(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to the Oral Abstract Session: Genitourinary Cancer—Prostate, Testicular, and Penile. Dr. Nicholas James presented a study assessing a multimodal artificial intelligence (MMAI) model to identify benefit from 2nd-generation androgen receptor pathway inhibitors (ARPI) in high-risk non-metastatic prostate cancer patients from STAMPEDE.
Dr. James highlighted the importance of addressing ongoing uncertainty in treatment intensification for clinically high-risk M0 prostate cancer. While the current standard of care, based on the STAMPEDE platform study, includes two years of androgen deprivation therapy (ADT) combined with abiraterone1 and radiotherapy. However, this approach may overtreat a subset of patients. (1) Dr James posed a critical question: can a digital pathology-based AI risk score be used to guide the selective use of abiraterone, enabling more personalized treatment intensification strategies for patients with high-risk localized prostate cancer? This approach could help balance efficacy with toxicity by tailoring therapy to individual tumor biology.
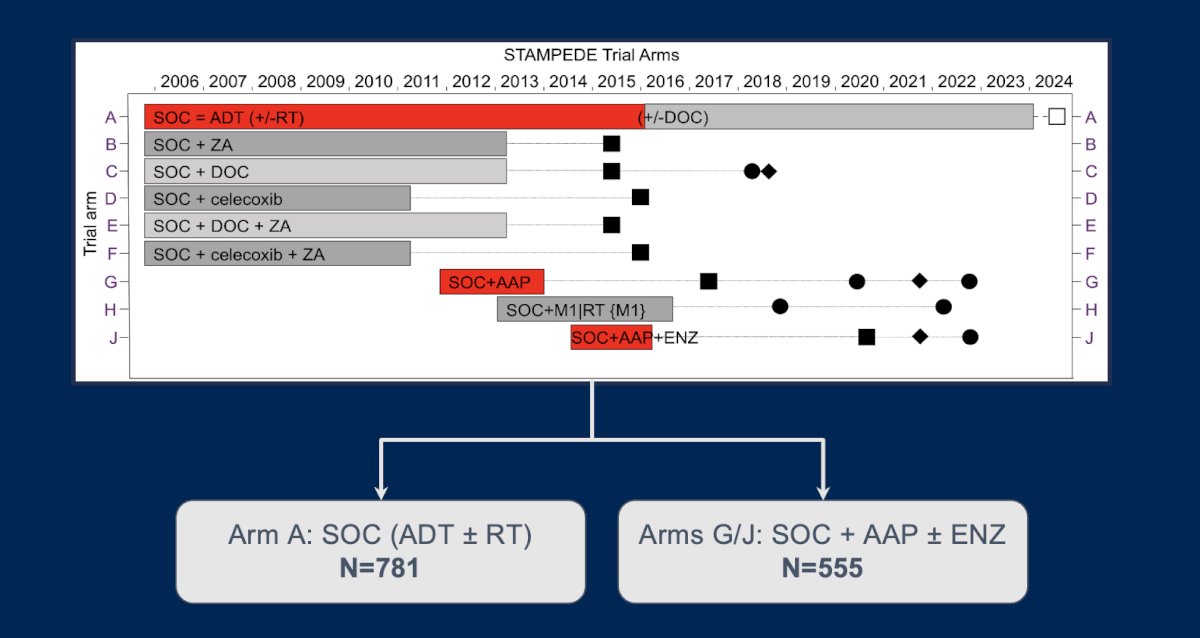
This was a substudy embedded within the STAMPEDE platform, designed to evaluate the feasibility of digital pathology AI-guided treatment selection for high-risk localized prostate cancer. The objective was to explore whether a prognostic AI-derived pathology score could identify a subgroup of clinically high-risk patients more likely to benefit from the addition of abiraterone (AAP) to standard of care (SOC) therapy. Eligible patients included those with node-positive (N1) disease or node-negative (N0) disease with at least two high-risk features: T3/T4 staging, Gleason score 8–10, or PSA ≥40 ng/mL. All participants had consented to biomarker development studies and had both digital pathology slides and clinical data available for analysis.
The primary endpoint was metastasis-free survival (MFS), defined as the earlier occurrence of distant metastasis or death from any cause. A secondary endpoint was prostate cancer-specific mortality (PCSM). The analysis was conducted with a median follow-up of six years. A total of 781 patients in Arm A (SOC (ADT ± RT)) and 555 in Arms G/J: SOC + AAP ± Enzalutamide) were included in this analysis.
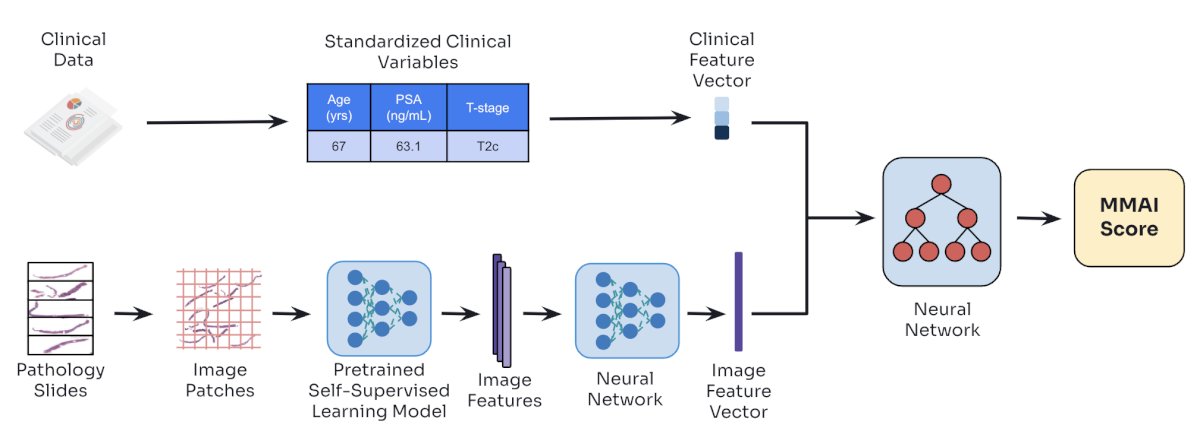
Prognostic MMAI (multi-modal artificial intelligence) scores were developed using H&E-stained biopsy whole slide images alongside clinical variables such as age, PSA, and T-stage.
These scores were then evaluated for their association with clinical outcomes using Cox regression for metastasis-free survival (MFS) and Fine-Gray competing risks models for prostate cancer-specific mortality (PCSM) and distant metastasis (DM), accounting for death as a competing event. To assess whether the benefit of adding abiraterone (AAP) to standard of care (SOC) varied by risk group, treatment-by-MMAI interaction tests were also conducted.
Dr. James reported that the MMAI score is prognostic even within clinically high-risk prostate cancer populations. Applying established clinical prognostic cut-offs, 89% (N=1,189) of M0 patients in the cohort were classified as MMAI high-risk, demonstrating the model's ability to further stratify risk within an already high-risk population.

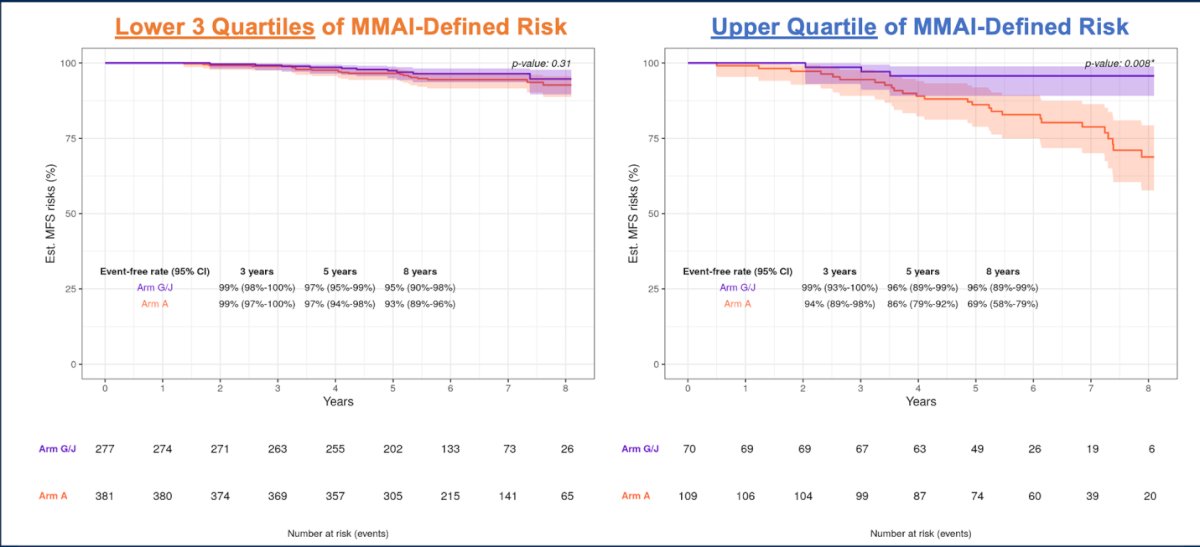
Moreover, an alternative MMAI cut-point was identified through an exploratory grid search using prognostic risk scores, aiming to optimize treatment benefit from abiraterone. This analysis stratified patients into two groups: the upper quartile versus the lower three quartiles of the MMAI score distribution. This data-driven threshold demonstrated significant discrimination in metastasis-free survival (MFS), with patients in the upper quartile showing a greater benefit from the addition of abiraterone.
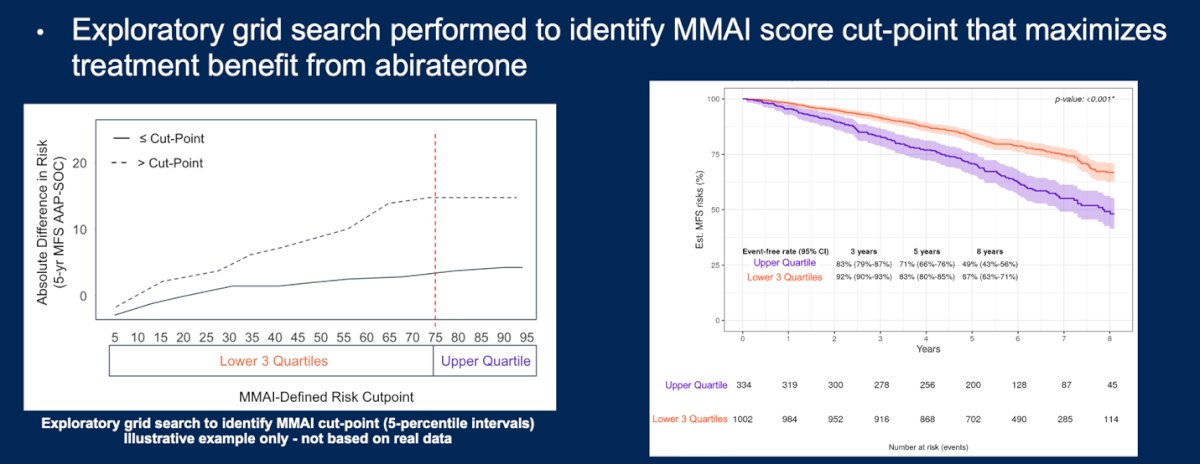
M0 patients with MMAI scores in the upper quartile of risk were significantly more likely to benefit from the addition of abiraterone, with a hazard ratio for metastasis-free survival (MFS) of 0.48 (95% CI: 0.33–0.71; p < 0.001). Notably, the interaction between MMAI risk score and treatment effect was statistically significant (interaction p = 0.01), supporting the potential role of MMAI as a predictive biomarker to guide selective treatment intensification with abiraterone in high-risk prostate cancer.

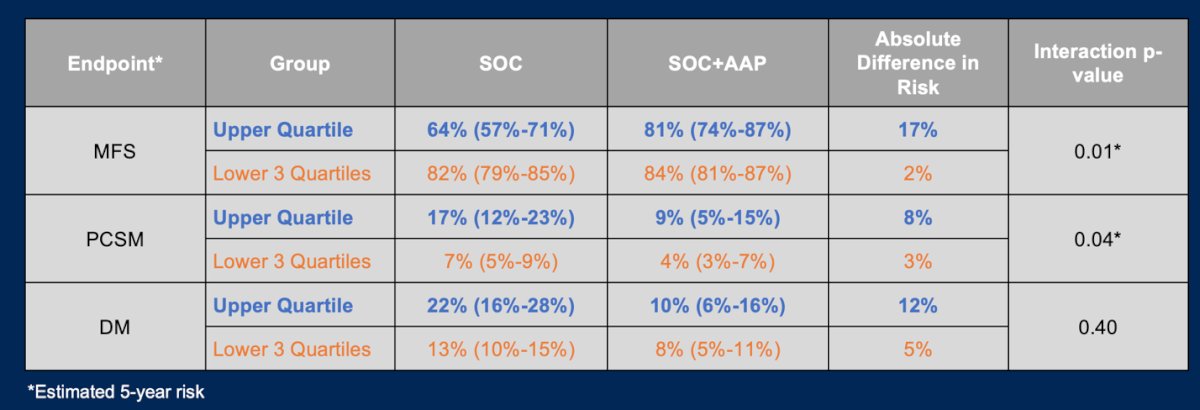
Moreover, in terms of MFS, distant metastasis (DM), and prostate cancer-specific mortality (PCSM), patients in the upper quartile of MMAI-defined risk derived the greatest benefit from the addition of abiraterone. The treatment-by-MMAI interaction p-value was significant for both MFS and PCSM, indicating a meaningful predictive effect. Notably, the absolute risk reduction in MFS with abiraterone was 17% in the upper quartile compared to just 2% in the lower three quartiles, highlighting the potential of MMAI scores to guide more personalized treatment intensification.
The differential treatment benefit from abiraterone remained evident even within the more clinically homogeneous subgroup of N0M0 patients. Those with MMAI scores in the upper quartile of risk were significantly more likely to benefit from the addition of abiraterone, reinforcing the score’s predictive value. In this subgroup, the MMAI-treatment interaction effect remained statistically significant (p = 0.02)
Dr. James acknowledged several limitations of the study, including the retrospective derivation of the MMAI score cut-point to optimize treatment effect differentiation. He emphasized that further validation is challenging due to the lack of comparable randomized trials in this specific setting. Looking ahead, he suggested that future studies should investigate the predictive utility of the MMAI score in broader contexts, such as with other androgen receptor pathway inhibitors like apalutamide or enzalutamide, and in additional abiraterone-treated populations, including patients with metastatic prostate cancer.
Dr. James concluded his presentation with the following key remarks:
- A prognostic digital pathology-based AI model may help guide the selective use of abiraterone in clinically high-risk prostate cancer patients.
- MMAI can identify non-metastatic high-risk patients who derive the greatest benefit from adding abiraterone to standard of care.
- This approach may support more personalized treatment strategies and help minimize overtreatment.
- The findings support the integration of digital pathology biomarkers into clinical decision-making in prostate cancer.
Presented by: Nicholas David James, PhD, FRCP, MBBS, The Royal Marsden NHS Foundation Trust and The Institute of Cancer Research. London, U.K.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: AI Model Identifies STAMPEDE Patients Needing Treatment Intensification - Nicholas James
Reference: