(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to the Oral Abstract Session: Genitourinary Cancer—Prostate, Testicular, and Penile. Dr. Joaquin Mateo delivered a lecture titled: Parp Up the Volume!: Combination Strategies in Advanced Prostate Cancer.
Dr Mateo began by emphasizing how the clinical development of PARP inhibitors (PARPi) has led to their regulatory approval for patients harboring homologous recombination repair (HRR) mutations. He noted the importance of the ongoing synergy between clinical and laboratory research, which continues to refine our understanding of why these therapies are effective in some patients but not in others.
Dr Mateo discussed three key trials presented at this session exploring PARP inhibitor combinations in advanced prostate cancer, each targeting a distinct therapeutic strategy:
- AMPLITUDE (Attard et al.) – A phase 3 trial evaluating niraparib + abiraterone acetate/prednisone (AAP) in mCSPC patients with HRR gene alterations, aiming to prevent or delay resistance through dual pathway blockade.
- COMRADE (McKay et al.) – A randomized phase 2 study assessing olaparib + radium-223 vs radium-223 alone in mCRPC with bone metastases, leveraging the synergy of DNA damage induction and impaired repair.
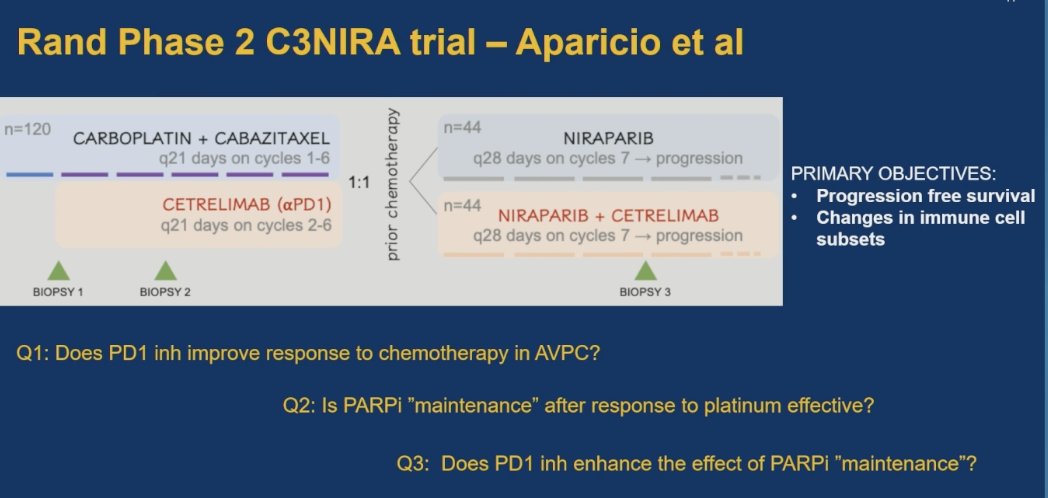
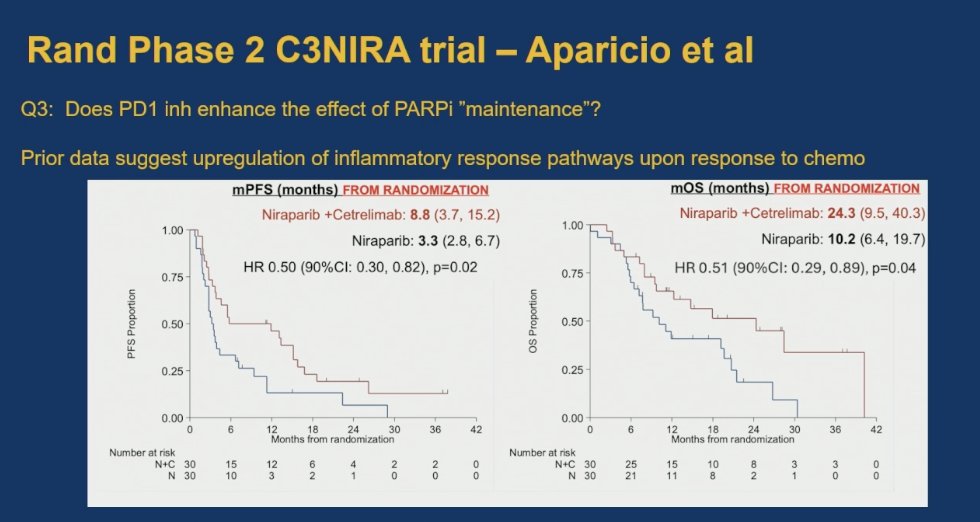
- C3NIRA (Aparicio et al.) – A phase 2 trial combining platinum-taxane chemotherapy and anti-PD-1 immunotherapy (cetrelimab) induction followed by niraparib ± cetrelimab maintenance in AVPC, exploring immune-modulatory adaptation.
Dr. Mateo emphasized that the overarching message from these three abstracts is that smart, biology-driven science must guide the design and development of combination therapies. By aligning mechanistic rationale with clinical strategy, we move closer to truly helping patients and meaningfully improving outcomes in advanced prostate cancer.
AMPLITUDE TrialThe Phase 3 AMPLITUDE trial randomized 696 mCSPC patients with HRR gene alterations to receive niraparib + AAP + ADT vs placebo + AAP + ADT. Patients were stratified by HRR mutation type, prior docetaxel use, and disease volume. The primary endpoint was rPFS; secondary endpoints included OS, time to symptomatic progression, and safety.

The AMPLITUDE trial builds on prior experiences from PROPEL, MAGNITUDE, and TALAPRO-2, which evaluated PARPi combinations in mCRPC.1-3 In MAGNITUDE, the same formulation of niraparib plus AAP used in AMPLITUDE showed benefit in HRR-mutated mCRPC, particularly in BRCA1/2-altered tumors. The non-HRR cohort was closed early due to lack of efficacy, and while rPFS improved in HRR-mutated patients, no significant OS benefit was observed.1
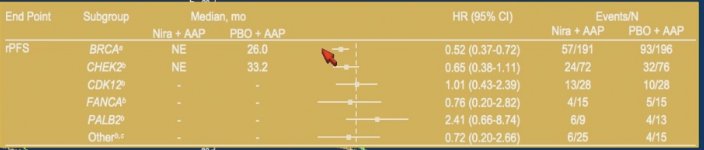
In the AMPLITUDE trial, patients with BRCA mutations experienced clear improvements in rPFS with the addition of niraparib to abiraterone and prednisone. While the HRRm group overall showed benefit, it’s important to note that BRCA-mutated patients were included within this cohort and appeared to drive much of the observed effect. Overall survival data remain immature at this point. Notably, up to 36% of patients in the placebo arm later received PARP inhibitors, which may impact long-term survival comparisons.

Dr. Mateo emphasized that patients with BRCA mutations undoubtedly derived the greatest benefit from the combination of niraparib and abiraterone, reinforcing the importance of biomarker-driven treatment selection in advanced prostate cancer.
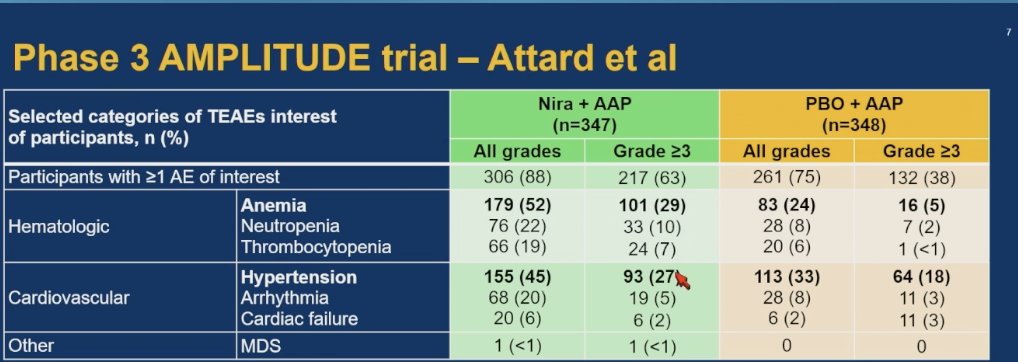
In terms of safety, the profile was consistent with previous studies. Grade ≥3 anemia occurred in 29% of patients receiving niraparib plus abiraterone compared to 5% in the placebo arm. There was also a slightly higher incidence of hypertension with the combination 45% versus 33% for all-grade events, respectively.
Dr Mateo concluded his critical appraisal of the AMPLITUDE study with the following key points:
- The AMPLITUDE study demonstrated that combining niraparib with abiraterone (PARPi + ARPI) improves outcomes in patients with mCSPC, particularly those with BRCA mutations.
- While previous evidence supported the efficacy of this combination, these results raise the question of optimal timing, suggesting a potential benefit to earlier use in treatment.
- Based on these findings, early access to PARP inhibitors is reasonable, especially for patients with BRCA mutations.
- Genomic profiling should be embedded in the diagnostic evaluation of metastatic prostate cancer.
- Broader implementation of diagnostic genomic profiling would support more equitable, efficient, and personalized care.
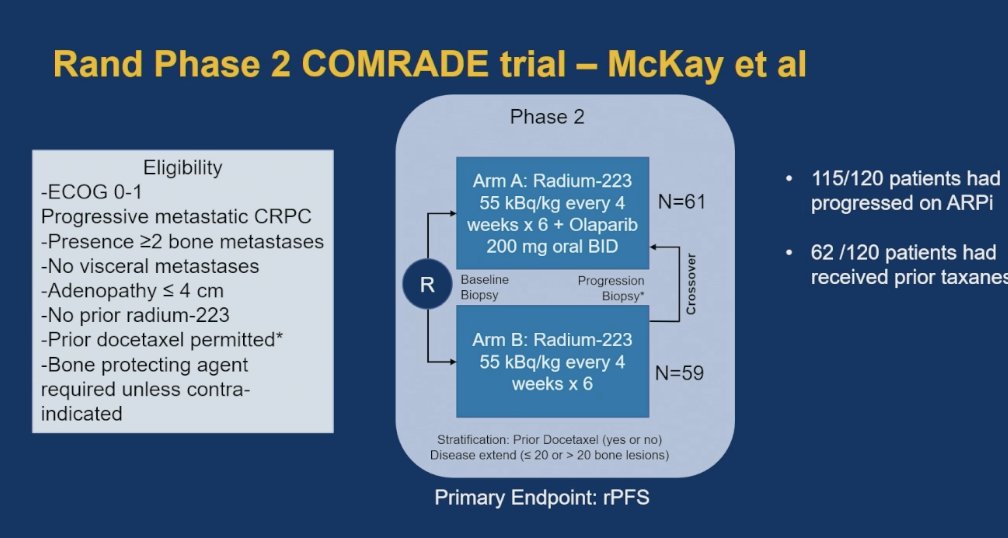
In the Phase II COMRADE study, patients with mCRPC were randomized 1:1 to receive olaparib plus radium-223 or radium-223 alone. Notably, 115 of 120 patients had progressed on prior ARPI therapy, and 62 of 120 had received prior taxane chemotherapy. The primary endpoint was rPFS with stratification by prior docetaxel use. Crossover to the combination arm was allowed for patients initially assigned to radium-223 monotherapy. The study design is outlined below.
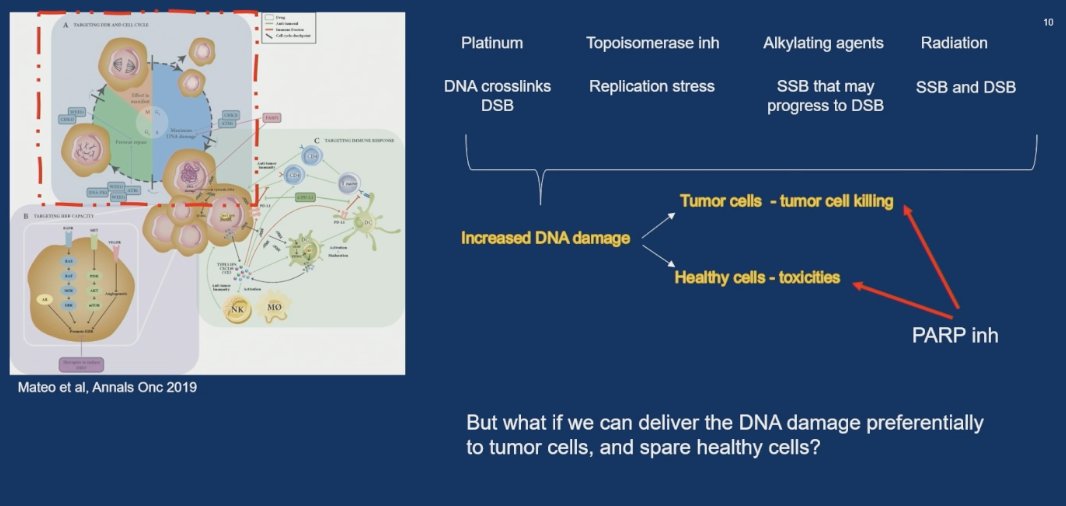
Combining PARP inhibitors with DNA-damaging agents such as radium-223 increases DNA damage in tumor cells, enhancing tumor cell killing through synthetic lethality. The rationale behind this approach lies in leveraging the synergy between PARPi and DNA-damaging therapies.
In the COMRADE trial, the combination of olaparib and radium-223 resulted in improved rPFS compared to radium-223 alone (median rPFS: 8.9 vs 4.7 months). The rates of anemia and thrombocytopenia were comparable to those observed with olaparib monotherapy.
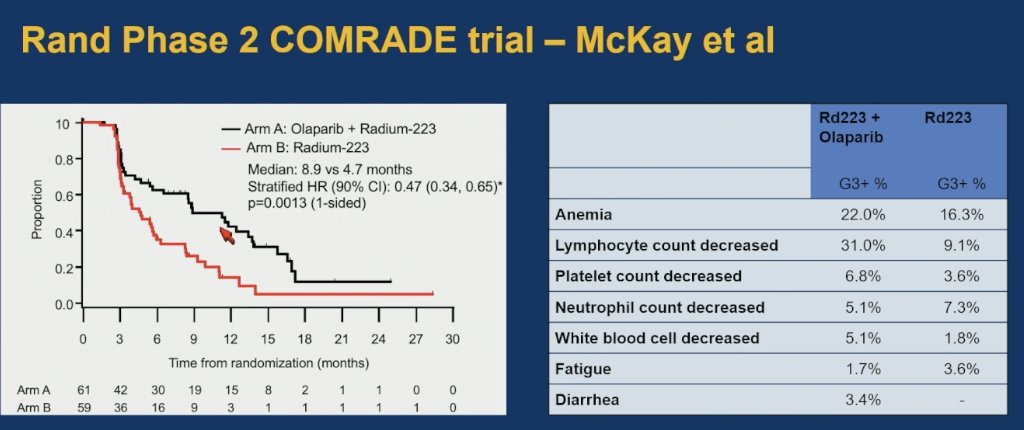
Dr. Mateo highlighted a similar hazard ratio for rPFS was observed in patients with and without homologous recombination repair (HRR) mutations, although interpretation is limited by the small number of HRR-positive patients. The combination therapy was associated with a longer time to next therapy (12.0 vs 7.7 months) and a lower rate of symptomatic skeletal events (SSEs) at one year (13% vs 23%), aligning with the overall improvement in rPFS.
The benefit appeared to be more pronounced in patients with fewer than 20 bone metastases; however, this was a subgroup analysis and should be interpreted with caution, especially regarding tolerability. Notably, PSA50 (15% vs 15%) and alkaline phosphatase (ALK30) response rates (49% vs 51%) were similar between arms, though responders in the combination arm tended to achieve deeper responses. The Median OS and 18-month landmark OS were identical between groups, raising questions about long-term survival implications.
Dr. Mateo emphasized that while the combination does not appear to induce more responses, it may lead to deeper responses in those who do benefit.
Dr. Mateo highlighted several key findings from the COMRADE trial:
- Adding olaparib to radium-223 improves rPFS
- Confirms the feasibility and potential efficacy of combining PARP inhibition with "on-tumor" DNA damage induction.
- Supports future combination strategies involving other radiopharmaceuticals and antibody-drug conjugates (ADCs).
- An increasing number of radiopharmaceutical-based combinations are expected to emerge.
- A deeper understanding of the underlying biological interactions will be essential to optimize the timing and use of PARP inhibitors in this setting.
The C3NIRA trial (NCT04592237) was an investigator-initiated phase II study evaluating the addition of αPD1 (cetrelimab) to carboplatin and cabazitaxel induction, followed by niraparib ± cetrelimab maintenance in patients with mCRPC and ≥1 AVPC criteria. Participants first receive 6 cycles of induction chemotherapy (carboplatin + cabazitaxel), with cetrelimab given on cycles 2–6, and are then randomized 1:1 to maintenance with either niraparib alone or niraparib + cetrelimab. This trial has the potential to answer three questions.
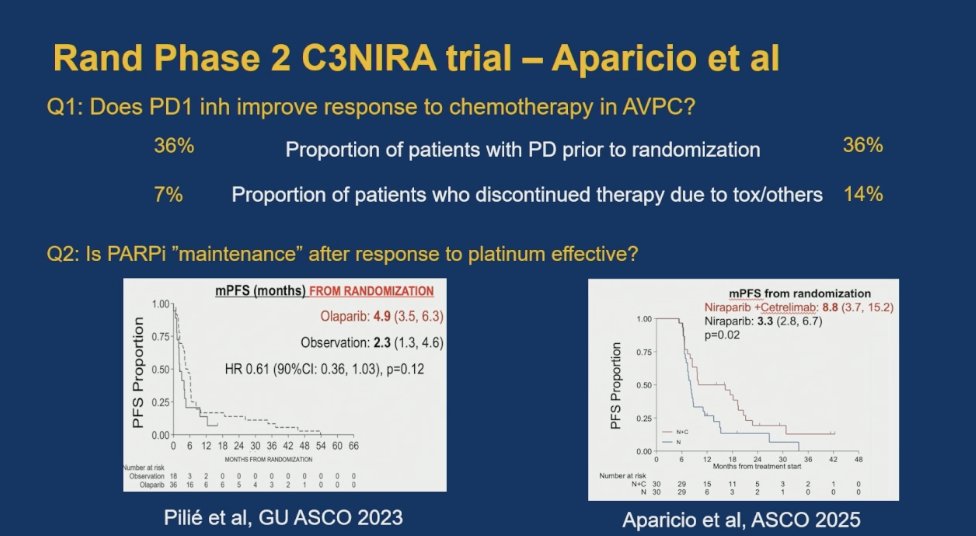
- Does PD1 inhibition improve response to chemotherapy in AVPC?
- Is PARPi "maintenance" after response to platinum effective?
- Does PD1 inhibitor enhance the effect of PARPi "maintenance"?
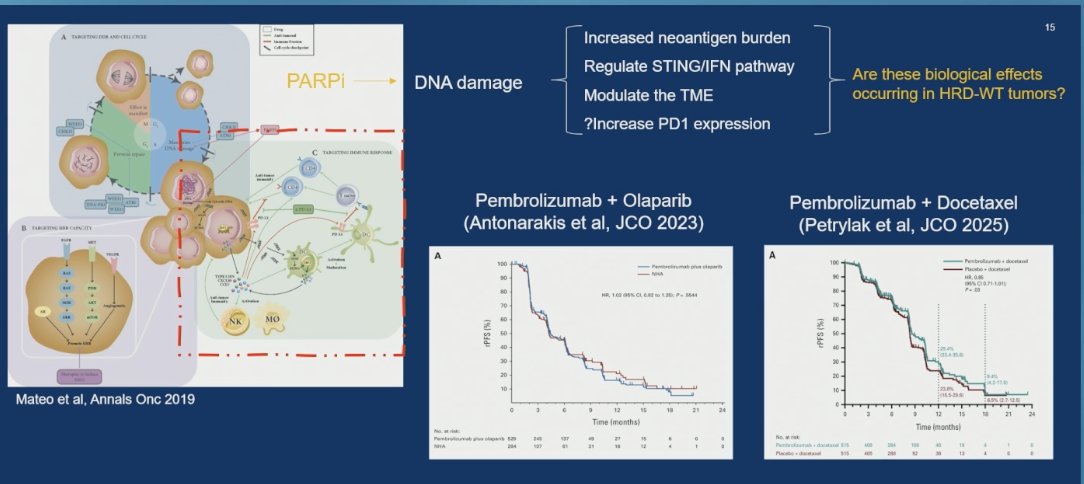
Prior studies investigating combinations such as pembrolizumab plus olaparib and pembrolizumab plus docetaxel have failed to demonstrate meaningful benefit, as illustrated below. In Dr. Mateo’s opinion, this reflects the limited understanding of therapeutic response outside of BRCA-mutated populations.
Is PARP inhibitor “maintenance” after response to platinum effective?
This remains a challenging question. Both arms had prior exposure to PARP inhibitors, making interpretation difficult. A prior study by Dr. Aparicio (Pilie et al., GU ASCO 2023) showed no significant benefit with olaparib maintenance following platinum therapy (median PFS: 4.9 vs 2.3 months; HR 0.61, 90% CI: 0.36–1.03; p=0.12). However, updated results from the C3NIRA trial (Aparicio et al., ASCO 2025) demonstrated improved mPFS with niraparib plus cetrelimab (8.8 vs 3.3 months; p=0.02), suggesting potential benefit in select patients.
This question builds on prior data presented by Dr. Aparicio, in which a subset of patients receiving the combination of niraparib and cetrelimab. In the most recent data, median overall survival (OS) from randomization was 24.3 months (95% CI: 9.5–40.3) for the combination arm versus 10.2 months (95% CI: 6.4–19.7) for niraparib alone (HR 0.51; 90% CI: 0.29–0.89; p=0.04). These findings suggest that PD-1 inhibition may enhance the durability of response to PARP inhibition in select patients. Preclinical data have also shown upregulation of inflammatory response pathways following chemotherapy, providing a potential mechanistic rationale for this combination.
- PARP inhibitor maintenance and PARPi ± IO combinations have not yet demonstrated clear benefit in metastatic prostate cancer
- Dynamic tumor adaptation, such as PD-1 upregulation in response to inflammatory signals, may inform trial design and help identify novel therapeutic targets.
- On-therapy biopsies can reveal adaptive vulnerabilities and support the development of adaptive trial strategies.
- These trials exemplify how hypothesis-driven research can guide treatment strategies tailored to distinct prostate cancer biologies.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Reference:
- Smith MR, Hussain M, Saad F, Chowdhury S, Oudard S, Hirmand M, et al. Niraparib in combination with abiraterone acetate and prednisone for metastatic prostate cancer. Lancet Oncol. 2022;23(3):362–373.
- de Bono J, Mateo J, Fizazi K, Saad F, Shore N, Sandhu S, et al. Olaparib for metastatic castration-resistant prostate cancer. N Engl J Med. 2023;388(2):130–141.
- Agarwal N, McGregor BA, McKay RR, Loriot Y, Dreicer R, Dorff TB, et al. TALAPRO-2: Talazoparib plus enzalutamide versus placebo plus enzalutamide as first-line treatment of metastatic castration-resistant prostate cancer (mCRPC). Lancet. 2023;401(10378):188–199.