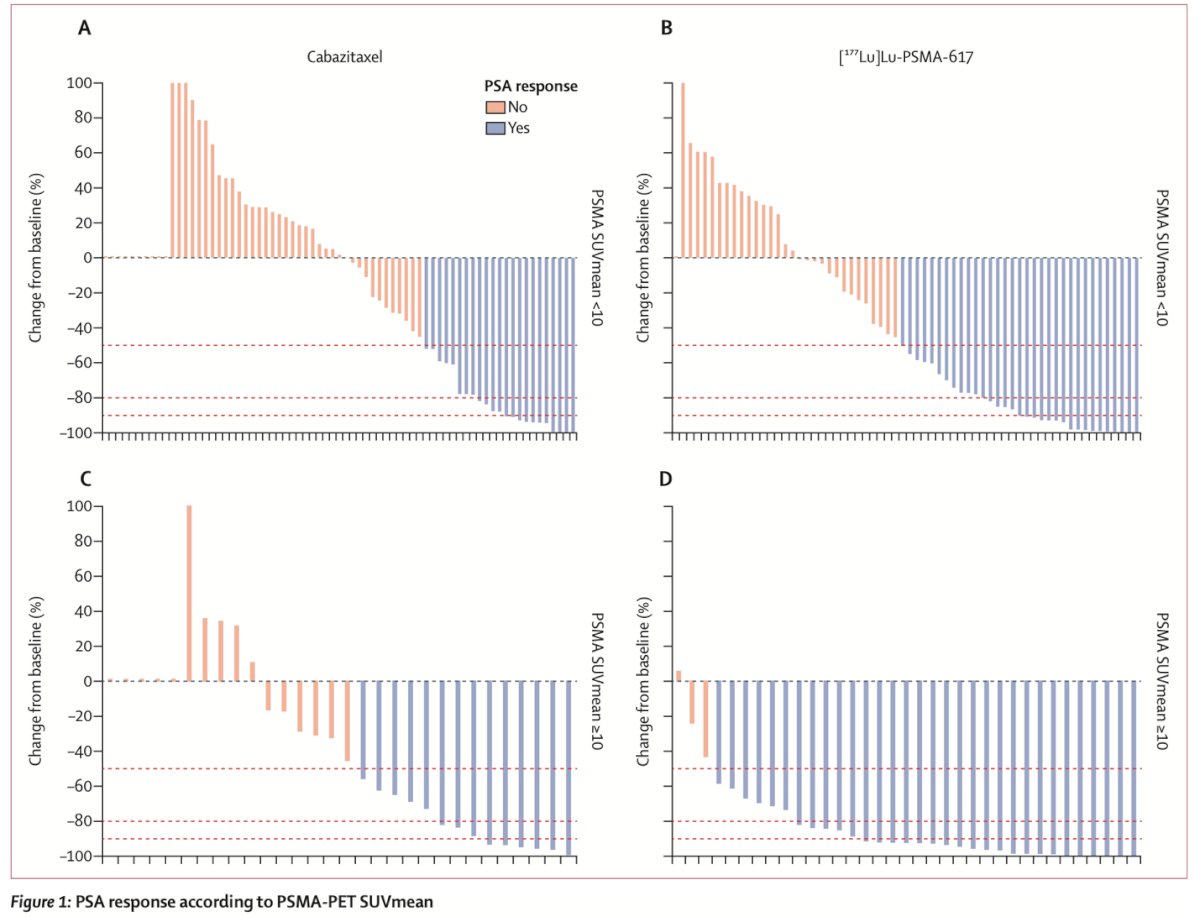
Dr. Raychaudhuri addressed the question of whether PSMA SUVmean is predictive or prognostic. Data suggest that patients with low PSMA expression have inferior survival outcomes regardless of treatment choice. However, she cautioned against using a low SUVmean as justification for defaulting to chemotherapy in patients who otherwise meet VISION eligibility criteria. Instead, this subgroup likely represents a population in need of alternative or more effective therapies.
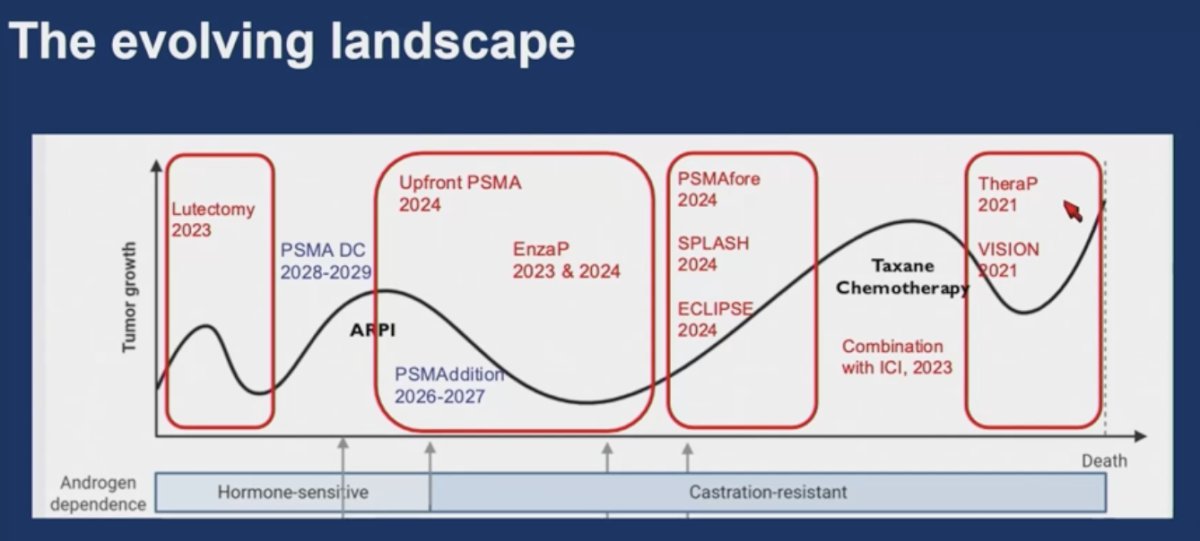
Earlier use of LuPSMA may have advantages, as PSMA expression can be affected by prior therapies such as AR pathway inhibitors, cytotoxic chemotherapy, and the emergence of neuroendocrine prostate cancer (NEPC) often PSMA-negative under therapeutic pressure. Administering LuPSMA earlier in the disease course may allow for more effective dosing with potentially reduced toxicity, particularly before cumulative bone marrow compromise occurs. Tumor volume and the radioligand’s cross-fire effect may also influence outcomes. Additionally, the emergence of clonal hematopoiesis in some patients receiving LuPSMA highlights the need to re-examine its long-term safety profile. The evolving landscape of LuPSMA therapy is outlined below.
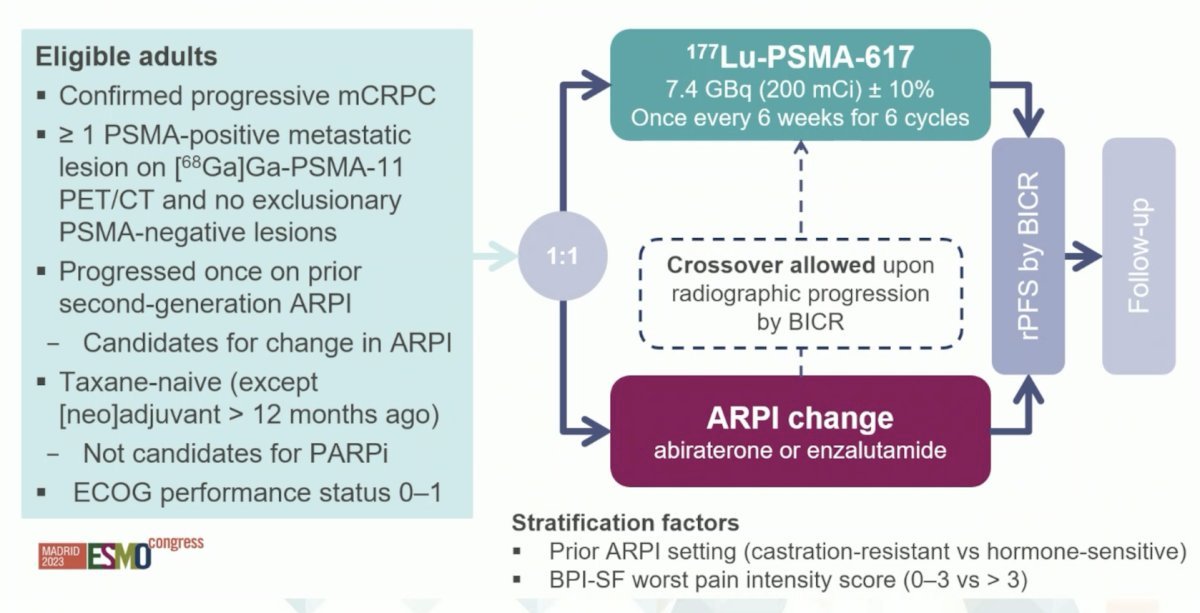
PSMAfore is a Phase III trial evaluating the use of LuPSMA in an earlier treatment setting for mCRPC. Eligible patients had progressive disease after one prior second-generation ARPI (abiraterone or enzalutamide), were taxane-naïve, and ineligible for PARP inhibitors. All patients had PSMA-positive lesions on ⁶⁸Ga-PSMA-11 PET/CT with no exclusionary PSMA-negative sites.
Patients were randomized 1:1 to receive either LuPSMA or an ARPI switch (to abiraterone or enzalutamide). Crossover to LuPSMA was permitted upon radiographic progression. The trial population represented a lower-risk group: 71% were asymptomatic or mildly symptomatic, and only 4% had liver metastases. The primary endpoint was rPFS by blinded independent central review.5
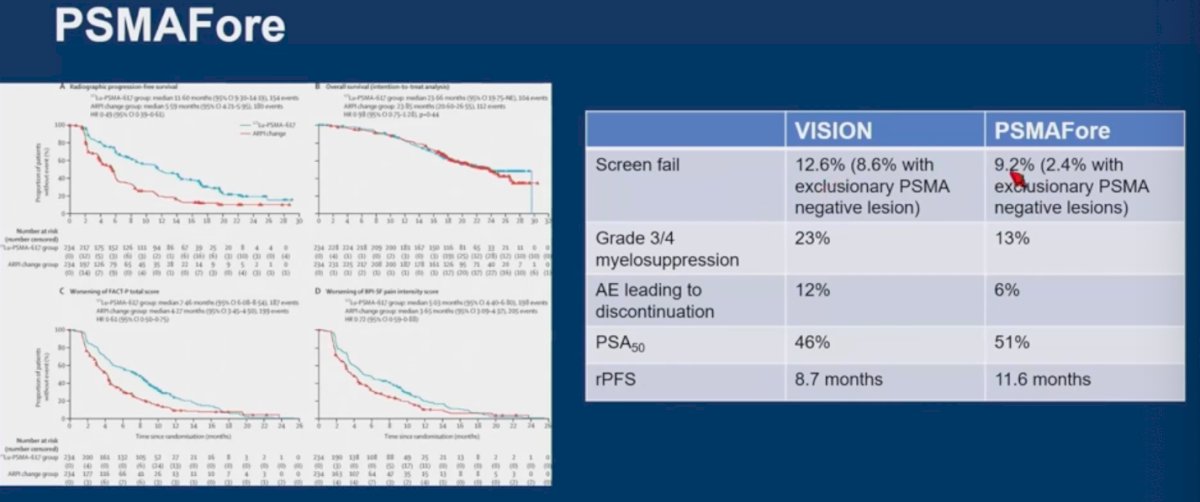
The PSMAfore trial did not meet its primary endpoint, which may be partially attributed to the high crossover rate 134 patients (57%) in the control arm ultimately received LuPSMA after progressing on ARPI. Notably, earlier-line recruitment appears more feasible, as screening failure rates were slightly lower compared to VISION (12.6% vs 9.2%), suggesting broader eligibility when treating patients earlier in the disease course.
On March 28, 2025, the U.S. Food and Drug Administration (FDA) expanded the indication for lutetium Lu 177 vipivotide tetraxetan to include adults with PSMA-positive metastatic castration-resistant prostate cancer (mCRPC) who have received prior ARPI therapy and are deemed appropriate candidates to delay taxane-based chemotherapy.
Dr. Raychaudhuri presented a simplified treatment algorithm in 2025 to guide decision-making in the pre-taxane setting for mCRPC. However, several important questions remain unresolved, including how best to choose therapy in the absence of head-to-head comparisons. The CCTG PR21 study a Canadian study, which has completed accrual, may help inform future guidance. Additional considerations include treatment-related toxicity profiles, imaging biomarkers, and the role of tumor mutational profiling in guiding patient selection.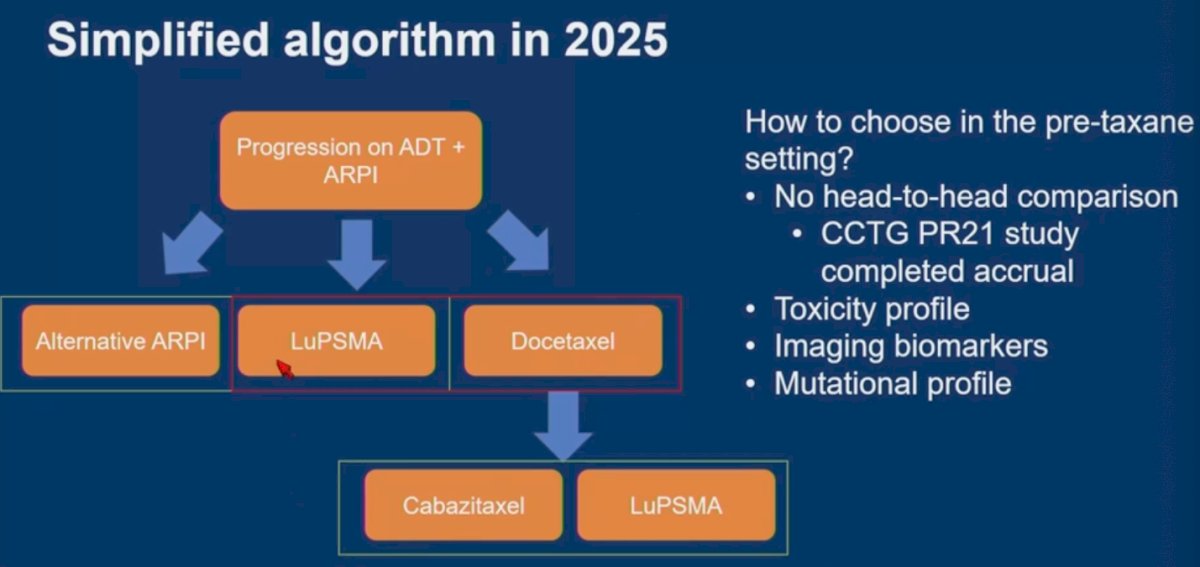
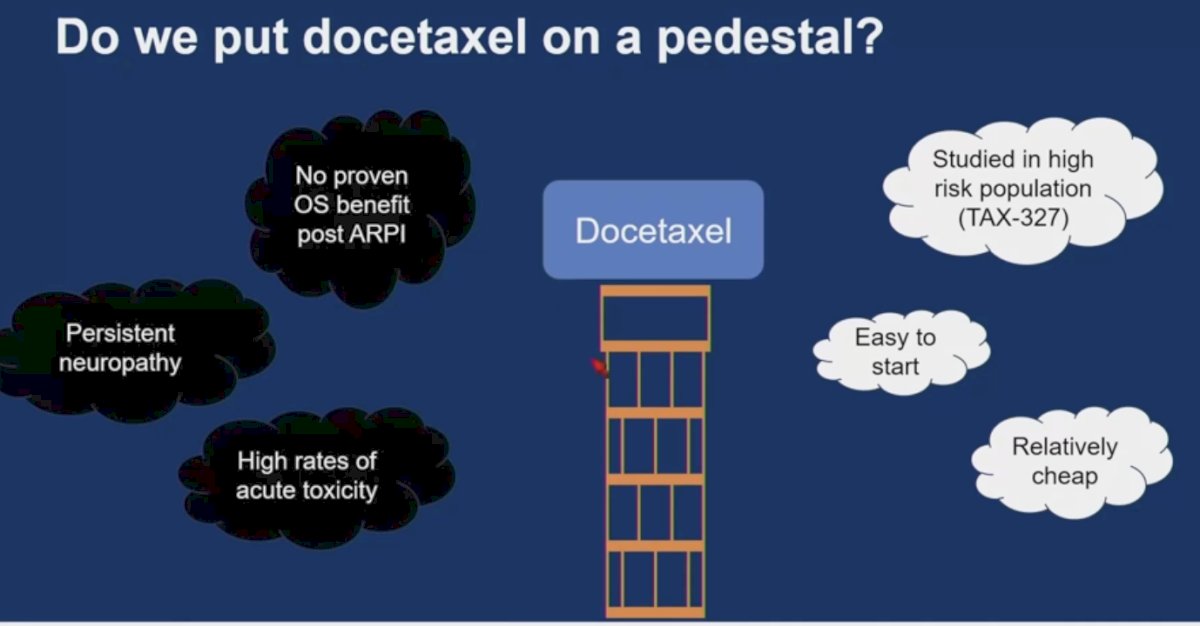
There is currently no clear OS benefit for docetaxel following ARPI therapy in mCRPC, and its use is associated with high rates of acute toxicity. Much of the available data comes from studies conducted in high-risk populations. As such, we should be cautious about overvaluing its role in treatment sequencing without stronger comparative evidence.
Access to PSMA-targeted radioligand therapy remains limited due to several logistical and systemic challenges. Delivery is complex, requiring coordination across multidisciplinary teams and administration in large tertiary centers. As a result, geographic barriers significantly limit access for patients in rural or underserved areas. Long wait times for both PSMA PET imaging and treatment further complicate timely care. Building partnerships between smaller community sites and high-volume centers is essential to expanding access. In addition, socioeconomic barriers must be addressed to ensure equitable delivery of this advanced therapy.
Ongoing research is focused on optimizing the therapeutic impact of LuPSMA through more flexible dosing strategies, modulation of PSMA expression, and rational combination approaches. These include combining LuPSMA with chemotherapy, PARP inhibitors, ARPIs, and other agents. Dr. Raychaudhuri presented a compelling case of a patient who received more than 20 cycles of LuPSMA and remained progression-free for several years, highlighting the potential of extended treatment duration and combinatorial strategies in select patients.
Dr. Raychaudhuri concluded with the following key takeaways:
- Lutetium-177 PSMA is a safe and effective therapy in patients with mCRPC who meet PSMA PET imaging criteria, both before and after taxane chemotherapy.
- The optimal sequencing of LuPSMA within the treatment landscape remains undefined and continues to evolve as new data emerge.
Presented by: Ruben Raychaudhuri, MD, University of Washington and Fred Hutchinson Cancer Center, Seattle, WA.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:
- Sartor O, de Bono J, Chi KN, Fizazi K, Herrmann K, Rahbar K, et al. Lutetium-177–PSMA-617 for metastatic castration-resistant prostate cancer. N Engl J Med. 2021;385(12):1091–1103.
- Hofman MS, Emmett L, Sandhu S, Iravani A, Joshua AM, Goh JC, et al. [177Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): a randomised, open-label, phase 2 trial. Lancet. 2021;397(10276):797–804.
- Hotta M, Gafita A, Czernin J, Calais J. Outcome of Patients with PSMA PET/CT Screen Failure by VISION Criteria and Treated with 177Lu-PSMA Therapy: A Multicenter Retrospective Analysis. J Nucl Med. 2022 Oct;63(10):1484-1488. doi: 10.2967/jnumed.121.263441. Epub 2022 Mar 10. PMID: 35273096.
- Buteau JP, Martin AJ, Emmett L, Iravani A, Sandhu S, Joshua AM, Francis RJ, Zhang AY, Scott AM, Lee ST, Azad AA, McJannett MM, Stockler MR, Williams SG, Davis ID, Hofman MS; TheraP Trial Investigators and the Australian and New Zealand Urogenital and Prostate Cancer Trials Group. PSMA and FDG-PET as predictive and prognostic biomarkers in patients given [177Lu]Lu-PSMA-617 versus cabazitaxel for metastatic castration-resistant prostate cancer (TheraP): a biomarker analysis from a randomised, open-label, phase 2 trial. Lancet Oncol. 2022 Nov;23(11):1389-1397. doi: 10.1016/S1470-2045(22)00605-2. Epub 2022 Oct 16. PMID: 36261050.
- Morris MJ, Castellano D, Herrmann K, de Bono JS, Shore ND, Chi KN, Crosby M, Piulats JM, Fléchon A, Wei XX, Mahammedi H, Roubaud G, Študentová H, Nagarajah J, Mellado B, Montesa-Pino Á, Kpamegan E, Ghebremariam S, Kreisl TN, Wilke C, Lehnhoff K, Sartor O, Fizazi K; PSMAfore Investigators. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naive patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): a phase 3, randomised, controlled trial. Lancet. 2024 Sep 28;404(10459):1227-1239. doi: 10.1016/S0140-6736(24)01653-2. Epub 2024 Sep 15. Erratum in: Lancet. 2025 Dec 21;404(10471):2542. doi: 10.1016/S0140-6736(24)02716-8. PMID: 39293462; PMCID: PMC12121614.