(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting, held in Chicago, IL, was host to the Oral Abstract Session: Genitourinary Cancer—Prostate, Testicular, and Penile. Dr. Gerhardt Attard presented the Phase 3 AMPLITUDE trial: Niraparib and abiraterone acetate plus prednisone for metastatic castration-sensitive prostate cancer patients with alterations in homologous recombination repair genes.
Dr. Attard began by highlighting that the addition of an androgen receptor pathway inhibitor (ARPI), such as abiraterone acetate plus prednisone (AAP), to androgen deprivation therapy (ADT) either as doublet therapy or as part of triplet therapy with docetaxel remains the standard of care for patients with metastatic castration-sensitive prostate cancer (mCSPC).1-4 We have two classes of drugs (Docetaxel and ARPIs) that improve OS in this setting.
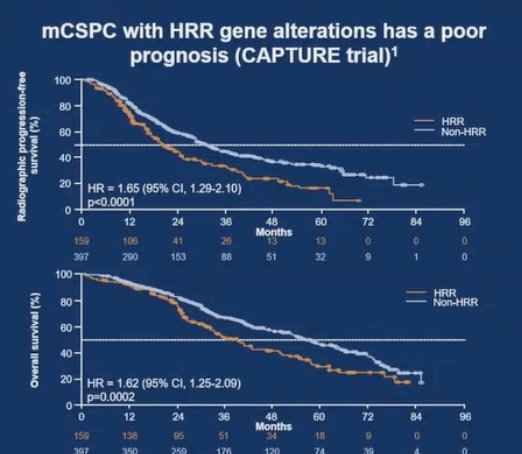
At ASCO 2025, Dr. Daniel Olmos presented data from the CAPTURE study conducted in Spain, which examined the prognostic role of homologous recombination repair mutations (HRRm) in patients with mHSPC receiving contemporary standard treatments. HRRm were identified in approximately 25% of patients and were associated with significantly worse survival outcomes compared to non-HRRm patients (HR 1.6; 95% CI, 1.3–2.1; p=0.0002).5
Niraparib, a potent and selective PARP-1/2 inhibitor, is already approved in combination with AAP for BRCA-mutated metastatic castration-resistant prostate cancer (mCRPC).6,7 The AMPLITUDE trial (NCT04497844) was designed to assess the efficacy of niraparib plus AAP in patients with HRRm mCSPC.
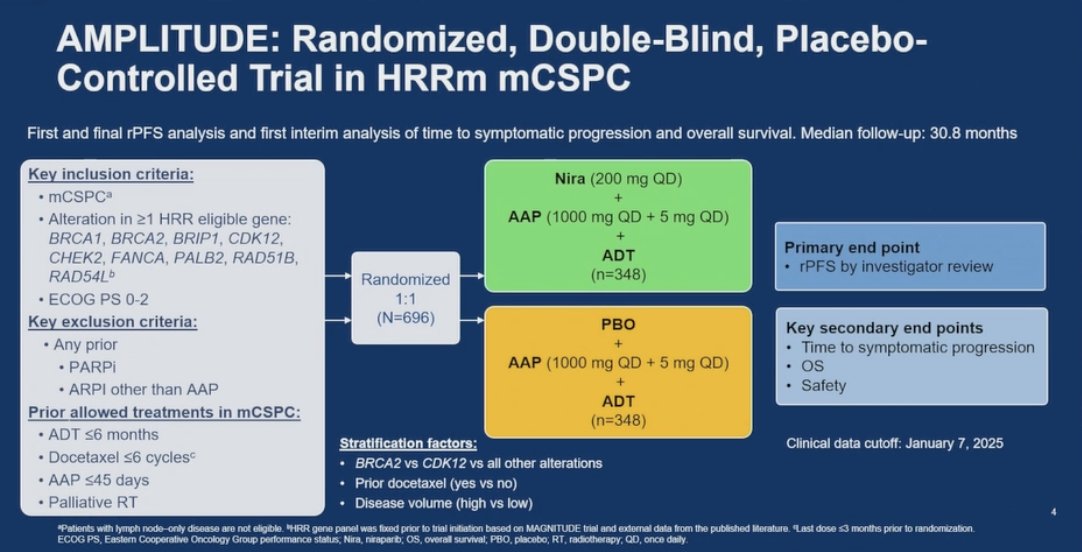
The AMPLITUDE trial is a randomized, double-blind, placebo-controlled phase 3 study evaluating the efficacy of a fixed daily tablet of niraparib (200 mg) in combination with abiraterone acetate plus prednisone (AAP 1000 mg + 5 mg) and continuous ADT in patients with mCSPC harboring at least one HRR mutation in one of these genes: BRCA1, BRCA2, BRIP1, CDK12, CHEK2, FANCA, PALB2, RAD51B, RAD54L.
A total of 696 patients with ECOG performance status 0–2 were randomized 1:1 to receive either niraparib + AAP + ADT or placebo + AAP + ADT. Prior treatments in the mCSPC setting were allowed, including ≤6 months of ADT, ≤6 cycles of docetaxel, or ≤45 days of AAP. Patients with prior PARP inhibitor use or ARPI exposure other than AAP were excluded. Stratification factors included BRCA2/CDK12 status, prior docetaxel use, and disease volume. The primary endpoint was radiographic progression-free survival (rPFS) by investigator assessment, with key secondary endpoints including time to symptomatic progression, overall survival, and safety. The study design is illustrated below.
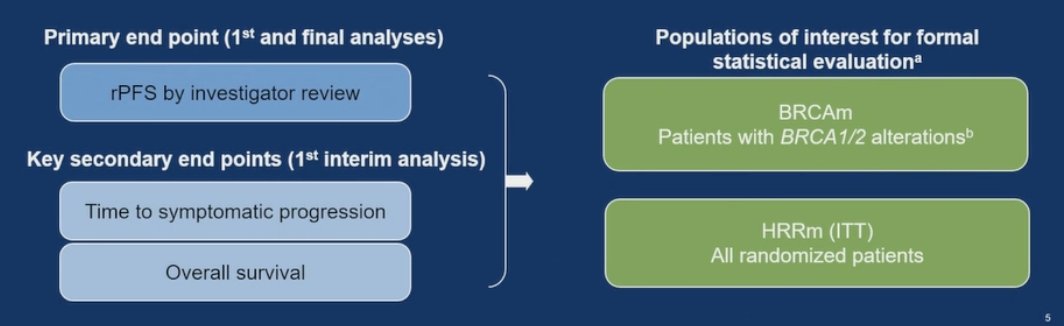
The statistical analysis plan for the AMPLITUDE trial used a graphical group sequential design to evaluate three hierarchical endpoints while controlling for an overall type I error rate of 0.05. The two main populations of interest for formal statistical evaluation were participants with BRCA1/2 alterations (BRCAm) and the full intent-to-treat HRRm population. The primary endpoint rPFS was assessed in both groups through first and final analyses. Key secondary endpoints, including time to symptomatic progression and overall survival, were evaluated during the first interim analysis. Notably, the HRR effectors subgroup, comprising patients with alterations in BRCA1/2, BRIP1, PALB2, RAD51B, and RAD54L, was also pre-specified for formal statistical analysis.
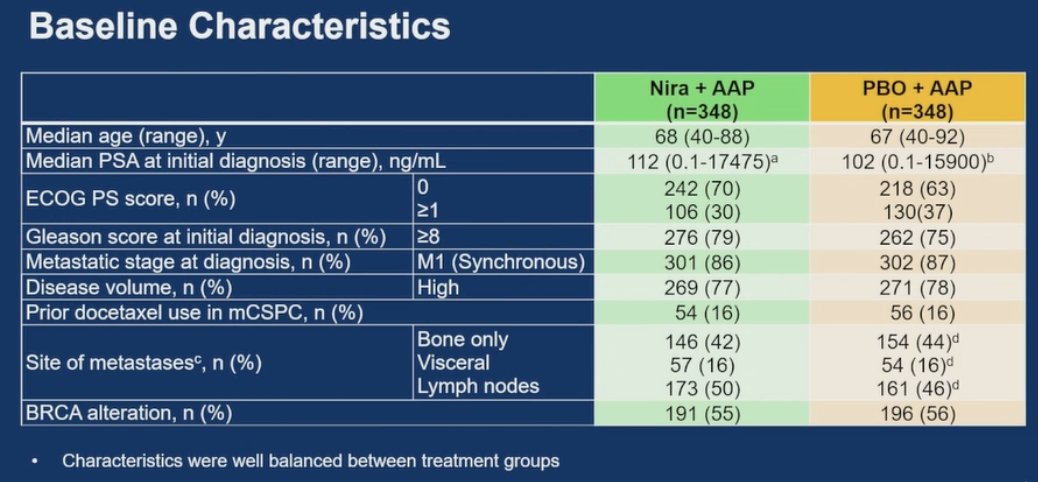
Dr. Attard noted that baseline characteristics were well balanced between treatment arms. He also emphasized that the characteristics of patients in the BRCAm subgroup were consistent with those observed in the overall HRRm population, supporting the comparability of outcomes across these cohorts. Dr Attard noted that over half of the patients had an alteration in BRCA 1/2.
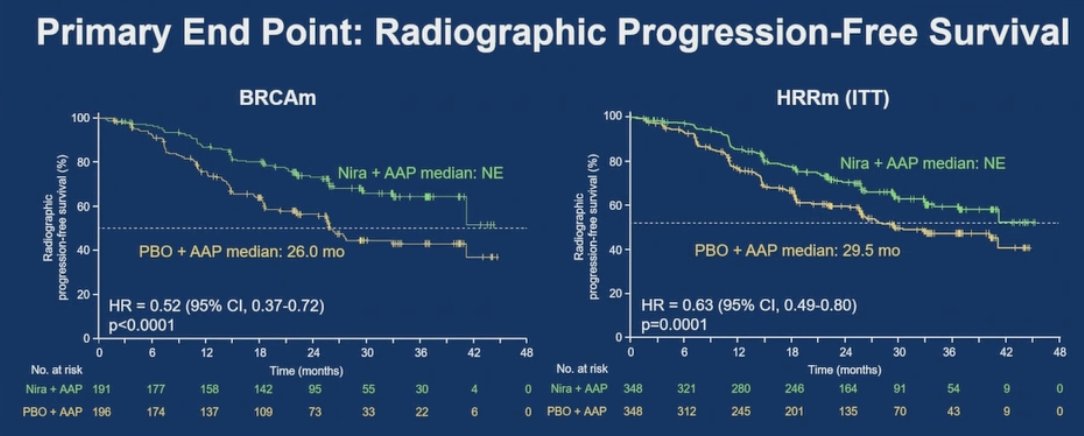
AMPLITUDE met its primary endpoint, demonstrating that the combination of niraparib and AAP significantly reduced the risk of radiographic progression or death by 48% in the BRCAm group (HR 0.52; 95% CI, 0.37–0.72; p < 0.0001) and by 37% in the broader HRRm population (HR 0.63; 95% CI, 0.49–0.80; p = 0.0001).
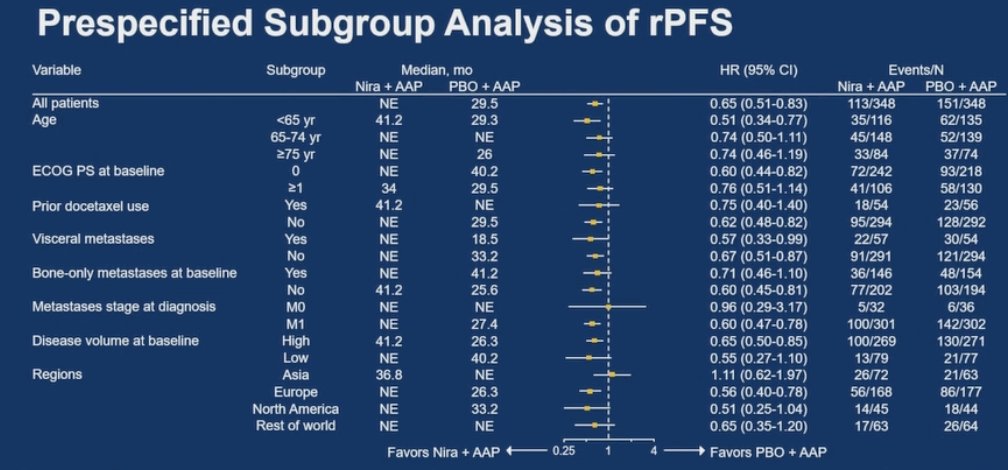
In the prespecified subgroup analysis, the rPFS benefit from niraparib plus AAP was consistent across all subgroups, as shown in the forest plot below.
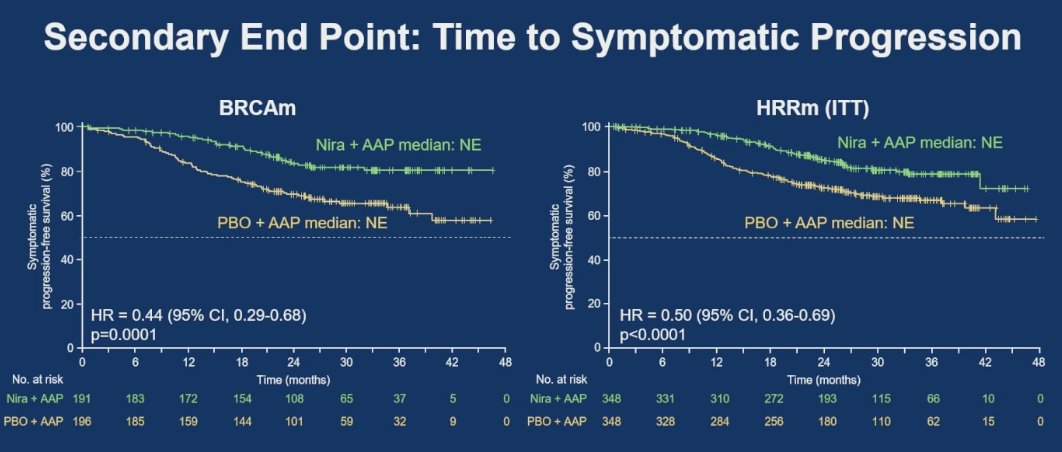
Dr. Attard highlighted that the combination of niraparib and AAP significantly reduced the risk of symptomatic progression by 56% in the BRCAm group (HR = 0.44; 95% CI, 0.29–0.68; p = 0.0001) and by 50% in the broader HRRm population (HR = 0.50; 95% CI, 0.36–0.69; p < 0.0001).
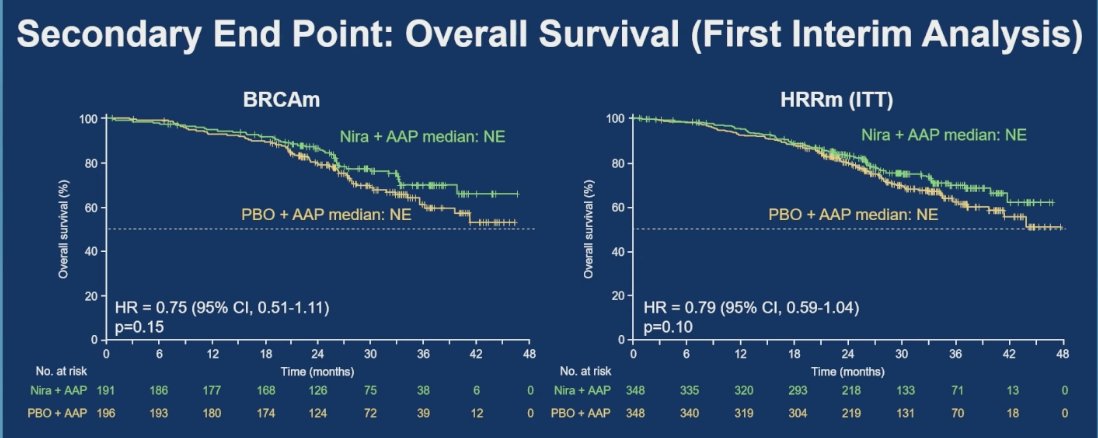
Moreover, the combination of niraparib and AAP was associated with a 25% reduction in the risk of death in the BRCAm group (HR = 0.75; 95% CI, 0.51–1.11; p = 0.15) and a 21% reduction in the HRRm group (HR = 0.79; 95% CI, 0.59–1.04; p = 0.10). However, overall survival analysis remains immature, as fewer than 50% of the required events have occurred in either group.
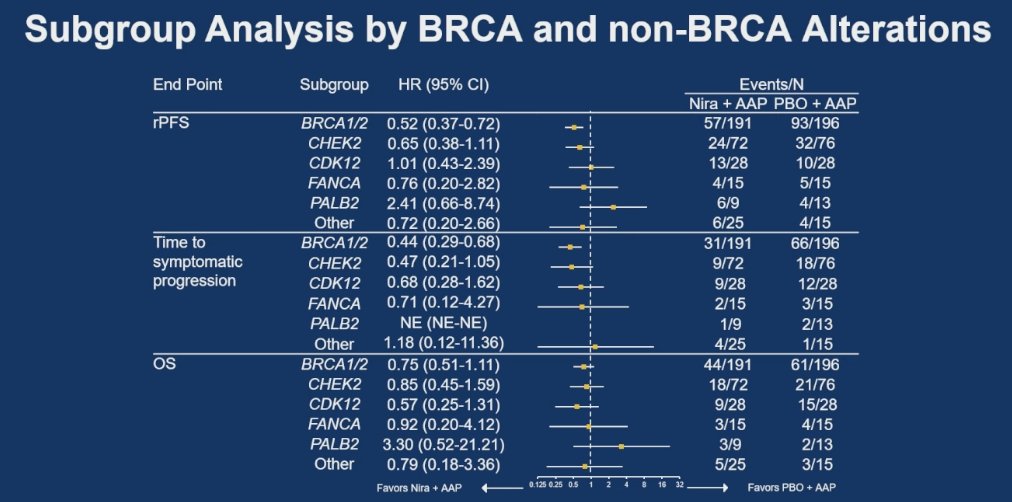
Dr. Attard presented a subgroup exploratory analysis stratified by BRCA and non-BRCA alterations, revealing that patients with BRCA mutations experienced the most pronounced improvement in rPFS with the combination of niraparib and AAP. In contrast, the benefit was less clear in patients with non-BRCA HRR mutations doing the gene-by-gene analysis, as the confidence intervals for these subgroups crossed the line of unity in the forest plot. However, these analyses are limited by the limited number of patients in the other gene groups.
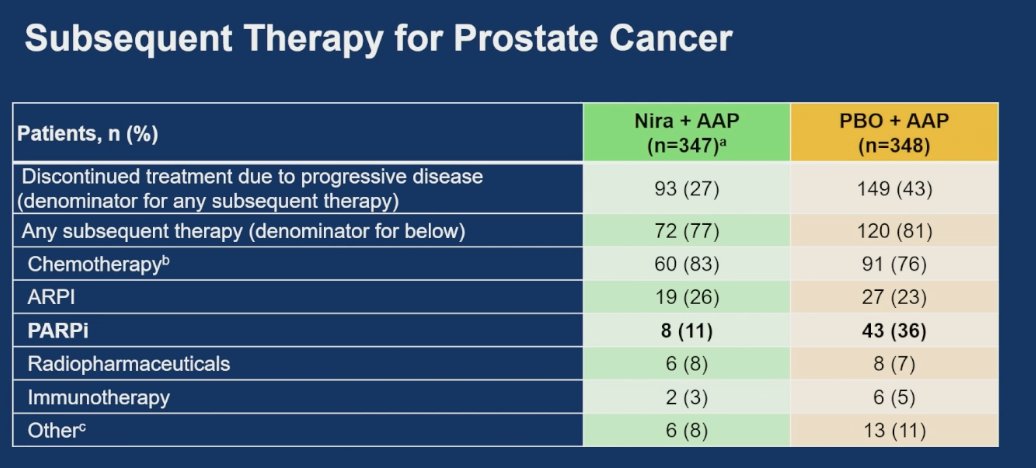
Notably, 54% of patients in the niraparib + AAP arm remained on treatment at the time of analysis, while 27% discontinued due to progressive disease. In comparison, only 44% of patients in the placebo arm remained on treatment, and 43% discontinued for progression. Importantly, the majority of patients in both arms who went on to receive subsequent therapy, most commonly received chemotherapy, which supports the robustness of the study's findings.
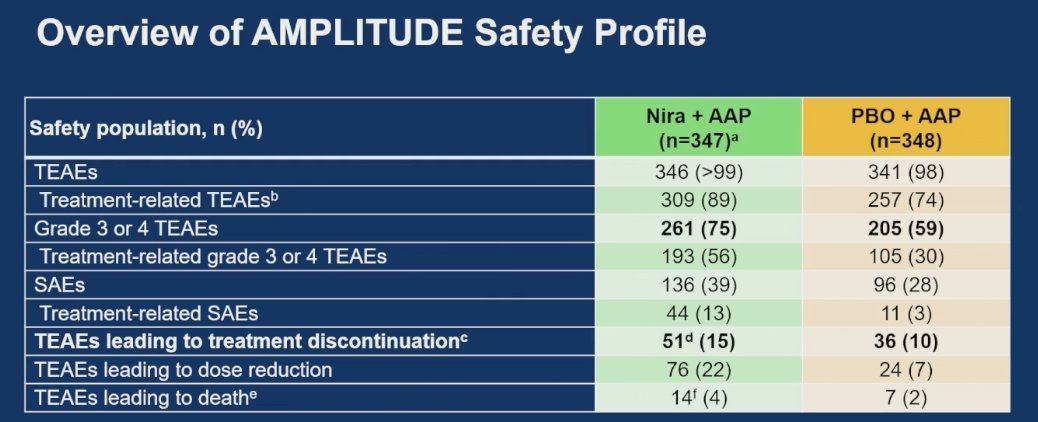
Most participants remained on treatment, and the adverse event (AE) profile was generally manageable. Treatment-emergent adverse events (TEAEs) were reported in nearly all patients 99% in the niraparib + AAP arm and 98% in the placebo + AAP arm. Serious AEs occurred in 39% of patients receiving the combination therapy compared to 28% in the control group. TEAEs leading to treatment discontinuation were observed in 15% of patients in the niraparib + AAP group versus 10% in the placebo arm, showing a difference of less than 1%.
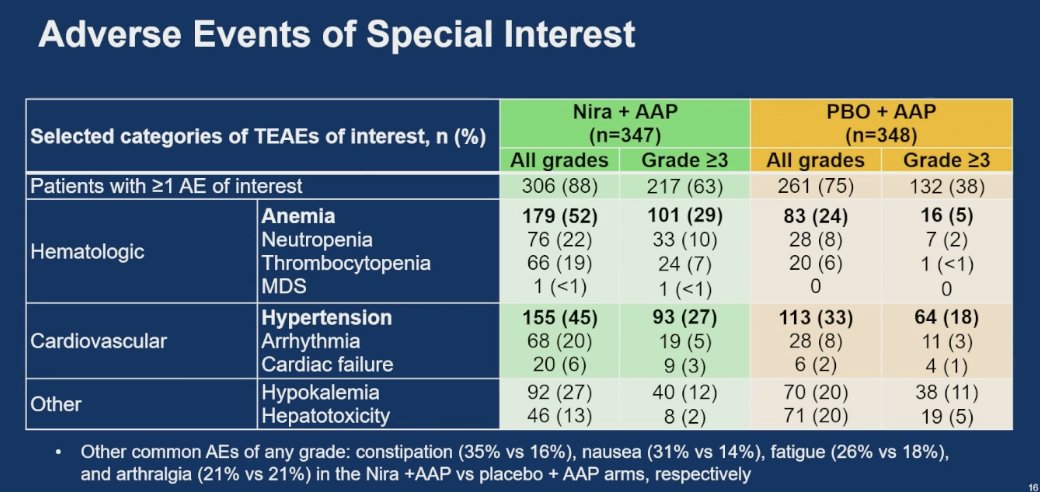
Notably, anemia was a common adverse event with niraparib, occurring in 52% of patients receiving niraparib + AAP, including 29% with Grade ≥3 events. In comparison, anemia occurred in 24% of patients in the placebo + AAP group, with only 5% experiencing Grade ≥3. Hypertension was another relevant toxicity, reported in 45% of patients in the niraparib arm versus 33% in the control group; Grade ≥3 hypertension occurred in 27% and 18% of patients, respectively.
Dr Attard concluded his presentation with the following key takeaway points:
- The AMPLITUDE trial met its primary endpoint of improved rPFS, demonstrating the efficacy of combining a PARPi (niraparib) with an ARPI (AAP) in mCSPC patients with HRR alterations.
- Patients with BRCA mutations derived the greatest benefit from the combination.
- Improvements in rPFS were accompanied by a statistically significant delay in time to symptomatic progression and a trend toward improved overall survival.
- The safety profile of niraparib + AAP was consistent with previous data from the MAGNITUDE trial, with <5% higher treatment discontinuation due to toxicity compared to placebo.
- AMPLITUDE supports niraparib + AAP as a potential new treatment option for mCSPC patients with BRCA or other HRR gene alterations.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: AMPLITUDE Trial: Niraparib Delays Progression in HRR-Mutant Prostate Cancer - Gerhardt Attard
Reference:
- Fizazi K, et al. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med. 2017;377(4):352-360.
- James ND, et al. Abiraterone for prostate cancer not previously treated with hormone therapy. N Engl J Med. 2017;377(4):338-351.
- Fizazi K, et al. Abiraterone plus prednisolone with or without enzalutamide in high-risk metastatic hormone-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 trial. Lancet. 2022;399(10336):1695-1707.
- Smith MR, et al. Apalutamide and overall survival in metastatic castration-sensitive prostate cancer. N Engl J Med. 2022;386(13):1132-1142.
- Olmos D, et al. Impact of somatic/germline homologous recombination repair (HRR) alterations on metastatic hormone-sensitive prostate cancer (mHSPC) outcomes by disease volume. Presented at: ASCO Annual Meeting; 2025. Abstract 5094.
- Chi KN. Talazoparib plus enzalutamide in metastatic castration-resistant prostate cancer with DNA repair alterations: updated results from TALAPRO-2. J Clin Oncol. 2023;41(16):3339-3351.
- Chi KN, et al. Talazoparib plus enzalutamide in metastatic castration-resistant prostate cancer. Ann Oncol. 2023;34(7):772-782.