(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30 and June 3 was host to the Poster Session: Genitourinary Cancer - Prostate, Testicular, and Penile Cancer. Dr. Nobuaki Matsubara presented Poster 5046: Safety and pharmacokinetics of mevrometostat in combination with enzalutamide in patients with metastatic castration-resistant prostate cancer (mCRPC).
Enhancer of zeste homolog 2 (EZH2) is overexpressed in castration-resistant prostate cancer (CRPC) and contributes to disease progression by repressing tumor suppressor genes, co-activating androgen receptor (AR)-mediated transcriptional programs, and promoting cell cycle deregulation.1,2 Mevrometostat is a potent and selective small molecule inhibitor of EZH2. It is hypothesized that combining an EZH2 inhibitor with an AR pathway inhibitor (ARPI) may enhance clinical response to ARPI therapy and delay or prevent the emergence of antiandrogen resistance.
In the randomized dose-expansion phase of a Phase 1 study (NCT03460977), the combination of mevrometostat (1250 mg twice daily on an empty stomach) and enzalutamide (160 mg once daily) demonstrated improved clinical outcomes compared to enzalutamide alone in patients with mCRPC, with a manageable safety profile.3
Dr Matsubara presented updated safety and pharmacokinetic data for mevrometostat at a lower dose of 875 mg administered with food in combination with enzalutamide. This open-label phase 1 trial evaluated the safety and pharmacokinetics of a food-effect cohort in patients with mCRPC.
This open-label, dose-escalation and dose-expansion study enrolled patients aged ≥18 years with mCRPC who had previously received abiraterone and/or enzalutamide and had evidence of progression according to modified Prostate Cancer Working Group 3 (PCWG3) criteria. In the randomized dose-expansion phase, patients were assigned 1:1 (unblinded) to receive either mevrometostat 1250 mg BID on an empty stomach in combination with enzalutamide 160 mg QD, or enzalutamide alone, administered from Day 1 to Day 21 in each cycle.
Observations from the earlier, non-randomized part of the study suggested that administration of mevrometostat with food could improve the safety profile compared to the 1250 mg BID fasting dose. The current analysis focused on patients who received mevrometostat 875 mg BID with food in combination with enzalutamide 160 mg QD and androgen deprivation therapy. The primary endpoint was the safety of this dosing strategy, while a secondary endpoint assessed the effect of food on pharmacokinetics. Outcomes were compared with those from the dose-expansion cohort who had received mevrometostat 1250 mg BID on an empty stomach with enzalutamide.
As of February 28, 2025, a total of 29 patients received mevrometostat 875 mg BID with food in combination with enzalutamide. The median duration of treatment was 8.0 months (range: 4.5–10.4). The median age of patients in this cohort was 73 years (range: 55–86). Baseline demographics and disease characteristics were generally comparable between patients receiving mevrometostat 875 mg BID with food and those in the dose-expansion cohort who received 1250 mg BID on an empty stomach alongside enzalutamide. Full baseline characteristics are detailed in the table below.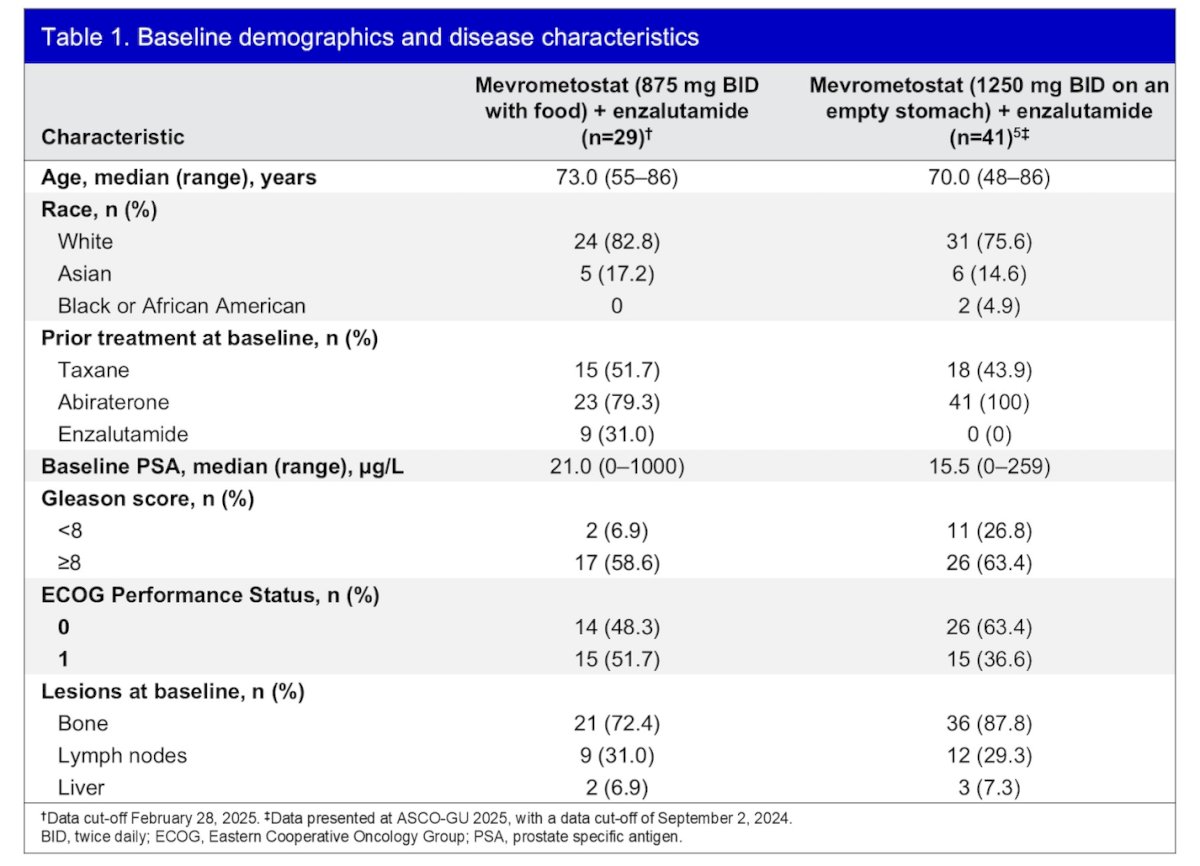
All 29 patients (100%) who received mevrometostat 875 mg BID with food in combination with enzalutamide experienced at least one treatment-emergent adverse event (TEAE). The most common all-cause TEAEs were diarrhea (n=13; 44.8%), thrombocytopenia (n=13; 44.8%), and dysgeusia (n=12; 41.4%). Notably, no grade ≥3 cases of diarrhea were reported in this cohort.
Adverse events leading to dose reductions of mevrometostat occurred in 5 patients (17.2%). These included two cases of dysgeusia and one case each of asthenic conditions, diarrhea, dyspepsia, prolonged QT on ECG, fall, and thrombocytopenia. One patient experienced a fatal (grade 5) event of osteonecrosis of the jaw, which was present at baseline and deemed unrelated to mevrometostat. This was the only TEAE that led to treatment discontinuation. Full safety data are summarized in the table below.
Gastrointestinal TEAEs were notably reduced in patients receiving mevrometostat 875 mg BID with food compared to those receiving 1250 mg BID on an empty stomach, as illustrated in the figure below. This suggests improved gastrointestinal tolerability with the food-based dosing strategy.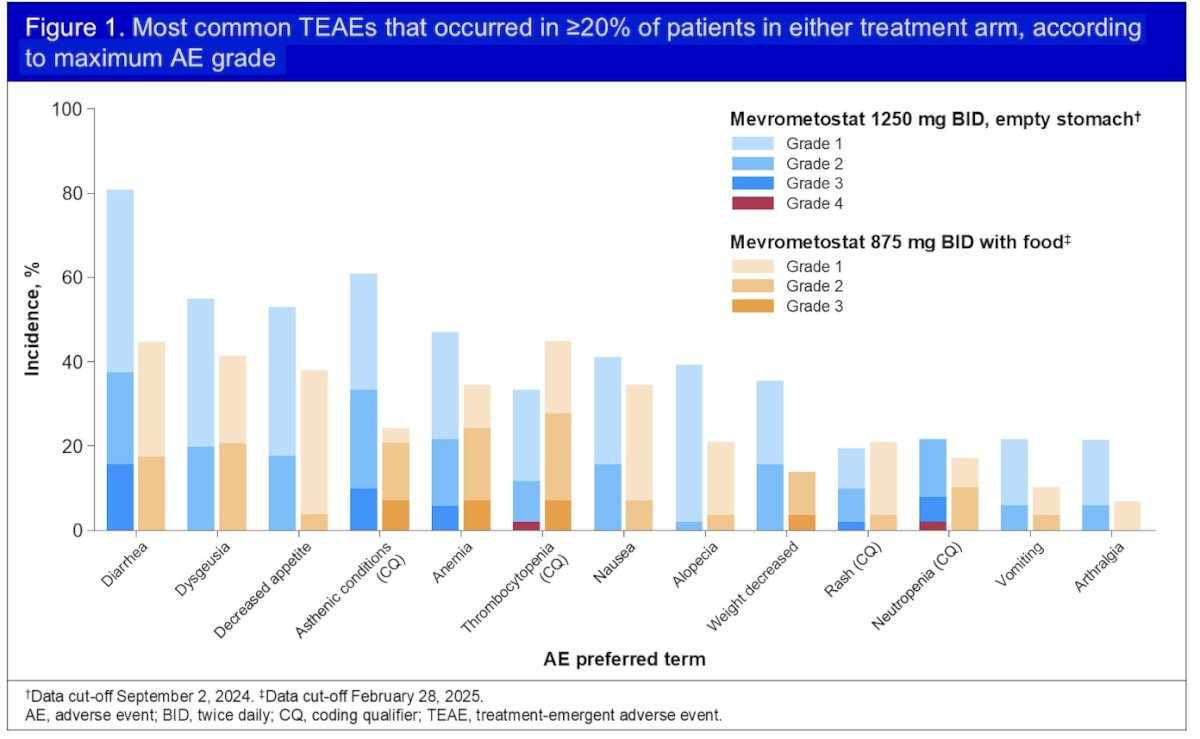
Pharmacokinetic analysis showed similar plasma exposures between patients receiving mevrometostat 875 mg with food (n=12) and those who received 1250 mg on an empty stomach (n=51). Geometric mean (coefficient of variation) for AUCtau (h*ng/mL) was 8,984 (48%) for the 875 mg cohort and 8690 (54%) for the 1250 mg cohort. Corresponding Cmax (ng/mL) values were 1868 (85%) and 2371 (54%), respectively, as illustrated in the graphics below.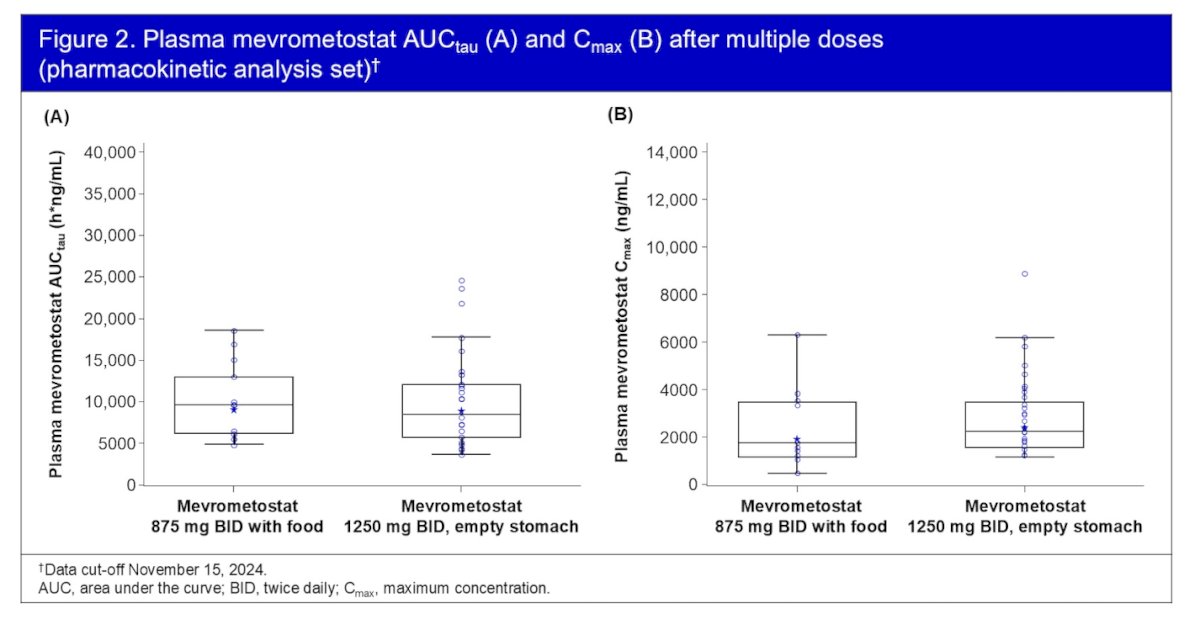
Dr. Matsubara concluded with the following key points:
- In patients with mCRPC, the combination of mevrometostat 875 mg BID with food and enzalutamide demonstrated an improved safety profile, particularly in terms of gastrointestinal tolerability, compared to the 1250 mg BID fasting regimen.
- Despite the lower dose and food-based administration, plasma exposures with mevrometostat 875 mg BID were similar to those observed with the 1250 mg BID fasting regimen.
- Based on these favorable safety and pharmacokinetic findings from the phase 1 trial, mevrometostat 875 mg BID with food was selected as the recommended dose for the phase 3 clinical development program in combination with enzalutamide.
Pivotal phase 3 trials using this regimen are now underway in multiple patient populations:
- MEVPRO-1 (NCT06551324): patients with mCRPC previously treated with abiraterone.
- MEVPRO-2 (NCT06629779): patients with mCRPC who are ARPI-naïve.
- MEVPRO-3: patients with mCSPC who are ARPI-naïve.
Presented by: Nobuaki Matsubara, MD, Department of Medical Oncology, National Cancer Center Hospital East. Chiba, Japan
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:
- Beltran H, Hruszkewycz A, Scher HI, Hildesheim J, Isaacs J, Yu EY, et al. The role of lineage plasticity in prostate cancer therapy resistance. Clin Cancer Res. 2019;25(23):6916–24.
- Berger A, Brady NJ, Bareja R, Robinson B, Sundi D, Rickman DS, et al. Lineage plasticity and therapeutic resistance in prostate cancer. J Clin Invest. 2019;129(9):3924–40.
- Schweizer MC, Alumkal JJ, Mehra R, et al. Phase 1/1b study of mevrometostat (EZH2i) plus enzalutamide in metastatic castration-resistant prostate cancer (mCRPC). J Clin Oncol. 2025;43(5_suppl):LBA138.