(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a prostate, testicular, and penile cancers poster session. Dr. Rana McKay presented the ongoing PREDICT (PREcision Diagnostics in Prostate Cancer Treatment) trial, a phase II, multi-arm, biomarker-based study (Alliance A032102).
Metastatic castration-resistant prostate cancer (mCRPC) is a lethal disease with overall survival ranging from 2 to 3 years. Advances in genomic sequencing have allowed for a deeper understanding of the molecular complexity of mCRPC with several actionable alterations now identified, fueling new biomarker-based treatment strategies.
Enhancer of Zeste Homolog 2 (EZH2) is significantly overexpressed in metastatic prostate cancer, especially in non-AR driven castration resistant tumors that harbor RB1 loss and neuroendocrine features. EZH2 is a member of a polycomb repressor complex 2 (PRC2) that represses downstream gene expression through histone H3 lysine 27 methylation (H3K27me). Preclinical studies have identified sensitivity of RB1 loss and NEPC models to EZH2 inhibition, along with evidence of a potential reversal of lineage plasticity towards a more luminal state.
Valemetostat tosylate (DS-3201b) is a dual inhibitor of EZH1 and EZH2. Aggressive variant prostate cancer, enriched for combined tumor suppressor loss, has demonstrated sensitivity to platinum-based chemotherapy. Additionally, SLFN11 overexpression has been associated with platinum sensitivity. As the understanding of the molecular underpinnings of mCRPC improves and availability of treatments expands, Dr. McKay and colleagues developed this phase II umbrella study to investigate rationally-designed biomarker-based treatments in mCRPC.
This is a multi-center, multi-arm, phase II umbrella study to investigate rationally-designed biomarker-based therapeutic strategies for patients with mCRPC. This study will include androgen receptor pathway inhibitor (ARPI) and taxane pre-treated/ineligible mCRPC patients who will undergo next-generation sequencing (NGS) followed by real-time molecular tumor board for arm allocation. Those with an actionable mutation will be randomized to valemetostat tosylate or cabazitaxel + carboplatin. Conversely, those without a study-defined DNA alteration will receive physician’s choice of cabazitaxel, Lu-PSMA, or AR-targeting agent.
The study includes a pre-registration step for arm determination by the molecular tumor board.
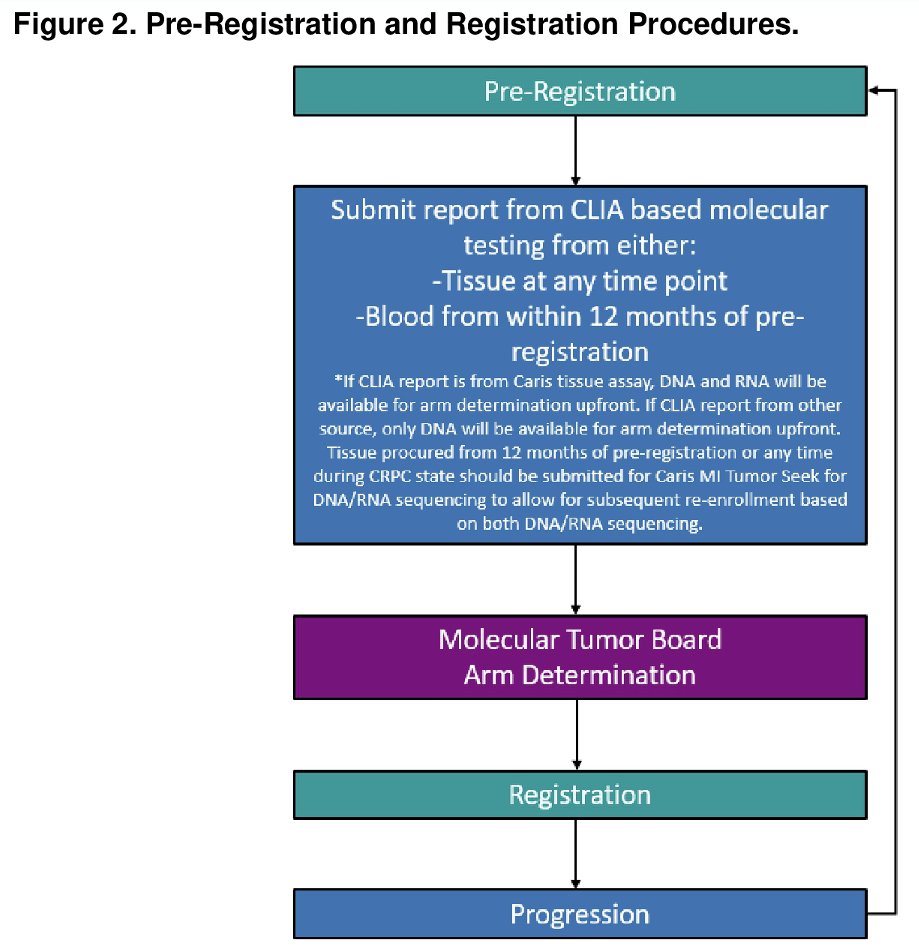
Arm assignments are determined by the underlying DNA and RNA alteration(s) present. The study is designed to accommodate future arms and biomarkers.

The primary study objective is objective response rate in patients with measurable disease by RECIST version 1.1. The secondary objectives are:
- Safety and tolerability
- Duration of response
- Radiographic progression-free survival (overall and 9-months landmark)
- PSA response (≥505 decline)
- Time to PSA progression
The full eligibility criteria are summarized below:
- Pre-Registration Eligibility
- Histological or cytological evidence of prostate cancer. All histologies are eligible.
- Measurable disease per RECIST version 1.1.
- Availability of tissue procured within 12 months of pre-registration or any time during CRPC state.
- Molecular report available performed as part of standard of care testing via any CLIA-certified next generation sequencing assay.
- Registration Eligibility
- Prior ARPI
- Prior taxane for either hormone sensitive or castration resistant disease unless taxane ineligible or refused. Patients with known BRCA1/2 mutations must have received prior PARP inhibitor. Prior Lu-PSMA-617 therapy is not mandated.
- No prior EZH inhibitors
- No prior cabazitaxel + carboplatin.
- Eastern Cooperative Oncology Group performance status 0-2.
- No major surgery within 4 weeks of registration.
- Adequate organ and bone marrow function.
- No significant cardiovascular disease:
- Myocardial infarction/unstable angina within 6 months prior to enrollment.
- New York Heart Association Class 3-4 heart failure.
- Uncontrolled hypertension.
- No moderate or severe hepatic impairment.
- Re-Registration Eligibility
- Qualifying DNA or RNA alteration.
- Progression mCRPC.
The statistical plan is as follows:
- A maximum of 64 patients with measurable disease and 94 patients with non-measurable disease for a total of 158 patients will be accrued to each treatment arm. This sample size incorporates an anticipated 5% dropout rate for patients that are registered into the study but withdraw prior to the start of treatment. Thus, the evaluation of the primary response endpoint is based on 61 patients per treatment arm. Patients who withdraw from the study after the start of treatment but prior to the 6-months response evaluation will be counted as a non-response.
- For each targeted therapy, the algorithm for the Simon two-stage minimax design applied to patients with measurable disease is as follows: Thirty-one patients are accrued in the first stage. If 6 or fewer responses are observed, accrual to that treatment will stop. If 7 or more responses are observed, an additional 30 patients will be entered onto the second stage of the study. At the conclusion of the second stage, if 18 or more responses are attained out of 61 patients, then the targeted therapy is considered sufficiently active. This per treatment study design has a type 1 error equal to 0.05 when the probability response is 0.20 and has power equal to 0.90 if the probability of response is 0.37.
Presented by: Rana McKay, MD, Associate Professor, Department of Medicine, University of California, San Diego, CA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.