(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to the Oral Abstract Session: Genitourinary Cancer—Prostate, Testicular, and Penile. Dr. Rana McKay presented a multicenter, randomized, phase 2, investigator-initiated ETCTN trial of olaparib + radium-223 vs. radium-223 in men with castration-resistant prostate cancer with bone metastases (COMRADE): Initial efficacy and biomarker analysis.
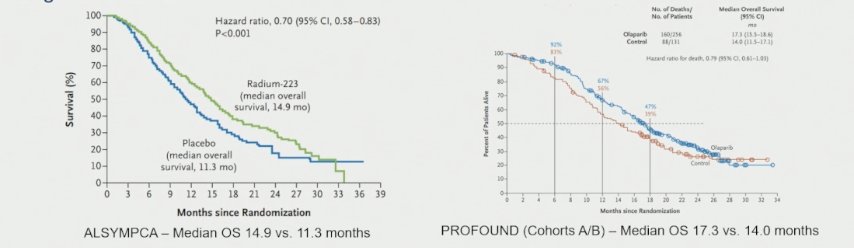
Castration-resistant prostate cancer (CRPC) remains a lethal condition, with over 90% of patients eventually developing bone metastases, which drive both morbidity and mortality. Radium-223, a targeted alpha emitter, has demonstrated an overall survival benefit in patients with bone-predominant metastatic CRPC.1 Separately, Olaparib, a potent PARP inhibitor has shown clinical efficacy in men with metastatic CRPC harboring homologous recombination repair (HRR) gene alterations, as evidenced by the PROfound trial.2
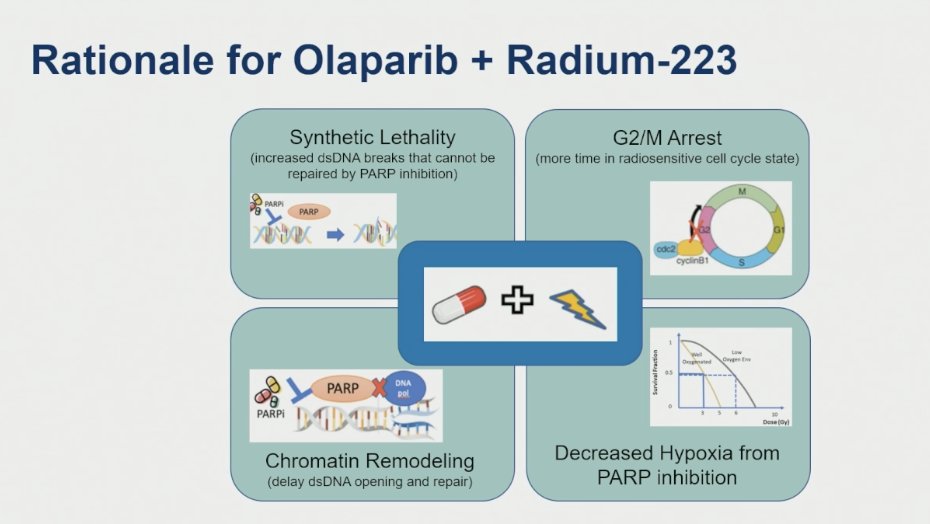
Dr. McKay outlined the rationale for combining radium-223 with PARP inhibition, highlighting four complementary mechanisms that enhance antitumor activity. First, synthetic lethality arises when radium-induced double-strand DNA breaks cannot be repaired due to PARP inhibition, leading to tumor cell death. Second, olaparib induces G2/M cell cycle arrest, prolonging the duration that cells remain in a radiosensitive phase. Third, PARP inhibition alters chromatin structure, delaying DNA repair by restricting access to damaged DNA. Finally, olaparib reduces tumor hypoxia by lowering cellular oxygen consumption, which may further potentiate the effects of radiation. Together, these synergistic mechanisms support ongoing investigation of this combination in mCRPC.
The investigators hypothesize that combining olaparib with radium-223 will be feasible and safe, while also demonstrating anti-tumor activity in patients with mCRPC with bone metastases.
The COMRADE trial was a Phase I/II study enrolling patients with mCRPC who had an ECOG performance status of 0–1, progressive disease, and at least two bone metastases. Eligible patients could not have visceral metastases or lymphadenopathy >4 cm, and prior treatment with radium-223 was not allowed. Prior docetaxel use was permitted, and concurrent use of bone-protecting agents was mandated unless contraindicated.
The Phase I portion established the recommended dose of olaparib. In the Phase II, patients were randomized 1:1 to receive olaparib plus radium-223 or radium-223 alone. The primary endpoint was radiographic progression-free survival (rPFS), with stratification by prior docetaxel use. Crossover to combination therapy was permitted for patients initially randomized to radium monotherapy. The study design is shown in detail below.
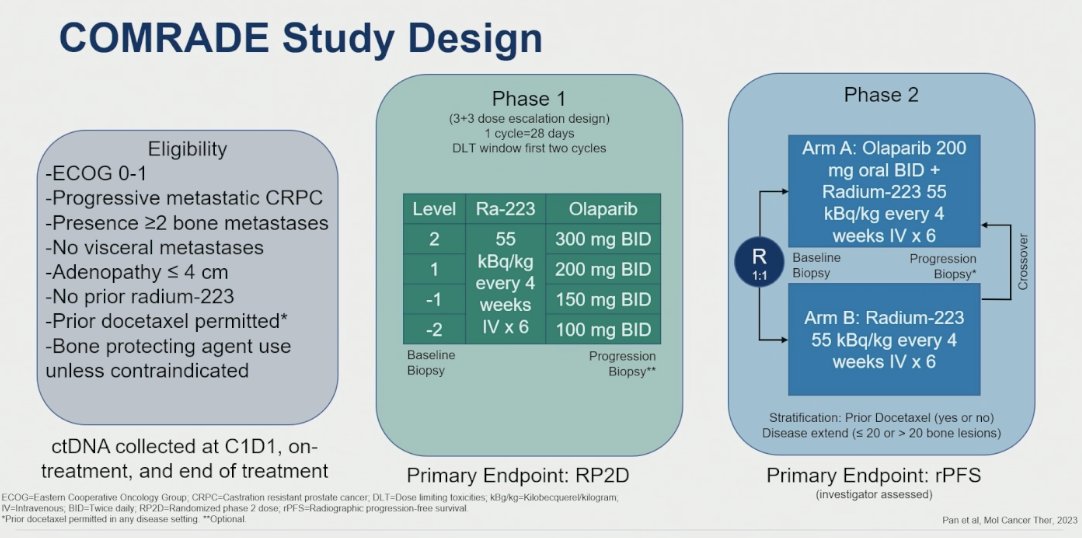
rPFS defined by PCWG3 and RECIST v1.1 criteria was the primary endpoint. With a planned enrollment of 120 patients, the study had 88% power to detect a 43% reduction in risk of progression (HR 0.57) using a 1-sided alpha of 0.10. One interim futility analysis was planned after 40 rPFS events, with a stopping boundary set at an estimated HR >1.05. Secondary endpoints included rPFS by disease extent, prior docetaxel exposure, and HRR mutation status (via tumor tissue and liquid biopsy), as well as PSA50, alkaline phosphatase reduction of 30% (ALK30), overall response rate (ORR), PSA progression, time to ALK progression, time to first subsequent treatment, time to symptomatic skeletal events (SSE), and overall survival.
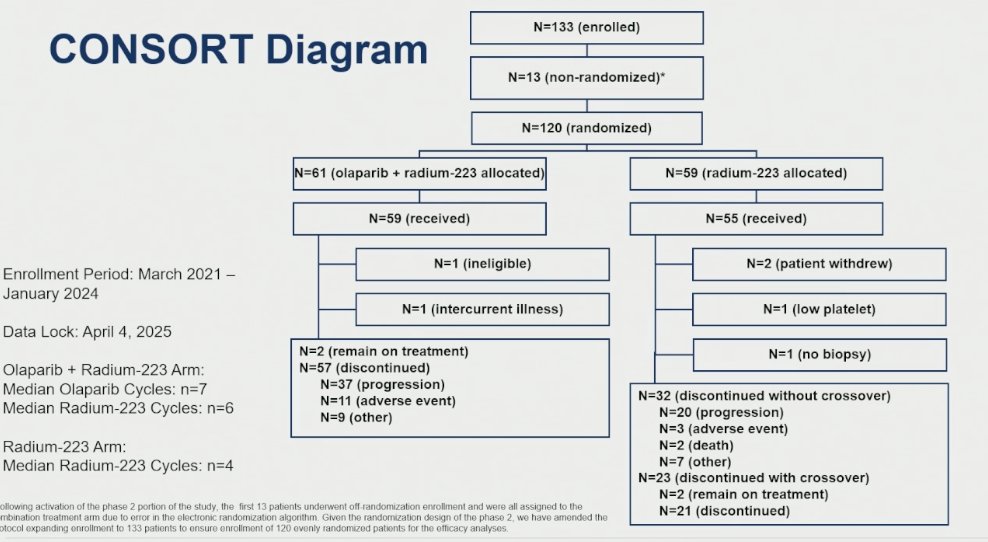
A total of 133 patients were enrolled in the COMRADE trial; however, due to a randomization algorithm malfunction, 13 patients were not successfully randomized. After protocol amendment, 120 patients were properly randomized in a 1:1 fashion to receive either olaparib plus radium-223 (n=59) or radium-223 alone (n=59). Dr. McKay emphasized the importance of this correction to ensure the integrity of the randomized cohort, which is reflected in the updated CONSORT diagram.
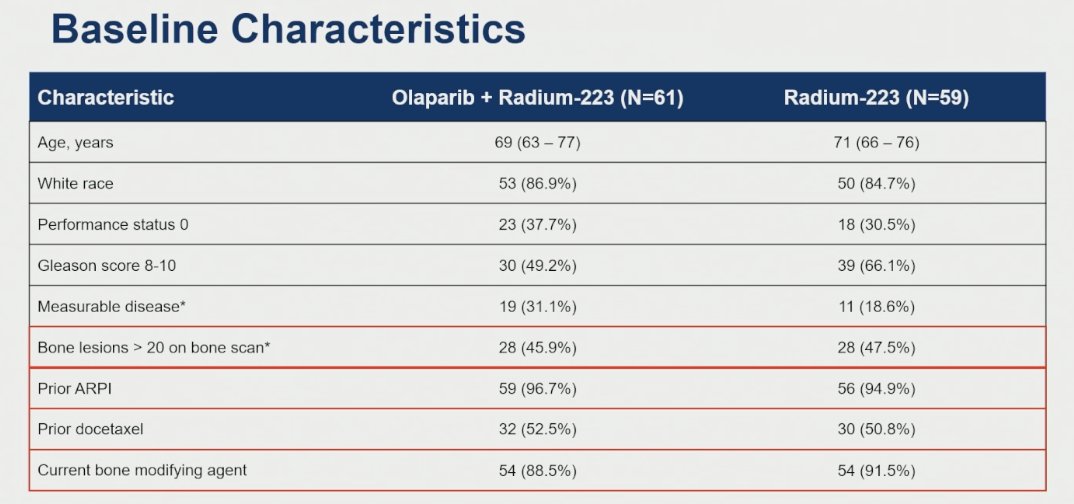
Baseline characteristics were well balanced between treatment arms. Notably, over 45% of patients in each group had more than 20 bone metastases, underscoring a high disease burden. This was a heavily pretreated population, with more than 95% having received prior AR pathway inhibitors and over 50% having received prior docetaxel. Additionally, the majority of patients were on bone-protective agents at baseline (88.5% in the combination arm and 91.5% in the radium monotherapy arm).
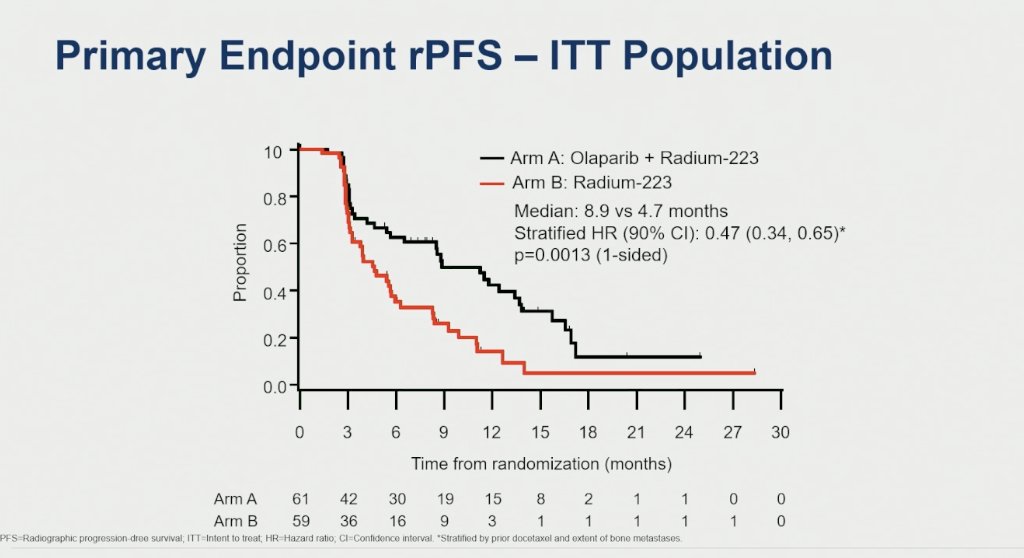
This was a positive study. The addition of olaparib to radium-223 significantly prolonged rPFS compared to radium-223 alone, with a median rPFS of 8.9 months versus 4.7 months, respectively. The stratified hazard ratio was 0.47 (90% CI: 0.34–0.65; 1-sided p=0.0013), indicating a 53% reduction in the risk of progression or death.
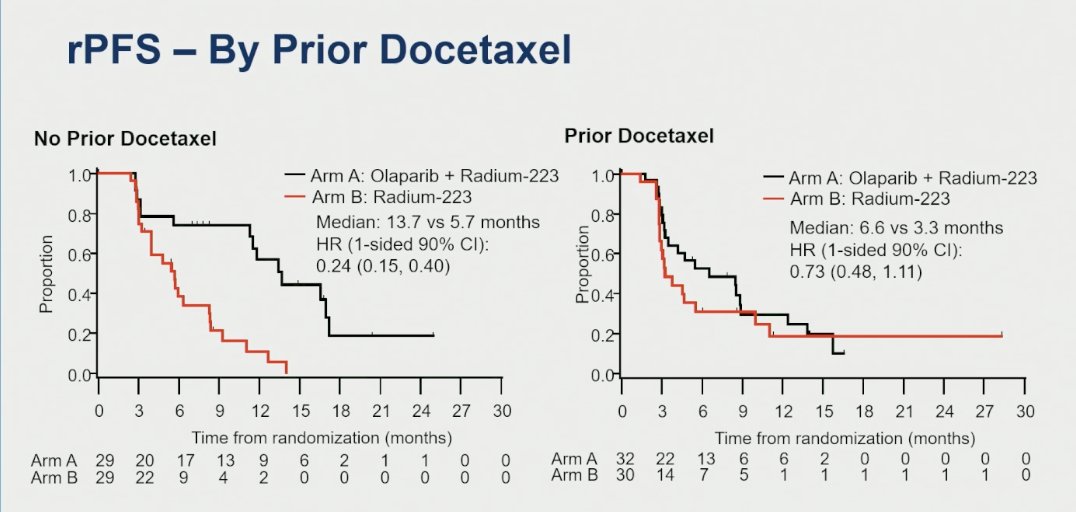
Notably, the greatest benefit from the combination of olaparib and radium-223 was observed in patients who had not received prior docetaxel. In this subgroup, median rPFS was significantly prolonged to 13.7 months compared to 5.7 months with radium-223 alone, with a stratified hazard ratio of 0.24 (1-sided 90% CI: 0.15–0.40).
A prespecified analysis of rPFS by extent of bone metastases revealed the most pronounced benefit among patients with ≤20 bone metastases. In this subgroup, the combination of olaparib and radium-223 extended median rPFS to 13.4 months versus 4.2 months with radium alone, corresponding to a hazard ratio of 0.21 (1-sided 90% CI: 0.13–0.33), indicating a 79% reduction in the risk of progression or death.

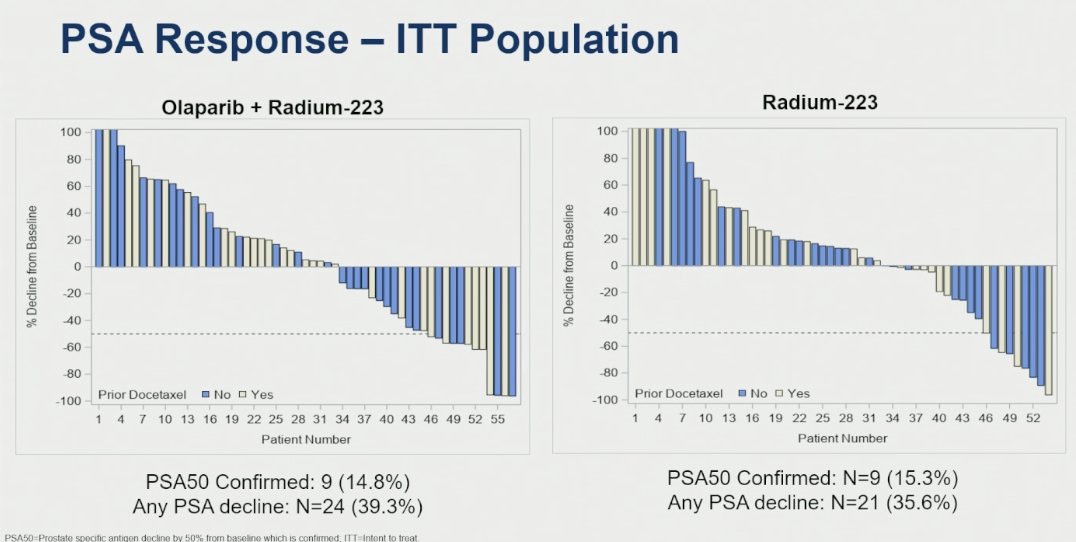
In the combination arm (olaparib + radium-223), 14.8% of patients achieved a confirmed ≥50% PSA decline (PSA50), and 39.3% experienced any PSA decline. In comparison, in the radium-223 monotherapy arm, 15.3% of patients achieved a confirmed PSA50 response, and 35.6% had any PSA decline.
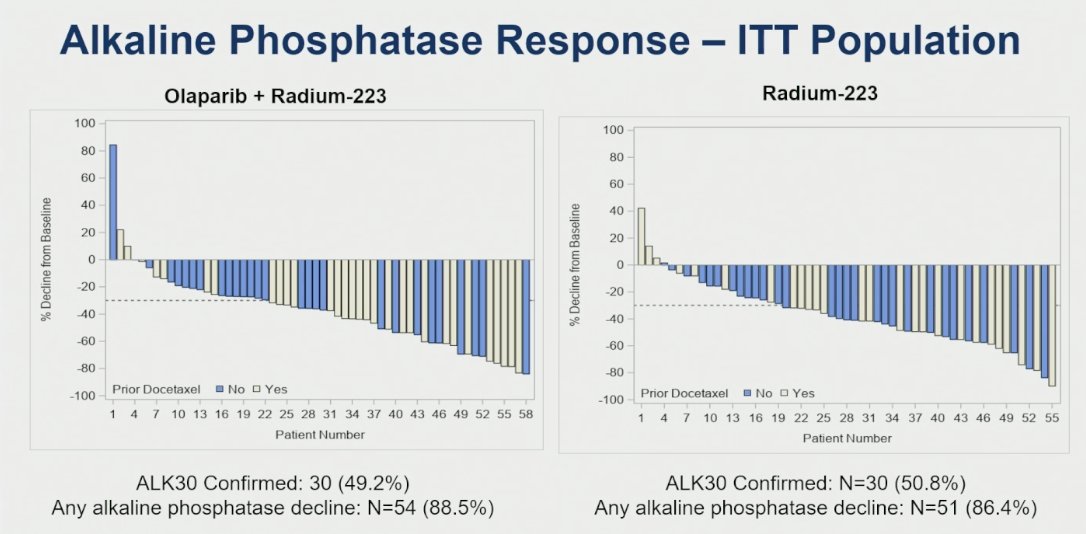
Similarly, in the combination arm, 49.2% of patients achieved a confirmed ≥30% decline in alkaline phosphatase (ALK30), and 88.5% experienced any decline. While, in the radium-223 monotherapy arm, 50.8% of patients achieved a confirmed ALK30 response, and 86.4% had any decline.
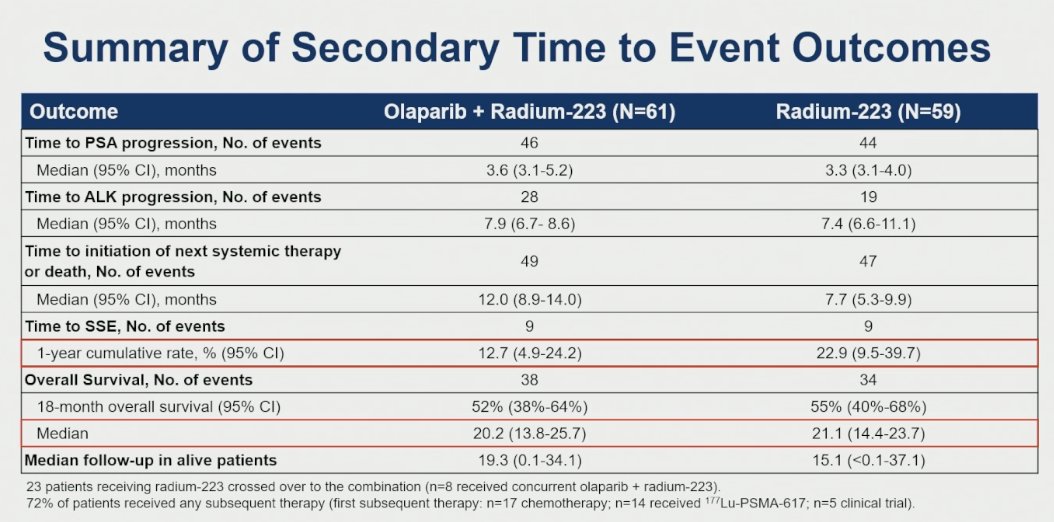
Key secondary endpoints showed no statistically significant differences between treatment arms, although a numerical improvement was observed in time to first SSE favoring the combination arm. Median overall survival was longer in the olaparib + radium-223 group (12 months) compared to the monotherapy group (7.7 months), though this may be confounded by crossover, 23 patients in the monotherapy arm received subsequent treatment with olaparib, and 8 of them received it concurrently with radium-223. Notably, 72% of patients received any subsequent therapy, including chemotherapy (n=17), 177Lu-PSMA-617 (n=14), and clinical trial participation (n=5).
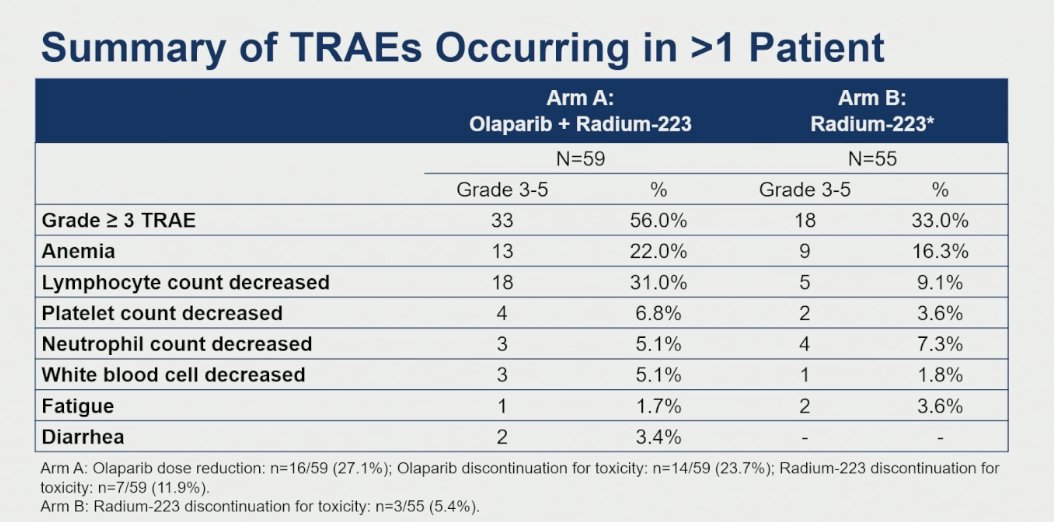
In terms of safety, the combination arm (Arm A) showed a higher rate of treatment modifications. Olaparib dose reductions occurred in 27.1% of patients (16/59), and 23.7% (14/59) discontinued olaparib due to toxicity. Additionally, 11.9% (7/59) discontinued radium-223 for toxicity. In the monotherapy arm (Arm B), 5.4% (3/55) discontinued radium-223 due to toxicity. The most notable toxicity contributing to treatment discontinuation was an increased incidence of grade ≥3 lymphopenia.
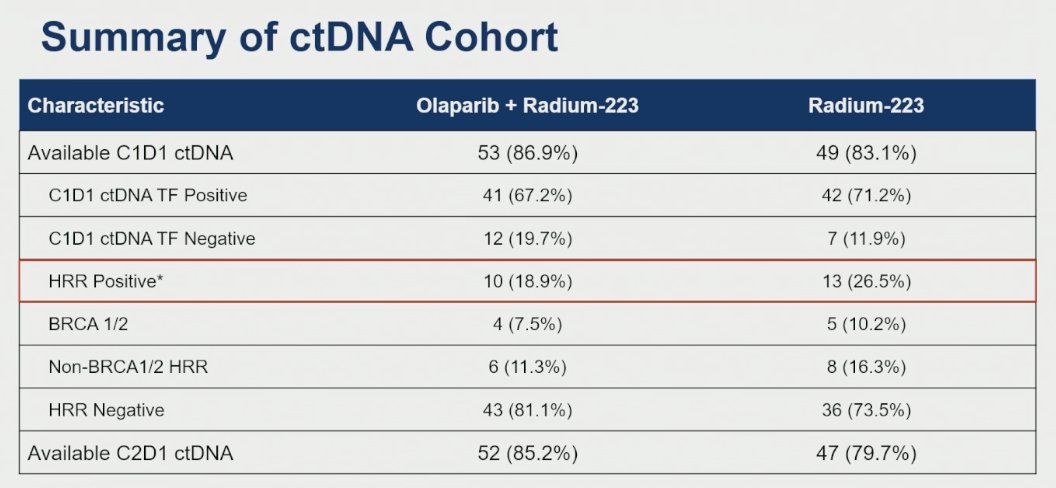
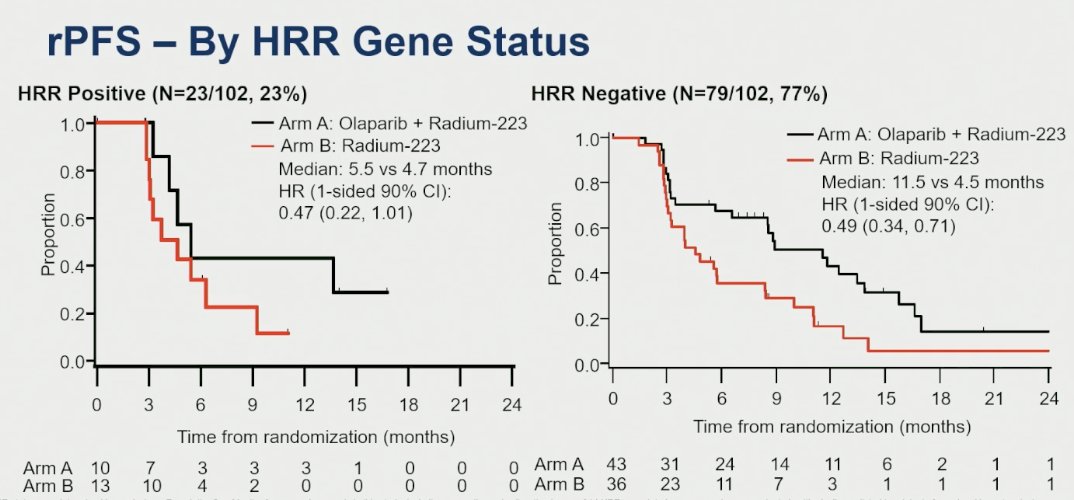
An exploratory circulating tumor DNA (ctDNA) analysis demonstrated that baseline (C1D1) ctDNA was available for 87% of patients (53/59) in the combination group and 83.1% (49/59) in the radium-223 monotherapy group. HRR gene alterations were detected in 18.9% of patients in the combination arm and 26.5% in the monotherapy arm.
In terms of rPFS by HRR gene status, the benefit of the combination was more pronounced among patients with HRR-positive tumors in the olaparib arm. Confirmatory analyses using tissue-based assays are currently ongoing.
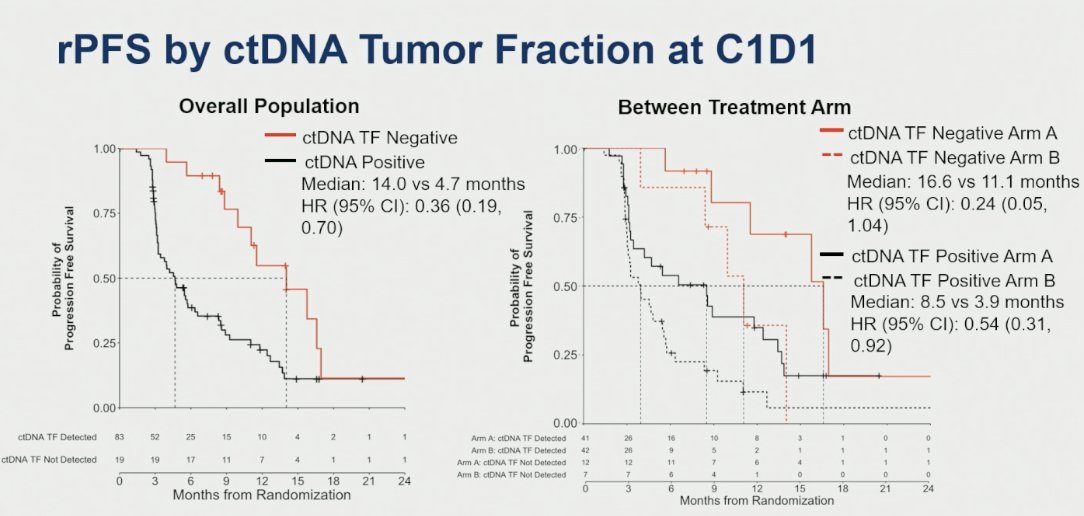
The presence of ctDNA at baseline was associated with worse outcomes, while patients with undetectable ctDNA experienced improved rPFS across the overall study population, highlighting its potential as a prognostic biomarker.
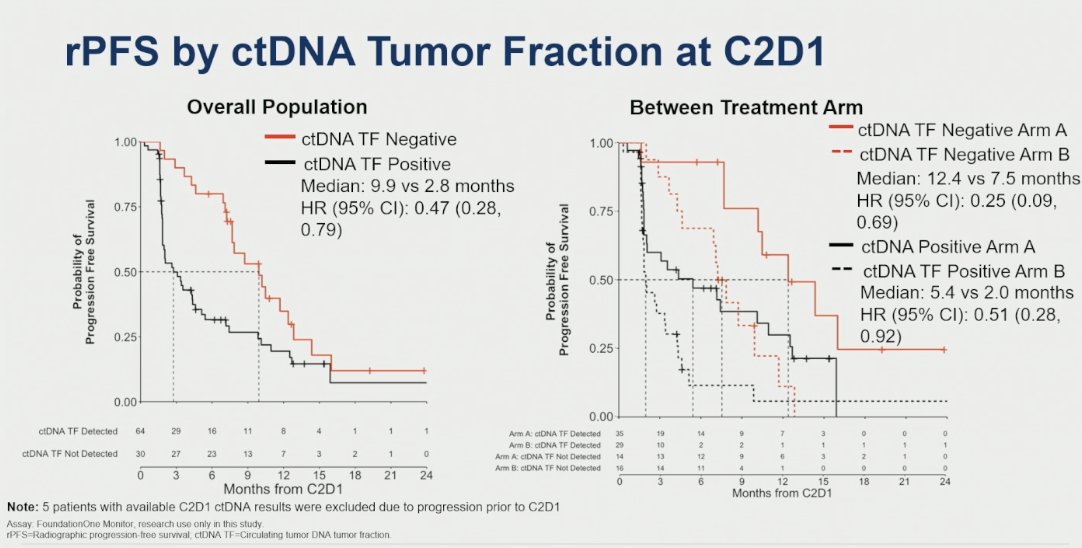
At C2D1, the presence of ctDNA was associated with lower rPFS in the overall population, suggesting that persistent ctDNA may be a marker of poor prognosis and early resistance to therapy..
Dr. McKay’s concluded her presentation with the following key takeaways from the COMRADE study:
- Reduced-dose olaparib plus radium-223 significantly improved rPFS compared to radium-223 monotherapy.
- The greatest benefit was observed in patients without prior docetaxel exposure and those with ≤20 bone metastases.
- ctDNA tumor fraction at both C1D1 and C2D1 was prognostic of rPFS across both treatment arms.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: COMRADE Trial: Radium-223 Plus Olaparib in Bone-Predominant mCRPC - Rana McKay
Reference:
- Parker C, Nilsson S, Heinrich D, Helle SI, O'Sullivan JM, Fosså SD, et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med. 2013;369(3):213–23.
- de Bono J, Mateo J, Fizazi K, Saad F, Shore N, Sandhu S, et al. Olaparib for metastatic castration-resistant prostate cancer. N Engl J Med. 2020;382(22):2091–102.