(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30 and June 3 was host to the Session New Frontiers in Prostate-Specific Membrane Antigen Radioligand Therapy. Dr. Michael Hofman presented the First-in-human results of terbium-161 161Tb-PSMA-I&T radioligand treatment in patients with metastatic castration-resistant prostate cancer (VIOLET): A single-centre, single-arm, phase I/II study.
Dr. Hofman began by emphasizing that 177Lu-PSMA is an effective treatment for metastatic castration-resistant prostate cancer (mCRPC), as it delivers targeted radiation that maximizes tumor cell killing while minimizing systemic side effects. However, even when a complete response is achieved in macroscopic disease, progression of mCRPC remains inevitable, underscoring the need for improved strategies to delay resistance and extend clinical benefit.
There are three types of radiation particles used in radioligand therapy based on their linear energy transfer (LET) and range in tissue:
- Beta particles (β⁻): These have a low LET (~0.2 keV/µm) and a relatively long tissue penetration range (1.8–10 mm). They are commonly used in treatments like ¹⁷⁷Lu-PSMA but may result in off-target effects due to their extended path, it causes single stranded DNA damage.
- Alpha particles (α): These have the highest LET (50–230 keV/µm) and a short range (40–100 nm), delivering dense, cytotoxic energy over a short distance, leading to potent cell killing with minimal off-target effects, causing double stranded DNA damage.
- Auger and conversion electrons: These exhibit a higher LET (4–26 keV/µm) and very short range (2–500 nm), enabling highly localized DNA damage with minimal collateral damage potentially advantageous for targeting energy sheltered micrometastases or single cancer cells.

Terbium-161 (¹⁶¹Tb) is a promising theranostic radionuclide that binds to PSMA receptors and emits β-particles, similar energy and half-life to ¹⁷⁷Lu, enabling effective crossfire radiation to target larger tumor volumes. In addition, ¹⁶¹Tb uniquely emits Auger electrons, which deposit high radiation energy over extremely short distances. This property may offer an advantage in eradicating micrometastatic disease, potentially outperforming ¹⁷⁷Lu in this setting.
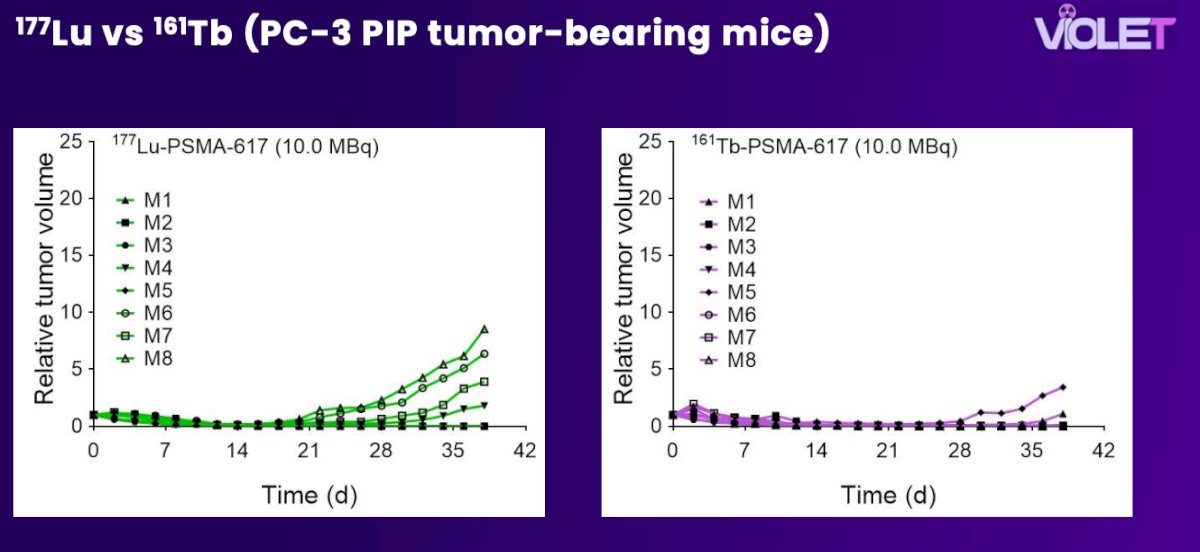
In a preclinical study, ¹⁶¹Tb -PSMA-617 demonstrated superior in vitro and in vivo efficacy in tumor-bearing mice compared to ¹⁷⁷Lu-PSMA-617. These findings support theoretical dose calculations suggesting that the additional emission of conversion and Auger electrons from ¹⁶¹Tb contributes to an enhanced therapeutic effect.1
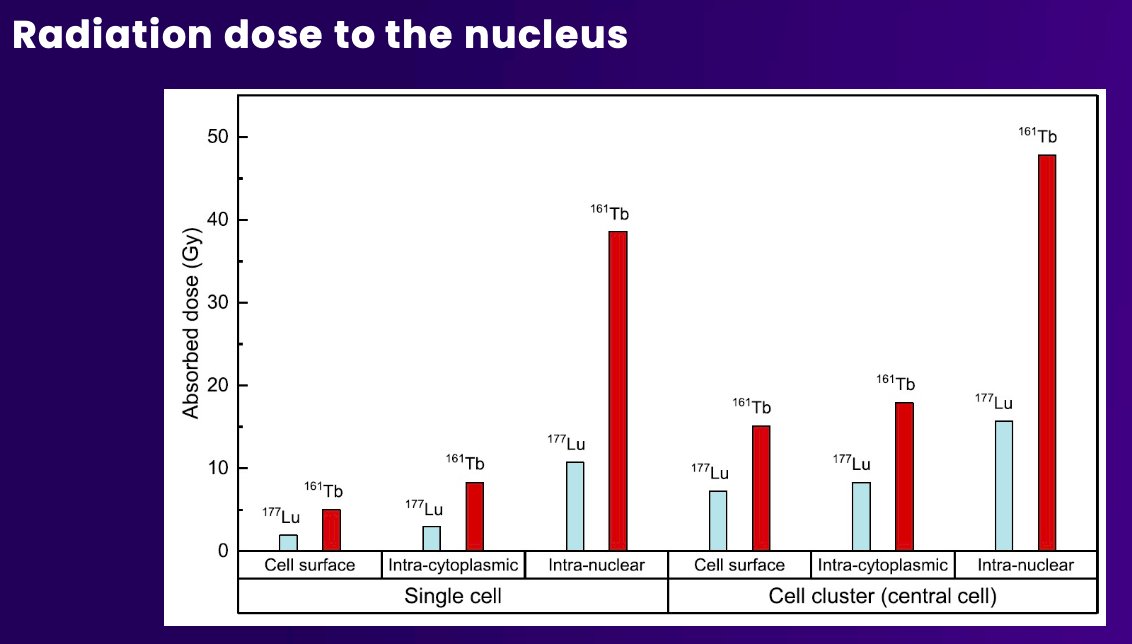
Moreover, in a dosimetric model study evaluating radiation delivery to the nucleus, ¹⁶¹Tb consistently demonstrated substantially higher absorbed doses compared to 177Lu across all intracellular localizations: 5.0 Gy vs. 1.9 Gy for cell surface distribution, 8.3 Gy vs. 3.0 Gy for intracytoplasmic distribution, and 38.6 Gy vs. 10.7 Gy for intranuclear localization.2
The VIOLET trial (NCT05521412) is a single-centre, investigator-initiated phase I/II study designed to evaluate a novel therapeutic approach in patients with mCRPC. Eligible patients must have progressed on at least one taxane (unless medically unsuitable) and an ARPI, and must demonstrate PSMA-positive disease on PET imaging (SUVmax ≥20) with no discordant FDG uptake. Participants also need to have adequate bone marrow, hepatic, and renal function, with an ECOG performance status of 0–2.
The study will enroll 30–36 patients and includes assessments such as CT, bone scan, PSMA and FDG PET, PSA, ctDNA, and patient-reported outcomes (BPI-SF, FACT-P, and FACT-RNT).
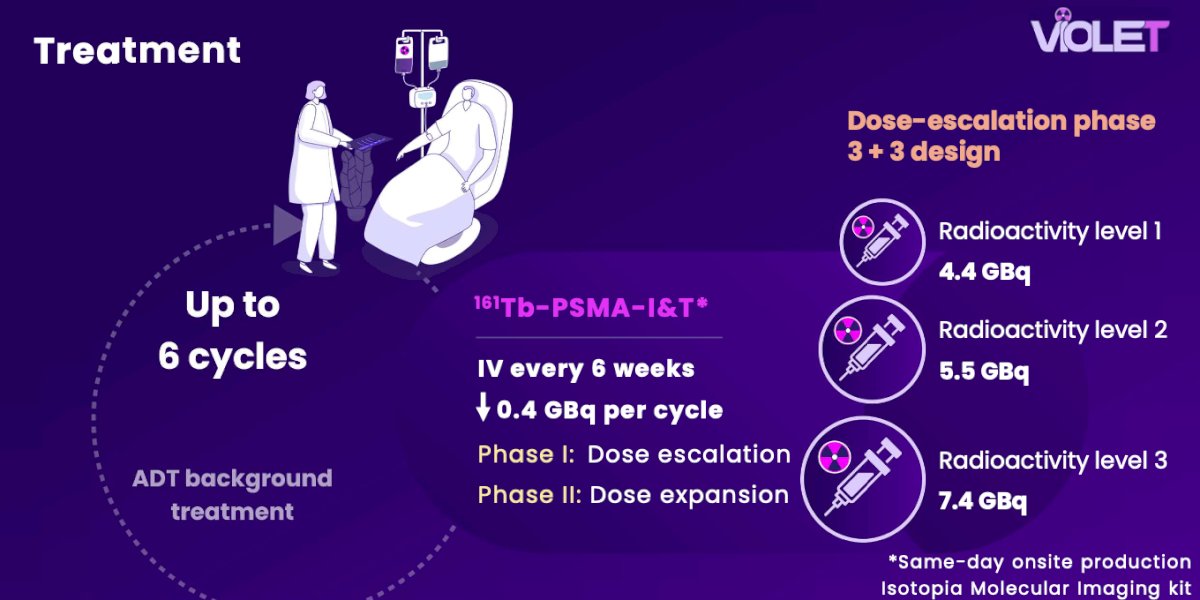
The VIOLET trial includes a dose-escalation and dose-expansion design evaluating ¹⁶¹Tb -PSMA-I&T in patients with mCRPC. A standard 3+3 dose-escalation approach is employed, with three radioactivity levels: 4.4 GBq, 5.5 GBq, and 7.4 GBq administered intravenously every six weeks, with an added 0.4 GBq per cycle. In phase I, the goal is to identify the recommended phase II dose. In phase II, patients will receive up to six cycles of therapy while continuing their background androgen deprivation therapy.
The VIOLET trial has two co-primary objectives:
- Determining the maximum tolerated radioactivity (defined as the highest dose level with fewer than one-third or two of six patients experiencing dose-limiting toxicity)
- Evaluating overall safety per CTCAE v5.0 criteria.
Secondary objectives include:
- Radiation dosimetry to normal organs and total tumor volume
- Patient-reported outcomes assessing quality of life (FACT-P) and pain (BPI-SF)
- key efficacy endpoints such as PSA response, progression-free survival (PSA, radiographic, and composite), objective response rate, and overall survival.
A total of 33 patients were assessed for eligibility in the VIOLET trial, with 3 excluded due to low PSMA uptake or FDG discordance. Impressively, enrollment was completed 8 months ahead of schedule. Among those treated, 3 patients received radioactivity level 1, 3 received level 2, and 6 received level 3. An additional 18 patients were treated in the dose expansion cohort. Overall, 21 patients (70%) completed all 6 treatment cycles, with a median total administered radioactivity of 38.0 GBq (IQR 21.1–38.5).

The median age of patients in the VIOLET trial was 69 years, with a median time since prostate cancer diagnosis of 6.5 years. Notably, 50% of participants had de novo metastatic hormone-sensitive disease at initial diagnosis. All patients had received a second-generation ARPI, and 67% had also received prior chemotherapy.

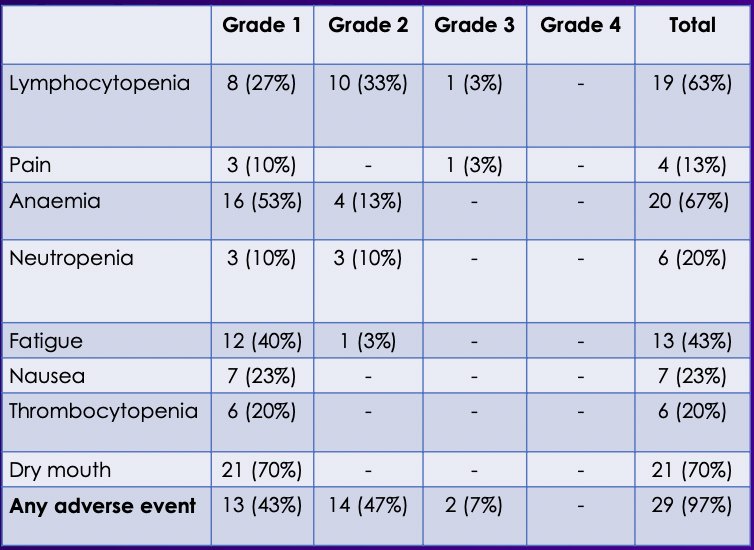
Dr. Hofman reported that no dose-limiting toxicities were observed. Treatment-related Grade 3/4 adverse events occurred in only 2 patients (7%), with no instances of radioactivity dose reduction, no cycle delays, and no treatment-related deaths.
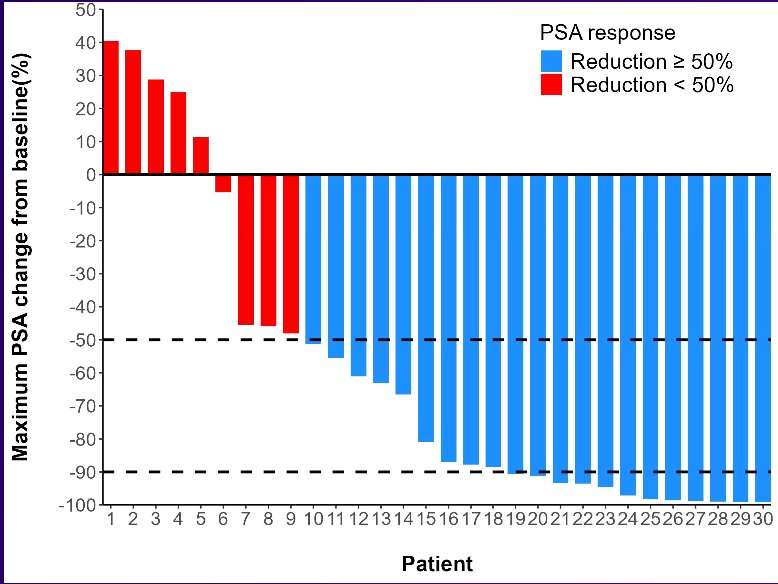
The PSA50 response rate in the VIOLET trial was 70% (95% CI, 51–85), while the PSA90 response rate was 40% (95% CI, 23–59) as shown in the waterfall plot below. PSA responses is a good biomarker for RLT.
The median PSA progression-free survival (PSA-PFS) was 9 months (95% CI, 5.7–15.1), while the median radiographic progression-free survival (rPFS) was 11 months (95% CI, 6.6–11.7).

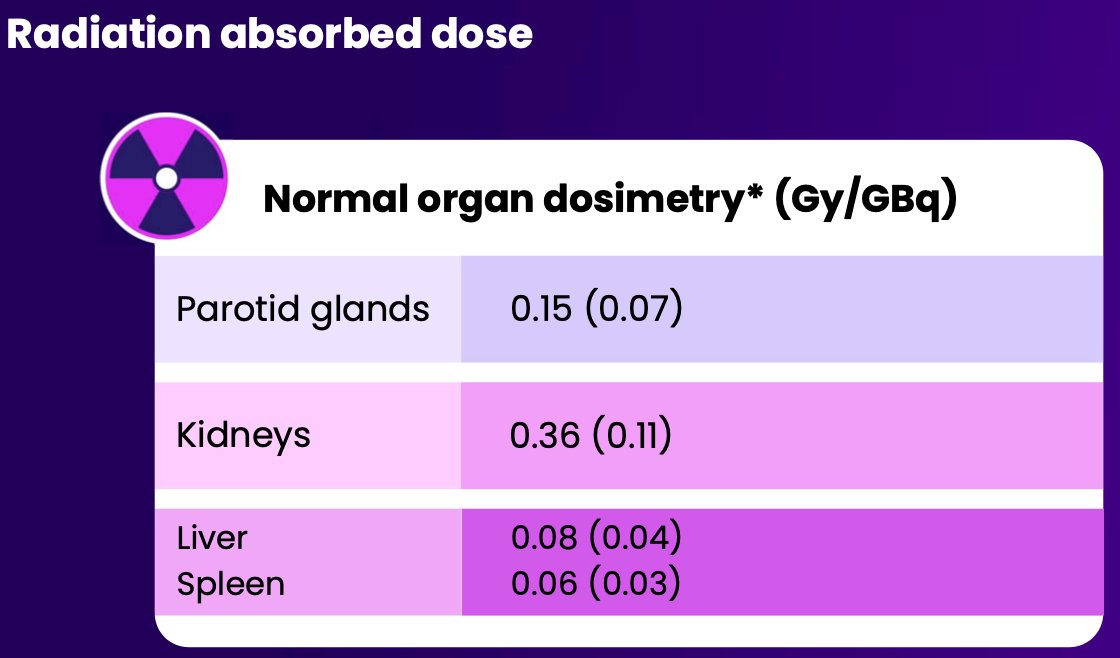
Organ dosimetry analysis showed that radiation absorbed doses to normal tissues remained within acceptable safety margins. The mean absorbed doses (in Gy/GBq) were 0.15 for the parotid glands, 0.36 for the kidneys, 0.08 for the liver, and 0.06 for the spleen which are the potential dose-limiting organs.
Dr. Hofman highlighted several key aspects of the VIOLET trial. Among the major strengths were the fact that this was a first-in-human study, recruitment was completed ahead of schedule, and the logistics were similar to those already established for 177Lu-PSMA.
Limitations included its single-cohort design, limited dosimetry data, especially regarding blood and Auger electrons, and the fact that dosing only reached up to 7.4 GBq. It is hard to say with these data that this is superior to 177Lu-PSMA, and comparative studies are needed.
Looking ahead, a 9.5 GBq cohort is currently recruiting, with future directions including larger phase III trials and exploration of earlier use, as we know 177Lu-PSMA performs better when introduced earlier. A summary slide of the trial is shown below.

Dr. Hofman concluded with the following key takeaway points:
- This study represents the first-in-human use of Terbium-161 across all cancer types.
- In patients with progressive mCRPC, Terbium-161 PSMA-I&T demonstrated a favorable safety profile, even at doses up to 7.4 GBq.: Only 2 patients (7%) experienced treatment-related grade 3–4 adverse events. No treatment-related dose reductions, delays, or deaths were reported.
- Early signals of efficacy were encouraging:
- PSA ≥90% decline was observed in 40% of patients (95% CI, 23–59).
- Median radiographic progression-free survival was 11.1 months (95% CI, 6.6–11.7)
Presented by: Michael Hofman, MBBS, FRACP, FAANMS, FICIS, GAICD, Prostate Cancer Theranostics and Imaging Centre of Excellence, Peter MacCallum Cancer Center, Melbourne, Australia
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: Terbium-161 vs Lutetium-177: Comparing Next-Gen Radioligands for Prostate Cancer - Michael Hofman
References:
- Müller C, Umbricht CA, Gracheva N, Tschan VJ, Pellegrini G, Bernhardt P, Zeevaart JR, Köster U, Schibli R, van der Meulen NP. Terbium-161 for PSMA-targeted radionuclide therapy of prostate cancer. Eur J Nucl Med Mol Imaging. 2019 Aug;46(9):1919-1930. doi: 10.1007/s00259-019-04345-0. Epub 2019 May 27. PMID: 31134301; PMCID: PMC6820371.
- Alcocer-Ávila ME, Ferreira A, Quinto MA, Morgat C, Hindié E, Champion C. Radiation doses from 161Tb and 177Lu in single tumour cells and micrometastases. EJNMMI Phys. 2020 May 19;7(1):33. doi: 10.1186/s40658-020-00301-2. PMID: 32430671; PMCID: PMC7237560.