(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30 and June 3 was host to the Oral Abstract Session: Genitourinary Cancer—Prostate, Testicular, and Penile. Dr. Rahul Raj Aggarwal delivered a presentation titled: Tailoring Therapy in Castration-Sensitive Prostate Cancer: Do Biomarkers Make the Cut?
Dr. Aggarwal began his presentation by highlighting how the treatment landscape for metastatic castration-sensitive prostate cancer (mCSPC) has evolved. Historically, patients were managed uniformly with androgen deprivation therapy (ADT), with or without first-generation antiandrogens. However, contemporary strategies now tailor treatment based on disease volume and timing of metastasis. Current clinical practice differentiates between synchronous low-volume, metachronous low-volume, and high-volume disease. For synchronous low-volume disease, ADT is combined with an androgen receptor pathway inhibitor (ARPI) and potentially local treatment. Patients with metachronous low-volume disease typically receive ADT plus ARPI, while those with high-volume disease are treated with ADT, ARPI, and possibly docetaxel.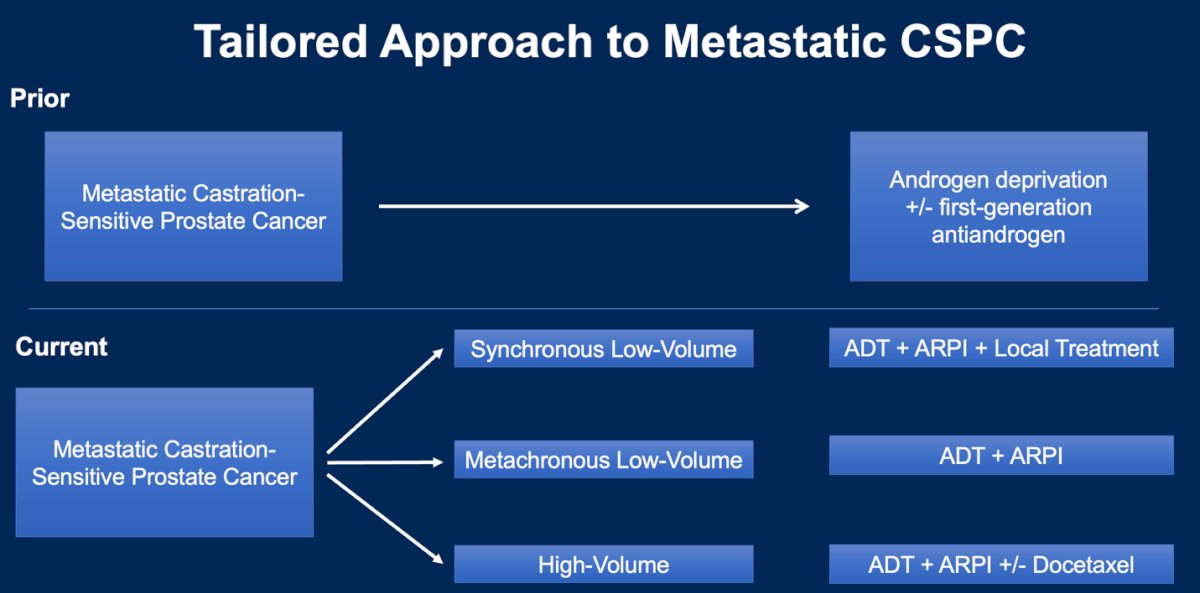
Multiple ARPIs including abiraterone, apalutamide, and enzalutamide have been shown to significantly improve overall survival in patients with mCSPC. Each agent reduced the risk of death compared to placebo: 34% with abiraterone, 35% with apalutamide, and 30% with enzalutamide.1-3
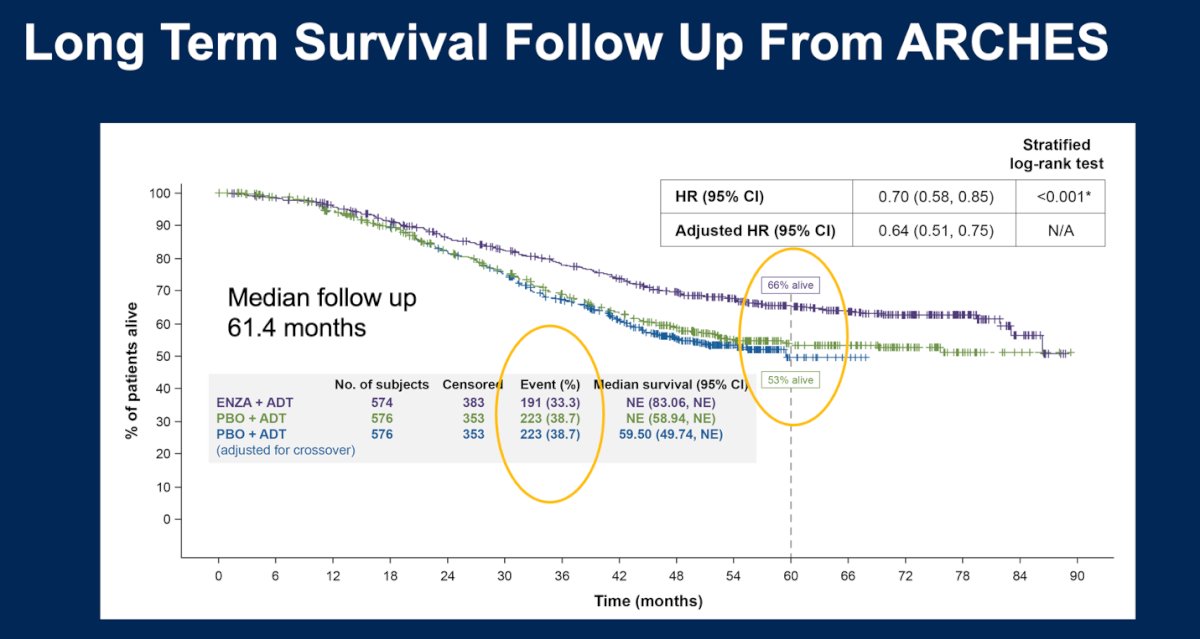
Notably, the ARCHES trial had the longest median follow-up among ARPI trials at 61.4 months. During this period, median overall survival was not reached in either treatment arm. At 5 years, 66% (two thirds) of patients receiving enzalutamide plus ADT were alive, compared to 53% in the placebo plus ADT arm.2
Dr. Aggarwal noted the potential to incorporate additional clinical and genomic biomarkers to further refine treatment selection and optimize outcomes in mCSPC. These include PSA nadir, patient-reported quality of life and treatment-related toxicity, PTEN inactivation, homologous recombination repair (HRR) alterations, and advanced molecular imaging. The following three abstracts presented at this session were critically appraised by Dr. Aggarwal:
- PSA as a prognostic marker:
Dr. Michael Ong (Abstract #5002) presented real-world data from the IRONMAN registry showing that a PSA >0.2 ng/mL at 6–12 months after ARPI-intensified therapy in mHSPC is associated with worse outcomes, supporting its role as a simple early prognostic marker. - Quality of life with treatment intensification:
Dr. Alicia Morgans (Abstract #5004) reported findings from the phase 3 ARANOTE trial indicating that darolutamide preserves health-related quality of life (HRQoL) in patients receiving intensified treatment. - PTEN inactivation and docetaxel benefit:
Dr. Emily Grist (Abstract #5003) presented data from a STAMPEDE ancillary study suggesting that patients with transcriptomic PTEN inactivation may derive greater survival benefit from adding docetaxel to ADT at treatment initiation. - HRR Alterations
- Molecular Imaging
A PSA nadir between 6–12 months of treatment has consistently emerged as a strong prognostic biomarker for both progression-free survival (PFS) and overall survival (OS) in mCSPC Multiple trials including SWOG 9346, CHAARTED, LATITUDE, TITAN, ARCHES, ENZAMET, ARANOTE, and real-world cohorts demonstrate that a PSA response of <0.2 ng/mL, ≤0.02 ng/mL, or ≤0.1 ng/mL within the 6- to 12-month window is associated with significantly improved long-term outcomes.4-7 Notably, in the IRONMAN an impressive global registry, PSA ≤ 0.2 at 6 and 12 months was linked to better prognosis, reinforcing this as a clinically meaningful target.
The IRONMAN registry data highlights real-world treatment patterns in patients with mHSPC, showing that only 65% of patients received appropriate treatment intensification with ADT + ARPI. Among the 2,713 eligible patients, 1,274 had documented use of ADT + ARPI. This gap reflects a lack of adherence to guideline-recommended treatment intensification in approximately one-third of patients globally, with wide geographic variability in uptake.8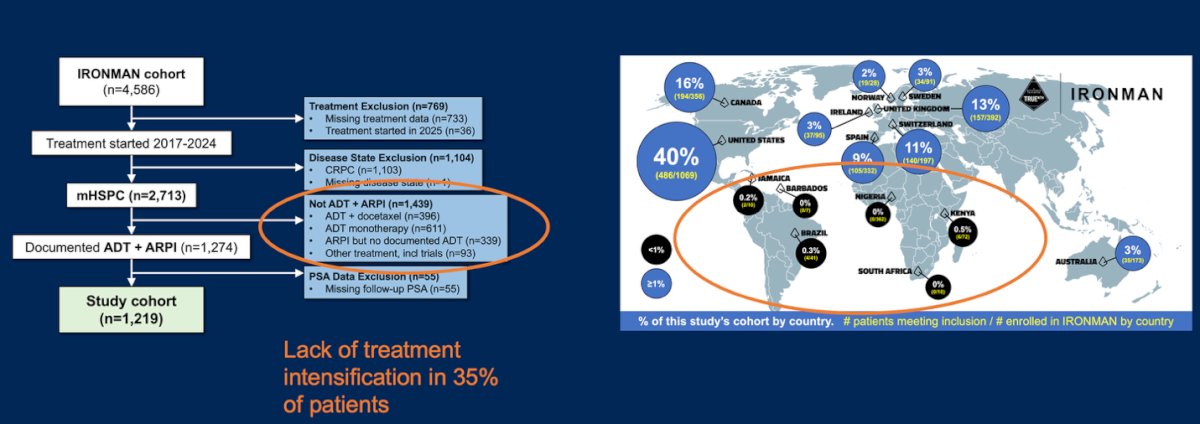
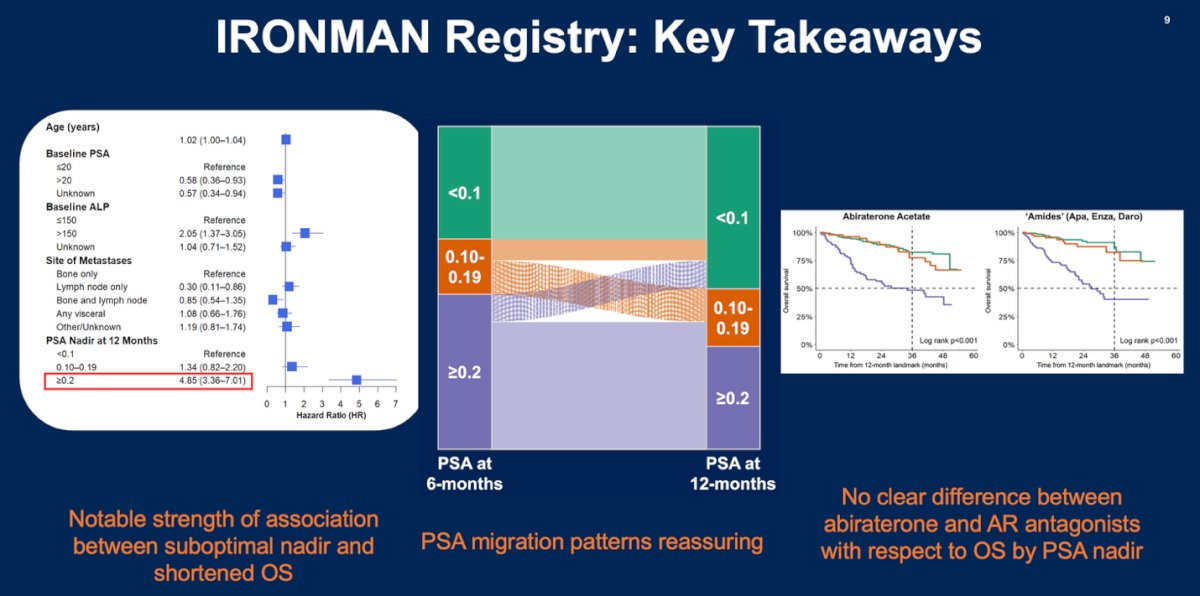
There are three key takeaways from the IRONMAN registry data:
- A strong association was observed between a suboptimal PSA nadir ≥0.2 ng/mL and shortened overall survival.
- PSA response migration patterns over time were consistent and clinically reassuring.
- No meaningful differences in overall survival were seen between patients treated with abiraterone versus AR antagonists when stratified by PSA nadir.
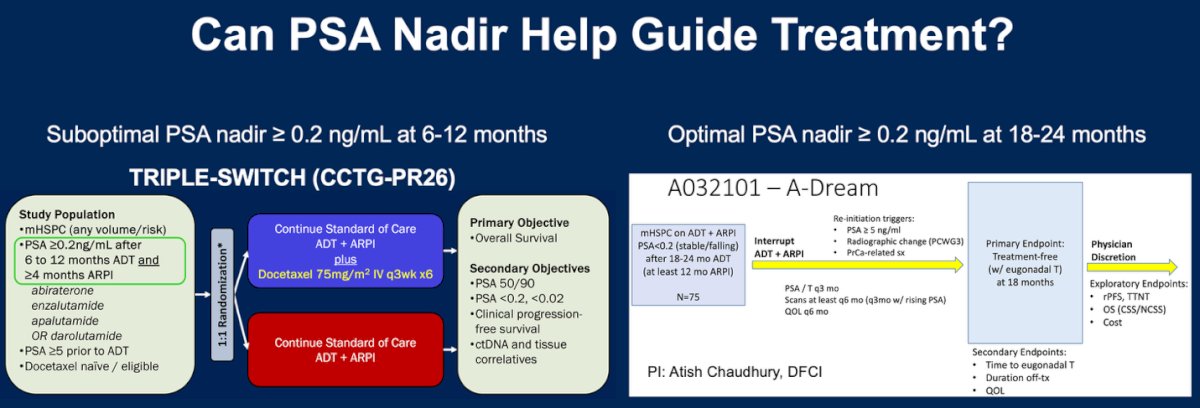
Dr. Aggarwal highlighted two key ongoing trials aiming to refine treatment strategies in mHSPC. The TRIPLE-SWITCH (CCTG-PR26) study uses a suboptimal PSA nadir (≥0.2 ng/mL at 6–12 months after ADT and ≥4 months of ARPI) as a trigger to randomize patients to intensification with docetaxel. The trial’s endpoints focus on clinically meaningful outcomes including improvement in overall survival, delayed time to CRPC and clinical progression, and preservation of quality of life.
He also discussed the A032101 “A-DREAM” study, which evaluates treatment interruption in patients with stable or falling PSA <0.2 ng/mL after 18–24 months of ADT (minimum 12 months of ARPI). This study aims to demonstrate non-inferiority of overall survival while extending eugonadal treatment-free intervals, delaying CRPC, and improving toxicity and quality of life. Results from both trials are eagerly awaited.
When choosing between ARPIs for patients with mCSPC, Dr. Aggarwal emphasized a patient-centered approach that considers toxicity profile, patient-reported quality of life, drug costs and insurance coverage, efficacy (OS and PFS), comorbidities, and patient preferences to guide optimal treatment selection. Notably, patient quality of life and toxicity profile should be regarded very highly when making these choices.

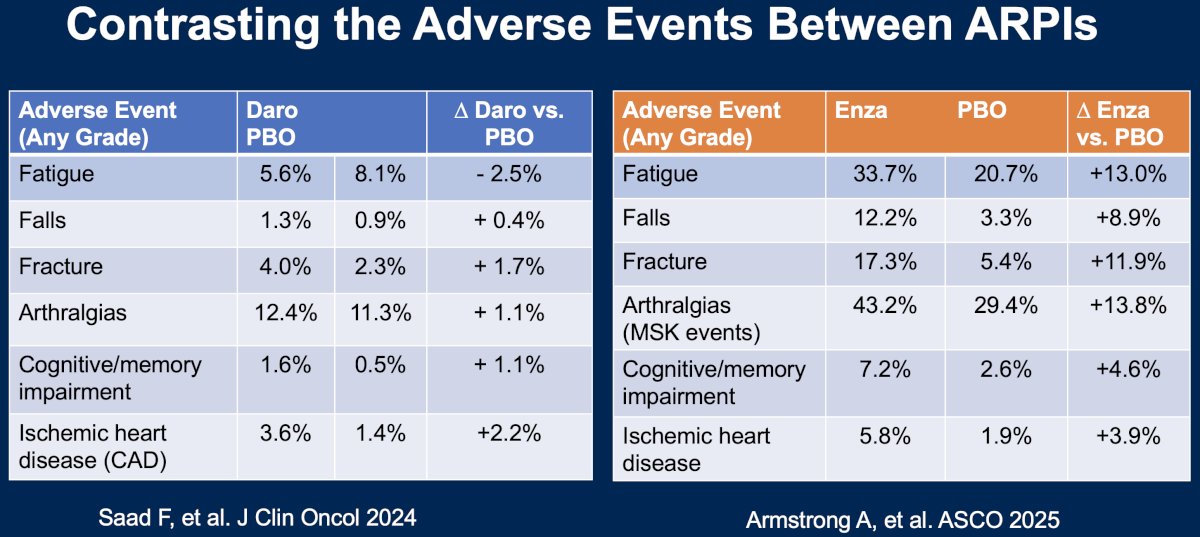
Moreover, while cross-trial comparisons have inherent limitations, contrasting adverse event profiles between darolutamide and enzalutamide may help inform ARPI selection in mCSPC. As shown below, fatigue was reported in 33.7% of patients receiving enzalutamide versus 5.6% with darolutamide; falls occurred in 12.2% vs. 1.3%, fractures in 17% vs. 4%, arthralgias in 43.2% vs. 12.4%, and cognitive or memory impairment in 7.2% vs. 1.6%, respectively. These differences underscore the importance of tailoring treatment based on patient preference, comorbidities, and toxicity profile.
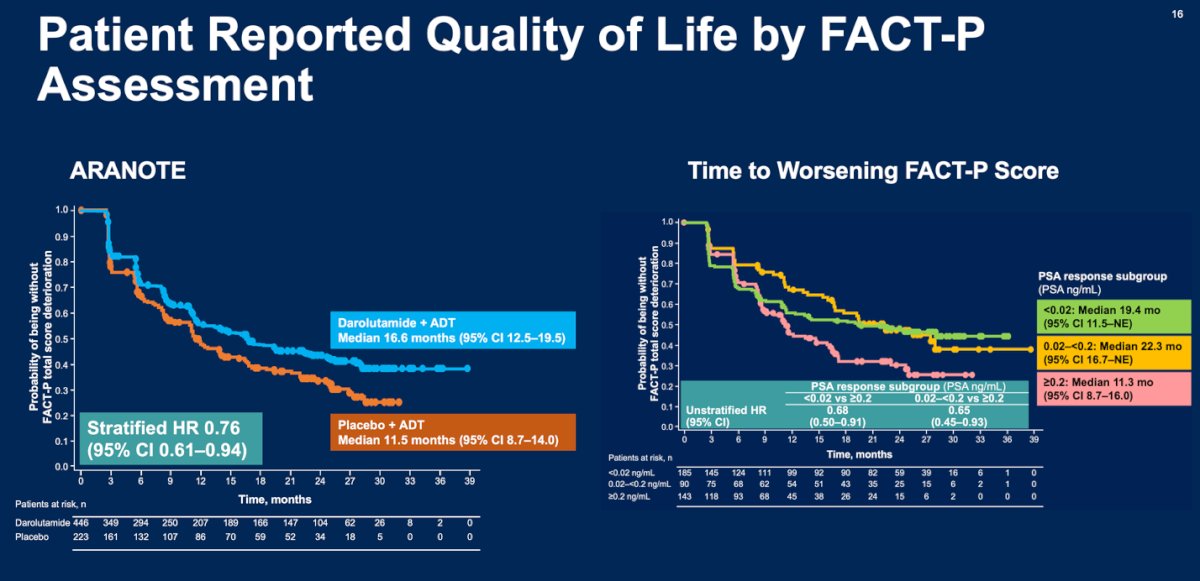
ARANOTE is the first phase 3 trial in mCSPC to demonstrate an improvement in time to deterioration in quality of life , showing a delay of 5 months as reported by Dr Morgans, as measured by FACT-P, with the addition of an ARPI to ADT. However, a key question remains: what drives this QoL improvement despite the addition of a second systemic therapy? Notably, time to worsening QoL occurred early in the control arm approximately 14 months before radiographic progression. Dr Aggarwal suggested that the depth of PSA nadir and PSA kinetics may be important contributing factors, as illustrated below.7
The ARACOG (AFT-47) trial is a randomized phase 2 study led by Dr. Alicia Morgans and sponsored by the Alliance Foundation. It enrolls men with mCRPC, nmCRPC, or mCSPC and randomizes them to receive either enzalutamide or darolutamide. Patients are stratified by age (<65, 65–80, >80) and undergo a series of cognitive and physical function assessments, including detailed cognitive testing such as the CANTAB test modules, TUG tests, blood draws (PSA, AR), and fMRI at weeks 0, 12, 24, and 52. Crossover is permitted at week 12 and week 24 for patients who meet pre-specified criteria, allowing evaluation of cognitive and functional impact of each ARPI over time.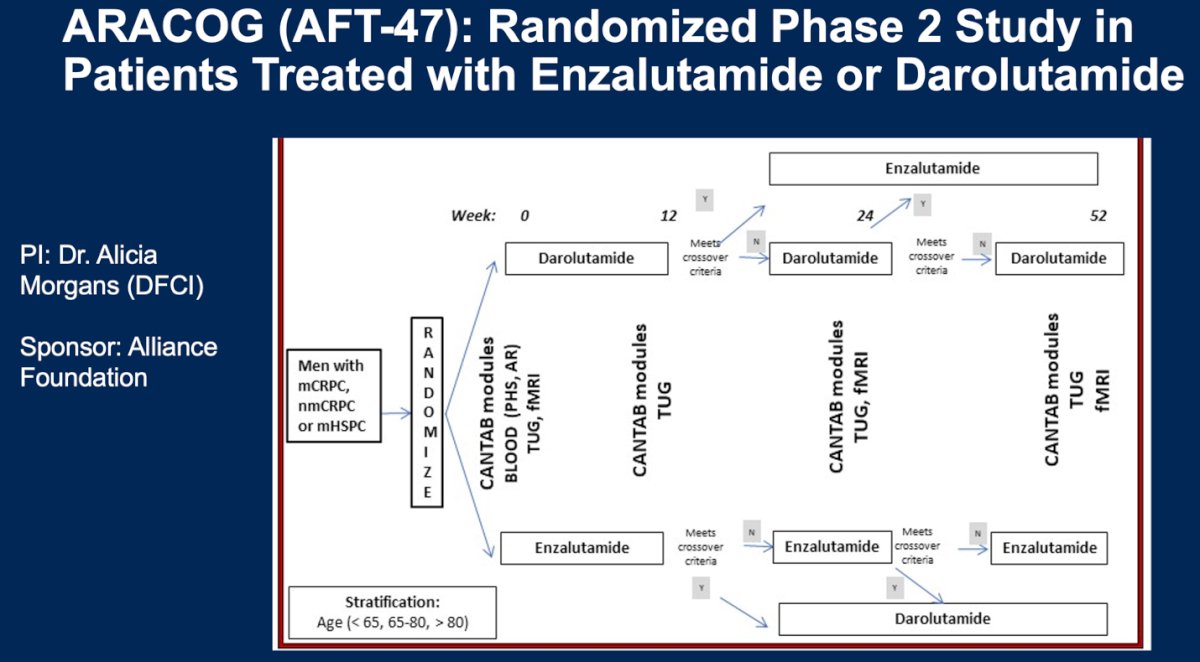
PTEN deficiency has emerged as a key biomarker identifying a high-risk subgroup within prostate cancer. Loss of PTEN function has been linked to worse clinical outcomes, with data suggesting an increased hazard of prostate cancer-specific mortality (HR 1.47; 95% CI, 1.07–2.04). Beyond genomic deletions, transcriptional profiling has provided additional evidence of PTEN deficiency at the transcriptome level, further refining patient stratification. Importantly, recent data suggest that PTEN loss may also have predictive implications particularly regarding enhanced sensitivity to docetaxel in the mCSPC setting raising the potential for biomarker-driven treatment intensification.
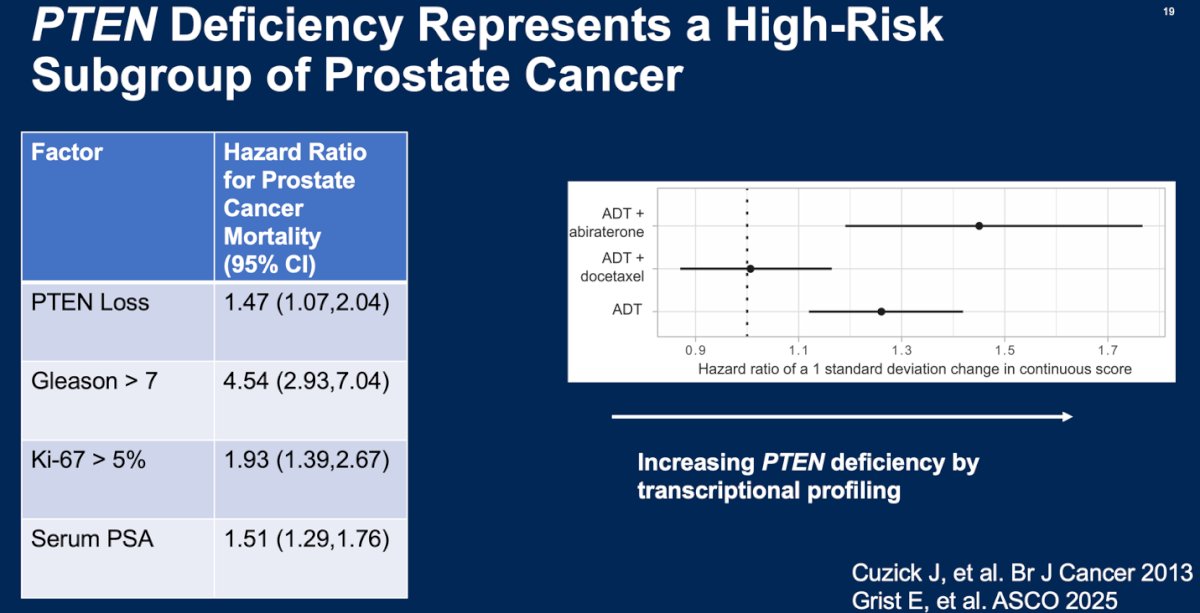
In the study presented by Dr. Grist using data from a STAMPEDE ancillary analysis, PTEN inactivation emerged as a potential predictive biomarker for docetaxel sensitivity in mCSPC. Patients with PTEN-deficient tumors appeared to derive greater overall survival benefit from the addition of docetaxel to ADT at treatment initiation, supporting its role in guiding treatment intensification. Notably, the predictive utility was further enhanced when PTEN inactivation was combined with a high Decipher genomic risk score, forming a composite biomarker that more effectively stratified patients likely to benefit from chemotherapy.
Dr. Aggarwal highlighted important caveats to the interpretation of the STAMPEDE ancillary analysis. While PTEN inactivation appears predictive of benefit from adding docetaxel to ADT in mCSPC, this finding requires prospective validation in randomized studies specifically evaluating triplet therapy (ADT + ARPI ± docetaxel), such as the ongoing TRIPLE-SWITCH trial. Additionally, it remains uncertain whether transcriptional profiling outperforms more widely accessible biomarkers, like homogeneous PTEN loss assessed by IHC or pathogenic alterations identified by NGS.
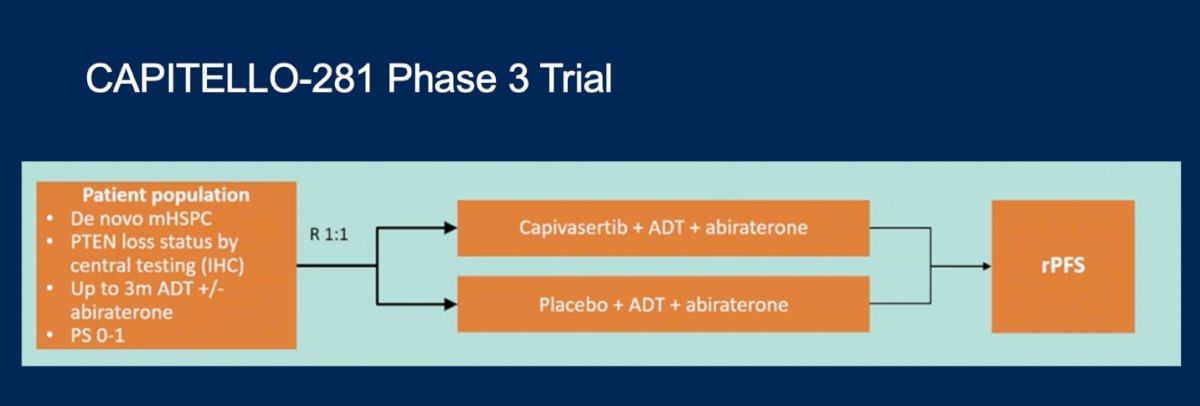
Lastly, Dr. Aggarwal discussed if PTEN deficiency can be leveraged for treatment selection in a pathway-specific manner. He highlighted the ongoing CAPItello-281 Phase 3 trial, which evaluates patients with de novo mCSPC stratified by PTEN loss status. In this study, participants are randomized to receive capivasertib (an AKT inhibitor) plus ADT and abiraterone versus placebo plus ADT and abiraterone, aiming to assess the therapeutic relevance of PI3K/AKT pathway targeting in the context of PTEN inactivation.
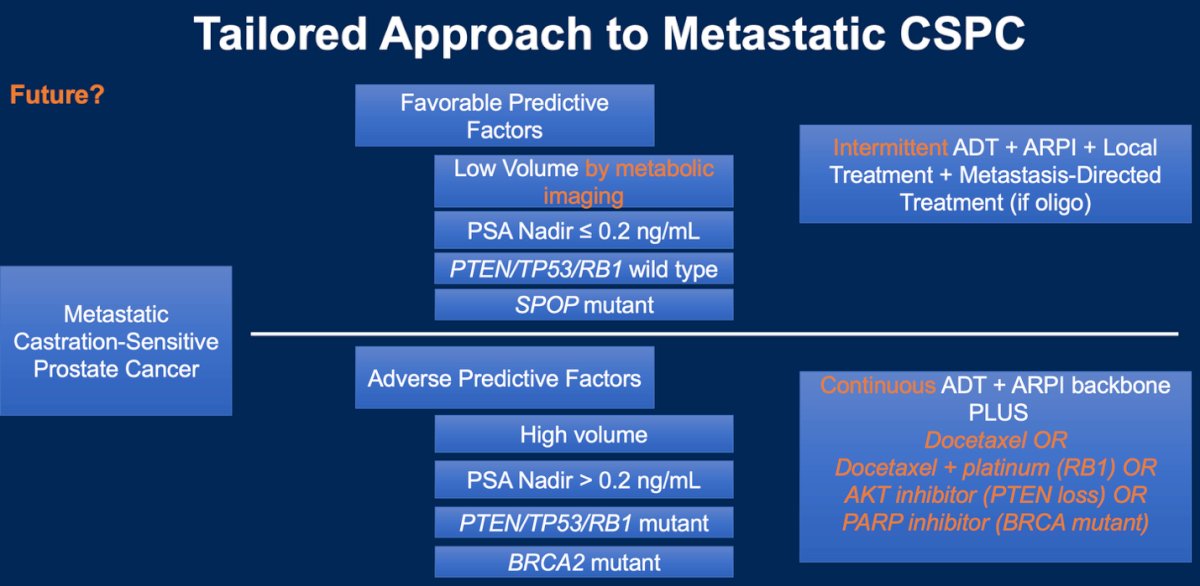
The future of mCSPC management is moving toward a more tailored approach, leveraging both clinical and molecular biomarkers to guide treatment decisions. Disease volume, PSA nadir, and genomic factors such as PTEN, TP53, and RB1 status as well as SPOP mutations and BRCA2 alterations may help clinicians identify patients who are more likely to benefit from treatment intensification or de-escalation. This evolving strategy aims to optimize outcomes while minimizing toxicity, offering a more personalized roadmap for managing metastatic castration-sensitive prostate cancer, as illustrated below.
Dr Aggarwal concluded his presentation with the following key takeaway points:
- PSA nadir is a validated and easy-to-understand prognostic biomarker, but it has not yet been validated to guide treatment intensification or de-intensification.
- Quality of life and toxicity data are important considerations when selecting an ARPI. Darolutamide may offer a favorable profile in this context.
- Somatic PTEN deficiency identifies a high-risk subset of mCSPC. However, further evidence from studies investigating triplet therapy and targeted AKT inhibition is needed to guide treatment decisions in this group.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:
- Chi KN, Agarwal N, Bjartell A, Chung BH, Pereira de Santana Gomes AJ, Given R, et al. Apalutamide for Metastatic, Castration-Sensitive Prostate Cancer. N Engl J Med. 2019;381(1):13–24. doi:10.1056/NEJMoa1903307.
- Armstrong AJ, Szmulewitz RZ, Petrylak DP, Holzbeierlein J, Villers A, Azad A, et al. ARCHES: Randomized, Phase III Study of Androgen Deprivation Therapy With Enzalutamide or Placebo in Men With Metastatic Hormone-Sensitive Prostate Cancer. J Clin Oncol. 2019;37(32):2974–86. doi:10.1200/JCO.19.00799.
- Fizazi K, Tran N, Fein L, Matsubara N, Rodriguez-Antolin A, Alekseev BY, et al. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. N Engl J Med. 2017;377(4):352–60. doi:10.1056/NEJMoa1704174.
- Hussain M, Tangen CM, Berry DL, et al. Intermittent versus continuous androgen deprivation in prostate cancer. N Engl J Med. 2013;368(14):1314-1325.
- Sweeney CJ, Chen YH, Carducci M, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N Engl J Med. 2015;373(8):737-746.
- Davis ID, Martin AJ, Stockler MR, et al. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N Engl J Med. 2019;381(2):121-131.
- Agarwal N, Khalaf D, Buonerba C, et al. Darolutamide plus androgen deprivation therapy versus androgen deprivation therapy alone in metastatic hormone-sensitive prostate cancer (ARANOTE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2024;25(5):455-467.
- Raval AD, Chen S, Littleton N, Constantinovici N, Goebell PJ. Real-world use of androgen-deprivation therapy intensification for metastatic hormone-sensitive prostate cancer: a systematic review. BJU Int. 2024;133(3):406-419