(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to the Oral Abstract Session: Genitourinary Cancer—Prostate, Testicular, and Penile. Dr. Michael Ong Presented data on the Prognostic significance of PSA>0.2 after 6-12 months treatment for metastatic hormone-sensitive prostate cancer (mHSPC) intensified by androgen-receptor pathway inhibitors (ARPI) from A multinational real-world analysis of the IRONMAN registry.
For patients with metastatic hormone-sensitive prostate cancer (mHSPC), decisions regarding the addition of androgen receptor pathway inhibitors (ARPIs) or chemotherapy are typically made within the first 6 months after initiating androgen deprivation therapy (ADT). However, treatment outcomes remain heterogeneous. While some patients experience a rapid decline in PSA and maintain long-term disease control, others develop early resistance despite receiving intensive therapy. Early prognostication—particularly within 6 to 12 months of starting treatment may offer an opportunity to better personalize therapeutic strategies and improve long-term outcomes.
Dr. Ong highlighted that early absolute PSA levels are a strong prognostic marker in mHSPC. Post hoc analyses from multiple randomized trials have consistently shown that achieving a PSA <0.2 ng/mL at 3 to 7 months is associated with favorable prognosis, regardless of treatment type, whether ADT alone (SWOG 9346), ADT + docetaxel (CHAARTED), or ADT + ARPIs (LATITUDE, TITAN, ARCHES, ENZAMET).1-6
More recent data suggest that "lower is better." Achieving a PSA <0.02 ng/mL between 3 and 12 months correlates with even better outcomes, as demonstrated in trials such as TITAN and ARANOTE.7 However, real-world data supporting these thresholds remains limited and warrants further investigation.
This study was designed to address two key clinical questions in the real-world management of mHSPC:
- Are PSA levels at 6 and 12 months prognostic for outcomes in patients receiving ADT plus an ARPI?
- Can PSA levels after 6 to 12 months of therapy help guide treatment intensification or de-escalation strategies?
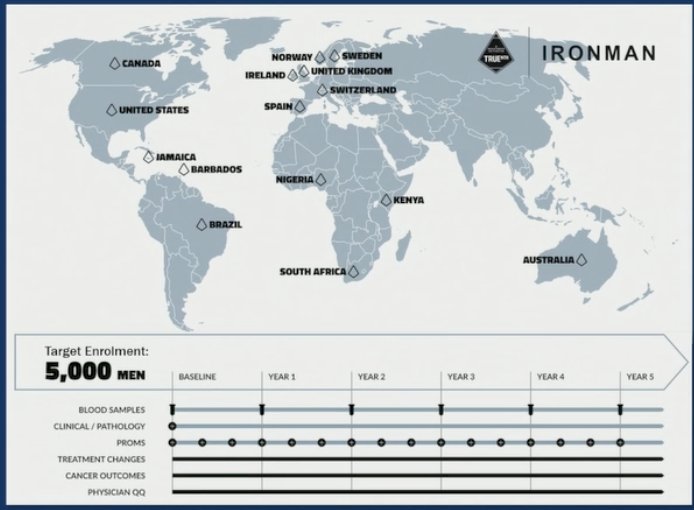
To address these questions, investigators utilized data from the IRONMAN Registry, a prospective, international cohort that includes over 4,600 patients with mHSPC and castration-resistant prostate cancer (CRPC). The registry spans 123 active sites across 15 countries and captures comprehensive, real-world data, including patient demographics, blood samples, clinical outcomes, and patient- and physician-reported questionnaires as illustrated below.
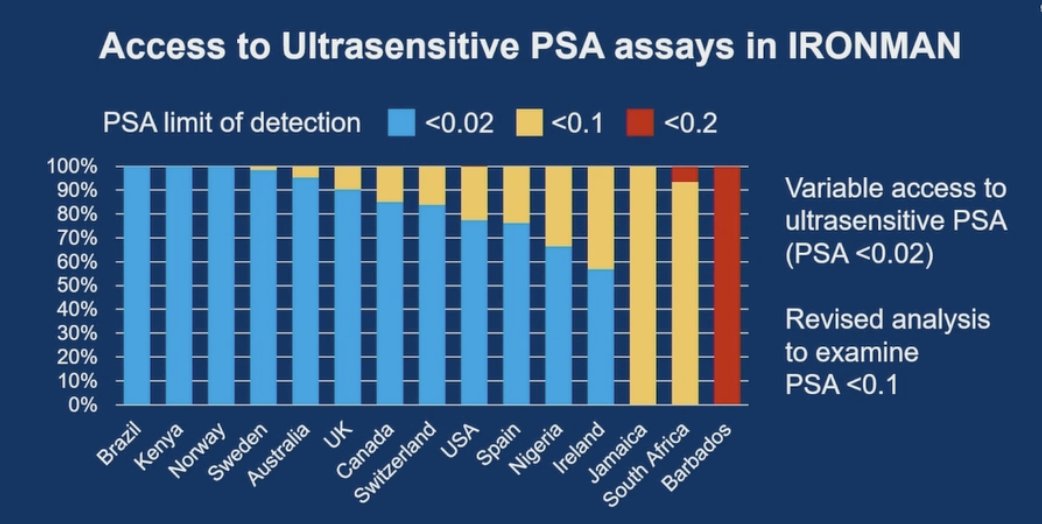
Dr. Ong noted that the initial analysis used a PSA threshold of <0.2 ng/mL; however, based on feedback and the availability of ultrasensitive PSA testing at select centers, the analysis was revised to also examine a lower cutoff of <0.02 ng/mL. Recognizing the variability in access to ultrasensitive assays across sites, the team conducted a revised analysis using an intermediate threshold of PSA <0.1 ng/mL to enhance generalizability
This analysis included patients with mHSPC from the IRONMAN Registry who were treated with ADT plus an ARPI, with or without docetaxel, and had available PSA data for at least 12 months. Patients were stratified into three PSA groups at both 6 and 12 months after ADT initiation: <0.1 ng/mL, 0.10–0.19 ng/mL, and ≥0.2 ng/mL.
Primary outcomes were assessed using 12-month and 6-month landmark analyses. Conditional overall survival and progression-free survival (PFS) were evaluated from each landmark to the time of death, progression, or censoring. Multivariable Cox proportional hazards models were constructed to assess the association between 12-month PSA strata and survival outcomes, adjusting for relevant clinical confounders.
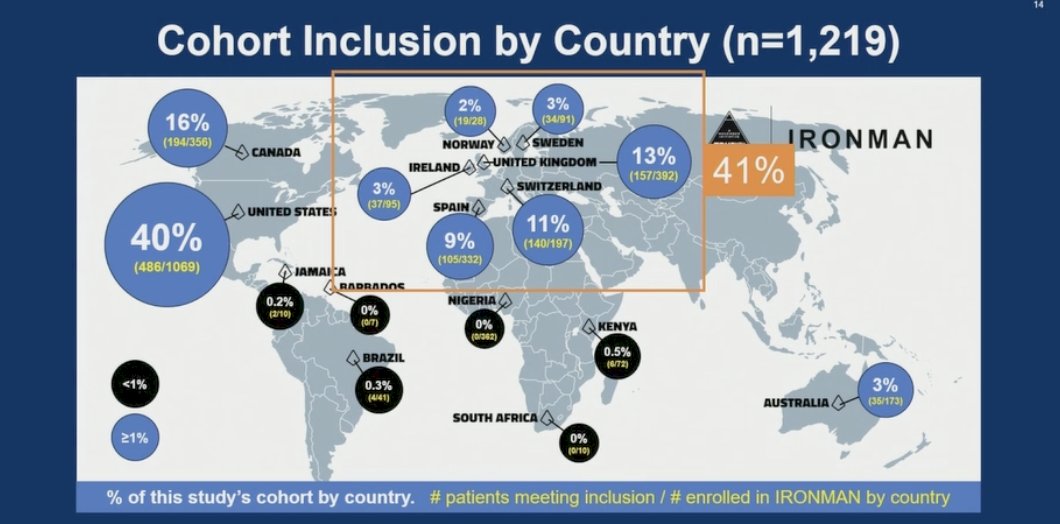
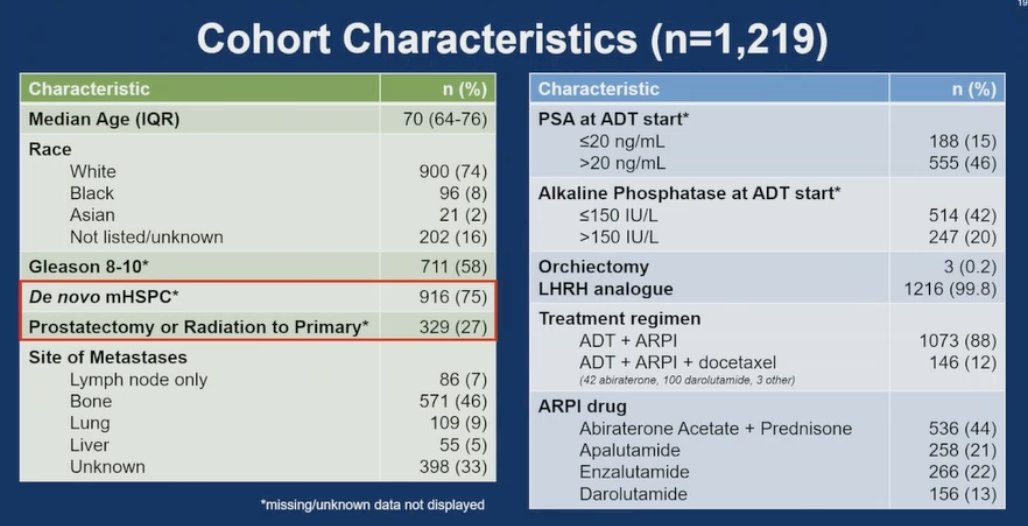
A total of 4,586 patients were in the IRONMAN registry, and 1,219 were included in the analysis. Geographically, the majority were from North America (56%), comprising 40% from the United States and 16% from Canada, followed by Europe (41%). Less than 1% of patients were enrolled from South America, Central America, and Africa.
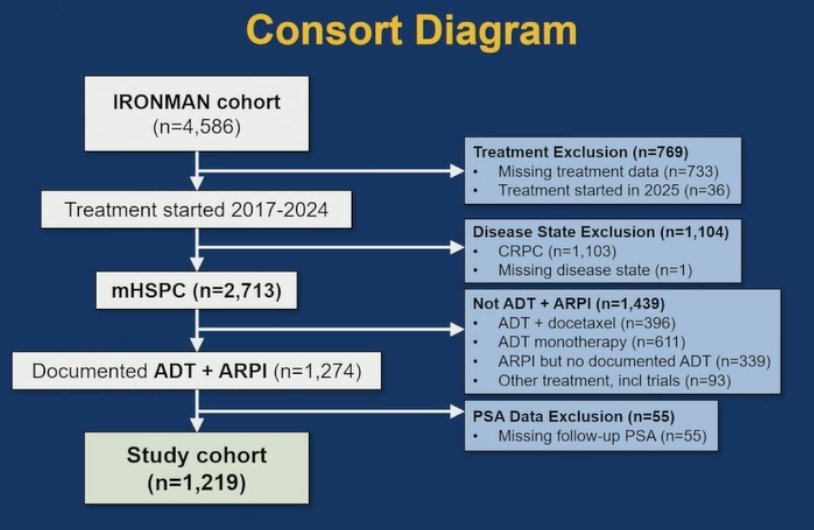
The CONSORT diagram for the study is shown below. Notably, out of 2,713 patients with mHSPC, 1,274 received documented treatment with ADT plus an ARPI. Of these, 55 patients were excluded due to missing follow-up PSA data.
The median age of the cohort was not specified, but 75% had de novo mHSPC while 27% had metachronous disease. Most patients (88%) received doublet therapy, and 12% received triplet therapy. Abiraterone was used in 44% of cases, with the remaining patients treated with “amide” agents.
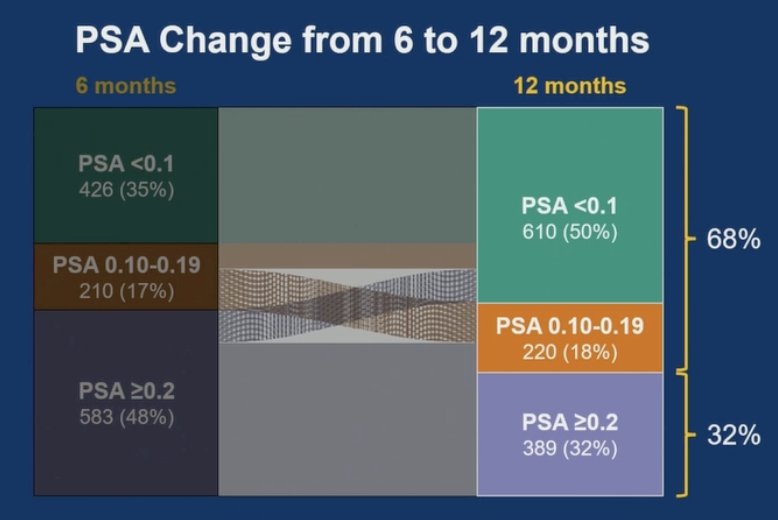
The Sankey diagram visually demonstrates the longitudinal change in PSA levels from 6 to 12 months in patients with mHSPC receiving ADT + ARPI. At 6 months, 52% of patients had a PSA <0.2 ng/mL, while 48% had a PSA ≥0.2. By 12 months, 68% of the overall cohort had achieved PSA <0.2, indicating that a notable proportion of patients with suboptimal early PSA responses improved by the 12-month landmark. Specifically, some patients initially in the ≥0.2 ng/mL group showed continued decline (only 32% had a PSA ≥0.2 at 12 months), highlighting the dynamic nature of PSA responses and the potential utility of 12-month PSA in refining prognostication.
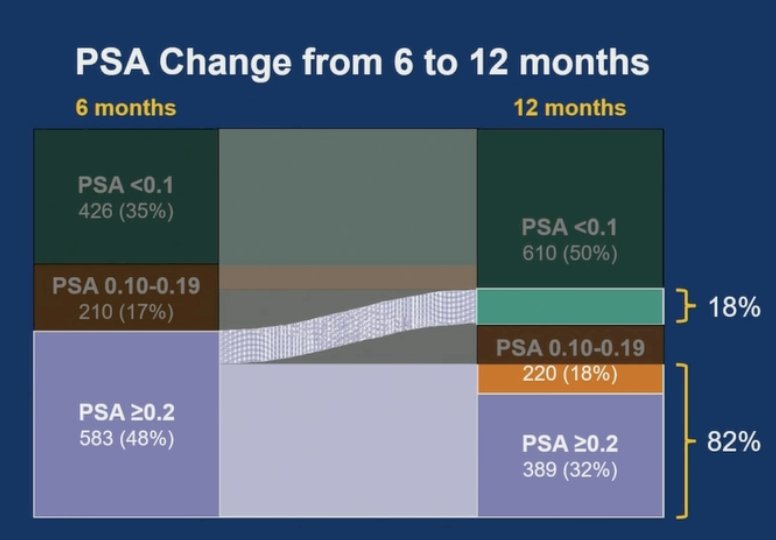
Dr. Ong noted that among patients with a PSA ≥0.2 at 6 months, the majority (82%) continued to have a PSA >0.1 at 12 months, with only 18% achieving a PSA decline to <0.1. This highlights the limited likelihood of achieving deeper PSA responses after 6 months in patients with persistently elevated PSA.
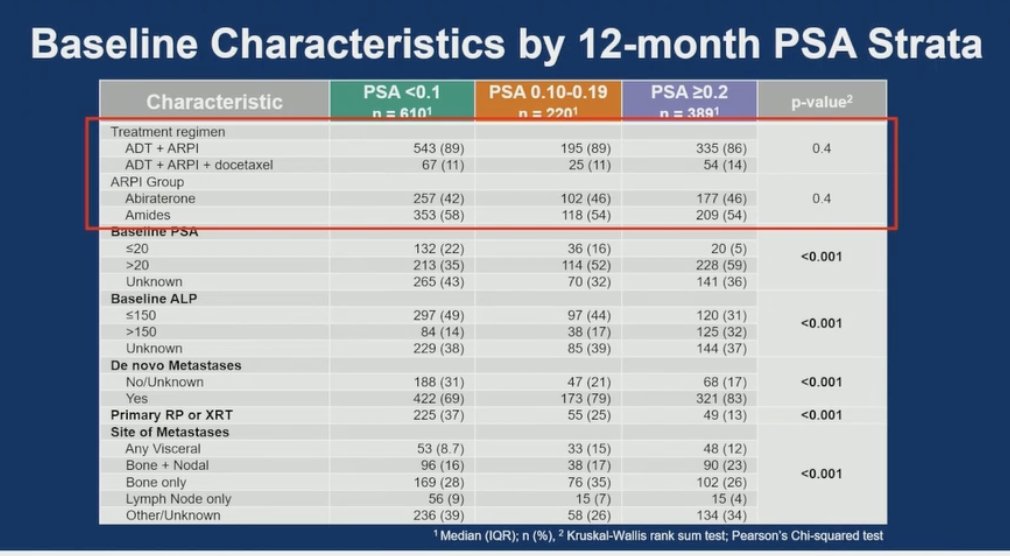
Notably, the treatment regimen, whether doublet, triplet therapy, or the specific ARPI used, was not associated with PSA strata at 12 months as shown below.
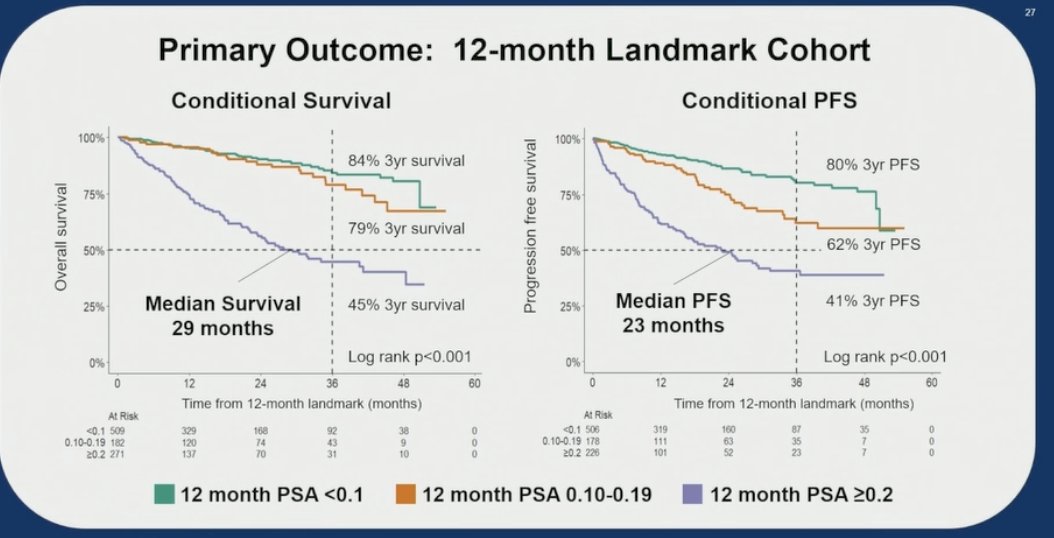
In this 12-month landmark analysis from the IRONMAN registry, PSA levels at 12 months were strongly associated with both OS and PFS in patients with mHSPC treated with ADT + ARPI. Patients with PSA <0.1 at 12 months had the most favorable outcomes, with an 84% 3-year OS rate and 80% 3-year PFS. Those with PSA 0.10–0.19 had slightly lower outcomes (79% OS and 62% PFS at 3 years), while patients with PSA ≥0.2 had markedly poorer prognoses, with a 3-year OS of 45% and PFS of 41%. Median survival was 29 months, and median PFS was 23 months. Notably, these differences were significant for OS and PFS.
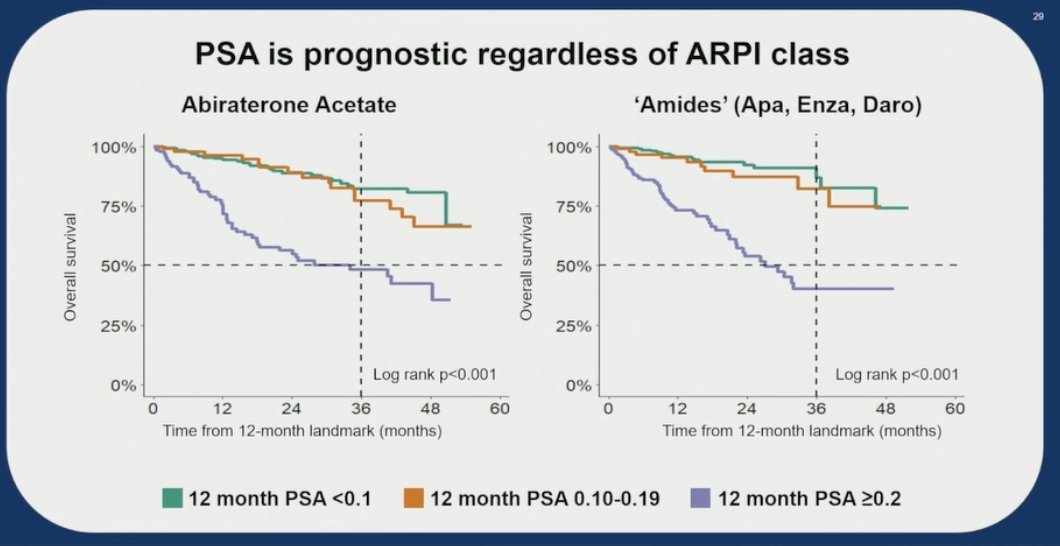
The data further support that PSA at 12 months is prognostic regardless of ARPI class (Abiraterone or “Amides”), or whether patients received doublet or triplet therapy. Across treatment intensities and ARPI types, patients with lower PSA levels consistently experienced better survival and progression-free outcomes.
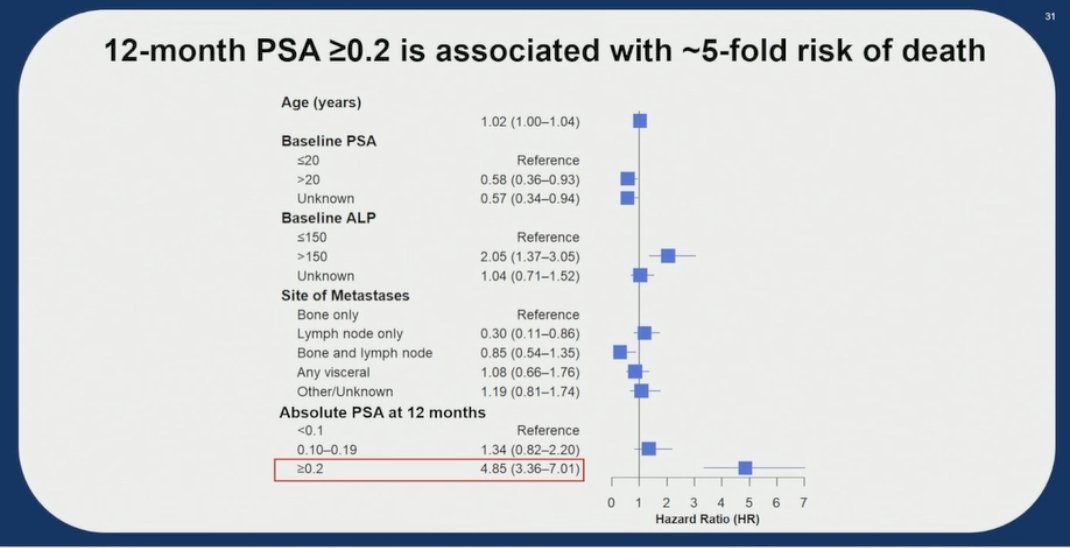
Multivariable Cox regression analysis demonstrated that 12-month PSA is a strong independent prognostic factor. Specifically, patients with PSA ≥0.2 at 12 months had nearly a fivefold increased risk of death compared to those with PSA <0.1 (HR 4.85; 95% CI 3.36–7.01).
Dr Ong acknowledges that this analysis has some limitations. First, missing data, particularly baseline PSA values prior to ADT initiation, may have influenced the univariable and multivariable analyses. Second, variability in PSA assay sensitivity across different laboratories and countries may have introduced inconsistencies, especially in distinguishing very low PSA values. Lastly, PFS was captured using a composite endpoint that included clinical, biochemical, and radiographic progression, which may have introduced heterogeneity in event classification across sites.
Dr. Ong concluded with the following key takeaways:
- Absolute PSA levels at 6 to 12 months after initiating ADT are prognostic in patients with mHSPC receiving ADT + ARPI.
- A PSA ≥0.2 ng/mL at 6–12 months is associated with poor prognosis. These patients may benefit from enrollment in clinical trials exploring treatment escalation strategies.
- Conversely, patients with PSA <0.2 ng/mL, particularly those achieving levels <0.1 ng/mL tend to have a favorable prognosis and may be candidates for future de-escalation approaches.
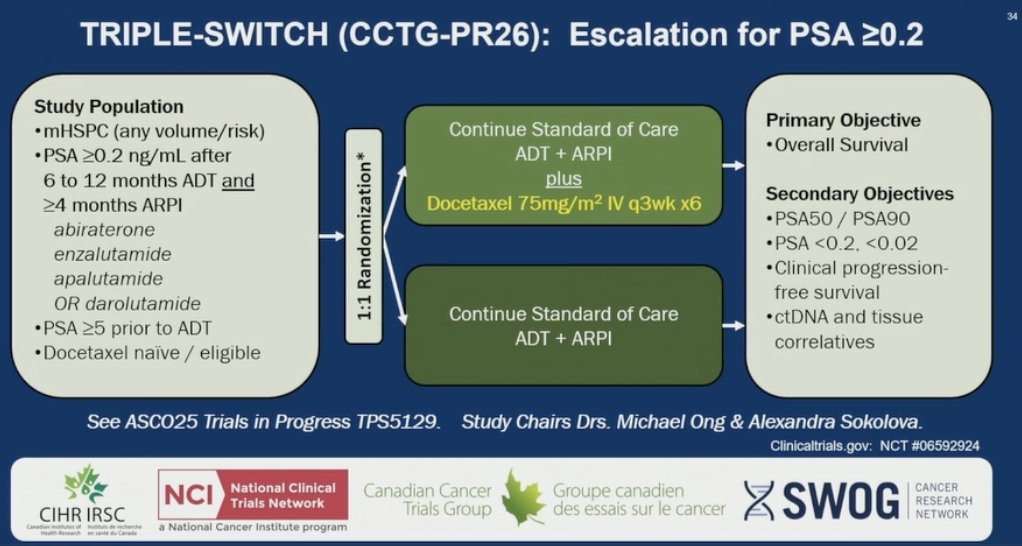
Dr. Ong highlighted that based on these findings, the TRIPLE-SWITCH (CCTG-PR26) trial was launched to assess escalation for patients with mHSPC and PSA ≥0.2 after 6–12 months of ADT + ARPI. Patients are randomized 1:1 to continue standard of care or receive docetaxel added to ADT + ARPI. The primary objective is overall survival, with secondary endpoints including PSA responses, PFS, and ctDNA correlatives.
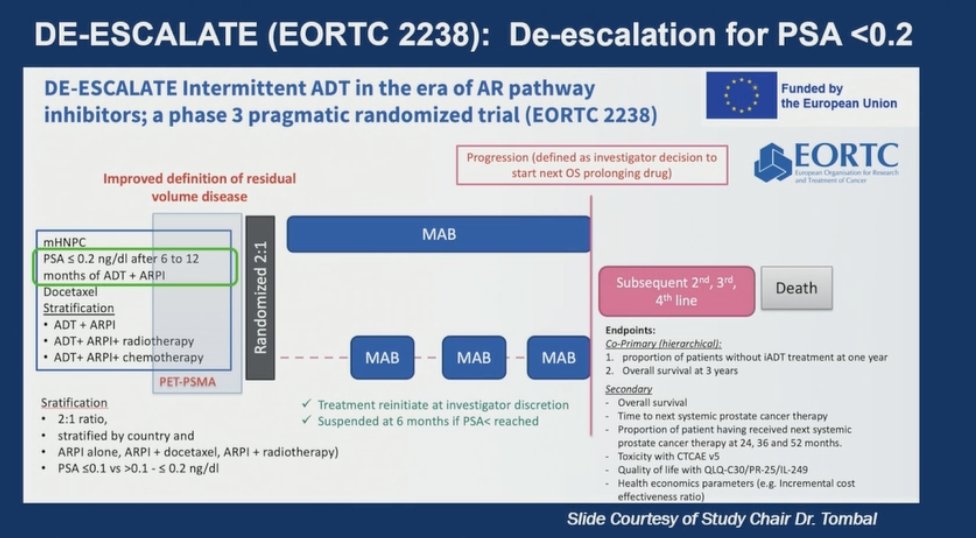
Lastly, Dr Ong highlighted the ongoing DE-ESCALATE (EORTC 2238) trial, a pragmatic, phase 3 randomized study evaluating intermittent ADT in patients with mCSPC who have achieved a PSA ≤0.2 ng/mL after 6–12 months of ADT + ARPI. Patients are randomized 2:1 to intermittent versus continuous ARPI-based therapy, stratified by country, treatment regimen, and PSA levels (≤0.1 vs >0.1–≤0.2). Treatment is paused at 6 months if PSA remains suppressed, with reinitiation at the investigator’s discretion upon PSA progression
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Reference:
- Hussain M, Tangen CM, Berry DL, Higano CS, Crawford ED, Liu G, et al. Intermittent versus continuous androgen deprivation in prostate cancer. N Engl J Med. 2013;368(14):1314–25.
- Sweeney CJ, Chen YH, Carducci M, Liu G, Jarrard DF, Eisenberger M, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N Engl J Med. 2015;373(8):737–46.
- Fizazi K, Tran N, Fein L, Matsubara N, Rodriguez-Antolin A, Alekseev BY, et al. Abiraterone plus prednisone in newly diagnosed high-risk metastatic castration-sensitive prostate cancer. N Engl J Med. 2017;377(4):352–60.
- Chi KN, Agarwal N, Bjartell A, Chung BH, Pereira de Santana Gomes AJ, Given R, et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N Engl J Med. 2019;381(1):13–24.
- Armstrong AJ, Szmulewitz RZ, Petrylak DP, Holzbeierlein J, Villers A, Azad A, et al. ARCHES: A randomized, Phase III study of androgen deprivation therapy with enzalutamide or placebo in men with metastatic hormone-sensitive prostate cancer. J Clin Oncol. 2019;37(32):2974–86.
- Davis ID, Martin AJ, Stockler MR, Begbie S, Chi KN, Chowdhury S, et al. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N Engl J Med. 2019;381(2):121–31.
- Saad F, Vjaters E, Shore N, Olmos D, Xing N, Pereira de Santana Gomes AJ, Cesar de Andrade Mota A, Salman P, Jievaltas M, Ulys A, Jakubovskis M, Kopyltsov E, Han W, Nevalaita L, Testa I, Le Berre MA, Kuss I, Haresh KP; ARANOTE Study Investigators. Darolutamide in Combination With Androgen-Deprivation Therapy in Patients With Metastatic Hormone-Sensitive Prostate Cancer From the Phase III ARANOTE Trial. J Clin Oncol. 2024 Dec 20;42(36):4271-4281. doi: 10.1200/JCO-24-01798. Epub 2024 Sep 16. PMID: 39279580; PMCID: PMC11654448.