(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to the Session State of the Art Lecture: Personalizing treatment for patients with metastatic castration resistant prostate cancer (mCRPC) in 2025. Dr. Himisha Beltran delivered a presentation on Non-Androgen-Receptor–Driven Prostate Cancer: Updates in Biology, Classification, and Management.
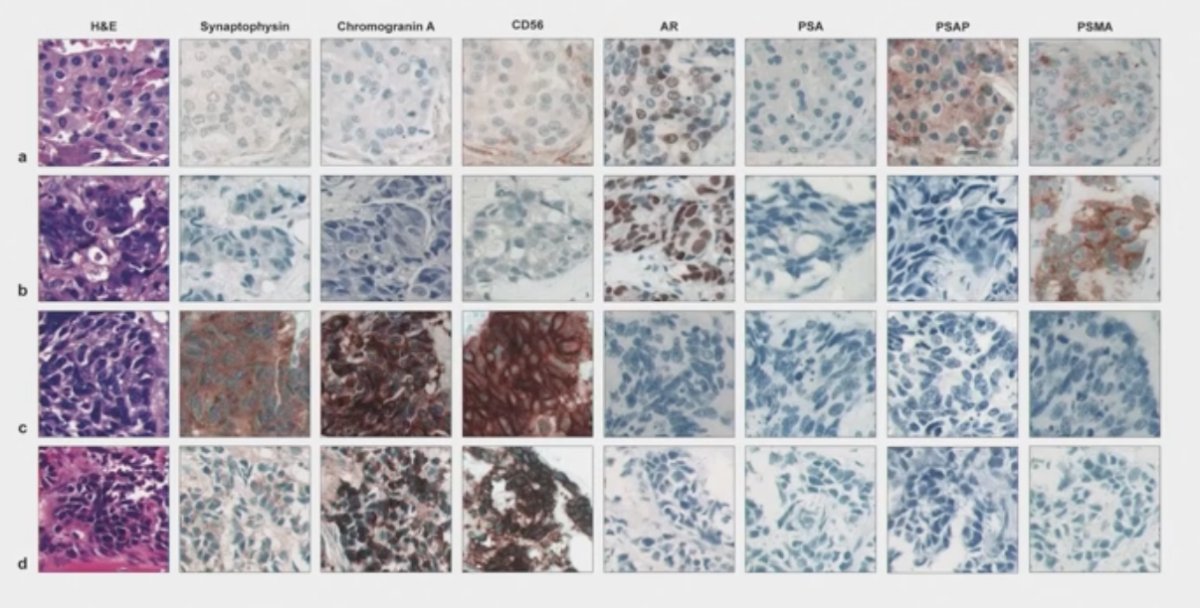
Castration-resistant prostate cancer (CRPC) is a heterogeneous disease clinically, genomically, and pathologically. A wide range of histologic subtypes can be observed, and some tumors may even lose key therapeutic targets such as prostate-specific membrane antigen (PSMA) and the androgen receptor (AR), as shown below.
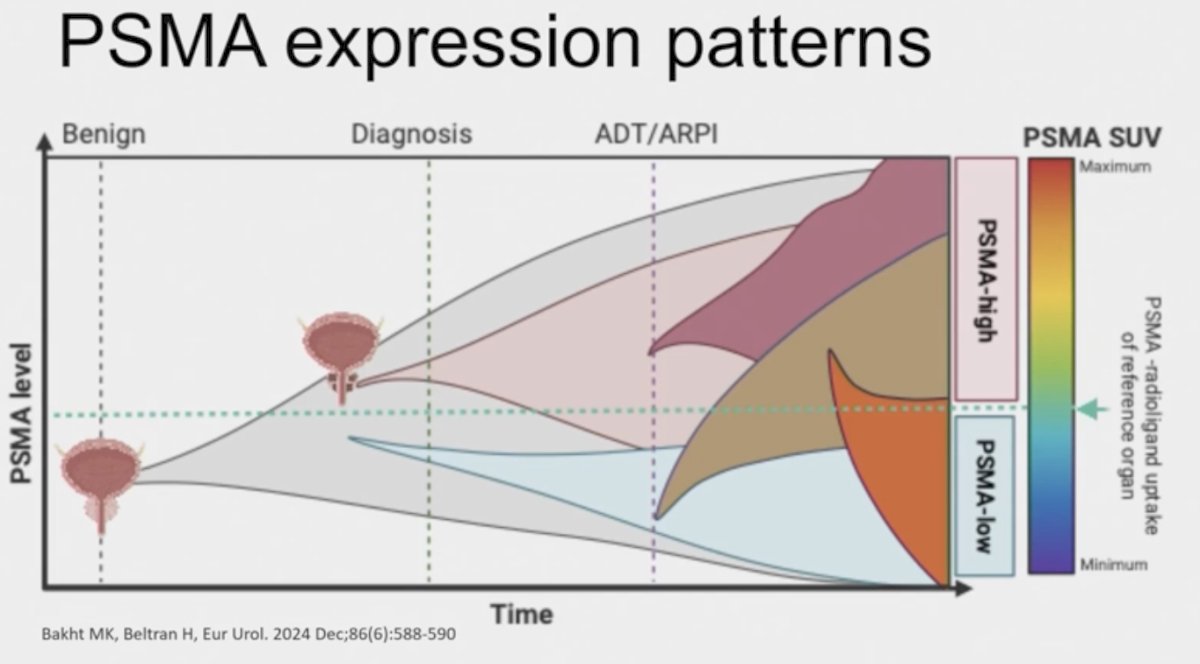
There are varying levels of heterogeneity in prostate cancer. At the tissue level, prostate tumors can exhibit diverse patterns of PSMA expression, with higher degrees of heterogeneity observed in advanced disease, as illustrated below. Notably, PSMA expression is lost in a subset of late-stage prostate cancers. This includes androgen receptor (AR)-negative small cell neuroendocrine prostate cancer (NEPC), a particularly aggressive subtype.
Neuroendocrine prostate cancer (NEPC) is a highly aggressive variant that may arise de novo or develop as a mechanism of treatment resistance. This phenomenon, known as lineage plasticity, occurs when tumors suppress their luminal adenocarcinoma characteristics and adopt a neuroendocrine phenotype. Recognizing this transformation is clinically important, as patients with NEPC may benefit from treatment regimens typically used for small cell lung cancer (SCLC). Despite this, both diagnosis and management of NEPC remain challenging due to its heterogeneous presentation and limited therapeutic options.
Dr. Beltran emphasized the importance of considering a biopsy to evaluate for neuroendocrine prostate cancer (NEPC), though she acknowledged the lack of clear guidelines on when to perform one. Given that NEPC is relatively uncommon, routine re-biopsy for all patients is likely to yield limited benefit. However, she personally considers biopsy in specific clinical scenarios, including cases of aggressive disease with low or non-rising PSA levels, PSMA-negative lesions on PSMA PET/CT, particularly if FDG-avid, and a history of mixed histologic features on prior biopsy to assess the dominant subtype. The rationale for biopsy in these cases includes early consideration of platinum-based chemotherapy, informed selection of next-line therapies, and eligibility for clinical trials.
The current diagnosis of NEC remains imperfect and variable. While some clinicians report rarely encountering NEPC, others suggest that 15–20% of CRPC tumors may exhibit neuroendocrine features. Several factors may contribute to this discrepancy, including the fact that repeat biopsies are not routinely performed in metastatic CRPC and that there is substantial variability among pathologists due to a lack of standardized evaluation criteria and nomenclature. Additionally, significant intra-patient heterogeneity further complicates accurate diagnosis and characterization.Over a decade ago, Dr. Beltran led a workshop in collaboration with the Prostate Cancer Foundation (PCF) that proposed a morphologic classification system for prostate cancers with neuroendocrine differentiation. In clinical practice, defining these morphologic features, particularly after androgen deprivation therapy (ADT) and chemotherapy, remains challenging. As a result, most pathology departments rely on immunohistochemistry (IHC) to confirm the diagnosis of neuroendocrine prostate cancer.
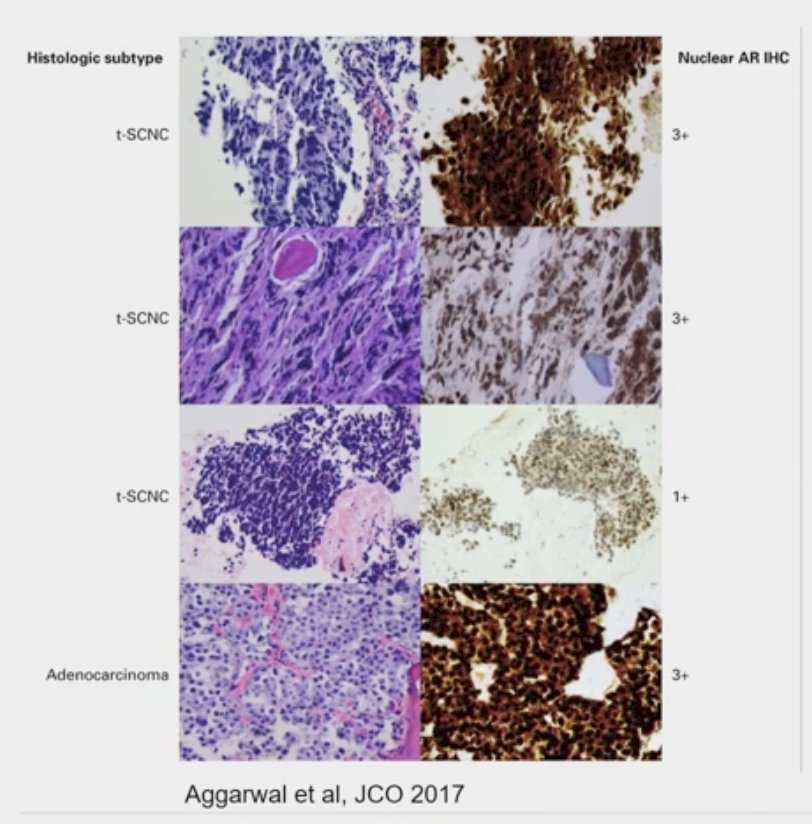
Additional studies, including those from the West Coast SU2C-PCF cohort, have helped uncover other clinically relevant prostate cancer variants. In biopsies obtained after treatment with androgen receptor (AR) pathway inhibitors, 17% of cases demonstrated treatment-emergent small cell neuroendocrine carcinoma. Interestingly, these tumors often retained AR expression but exhibited low AR signaling activity. These findings highlight that certain aggressive subtypes may not be identifiable through morphology alone, underscoring the importance of integrating molecular and functional analyses into diagnostic workflows.1
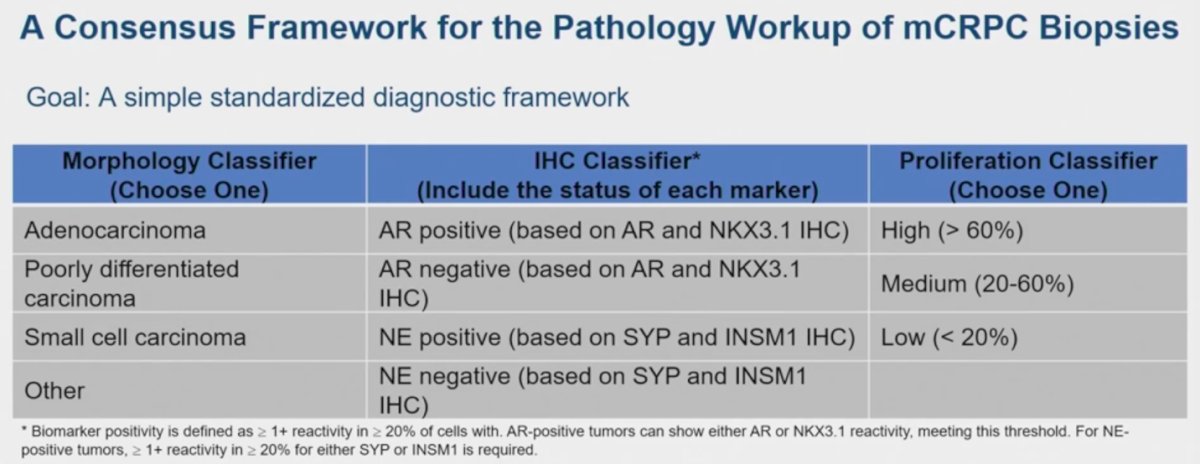
Recently, Dr. Beltran led a renewed pathology working group that brought together clinicians and pathologists with the goal of standardizing the diagnostic workup of mCRPC. The group emphasized the importance of going beyond IHC alone and proposed that every prostate cancer biopsy should be classified based on a comprehensive set of criteria outlined below:
- CRPC Morphology
- Adenocarcinoma: Gland formation, abundant cytoplasm, open/vacuolated chromatin, and prominent nucleoli. Mitotic figures and necrosis are typically absent.
- Small cell carcinoma: Sheets or clusters of cells with hyperchromatic nuclei, finely dispersed chromatin, no nucleoli, scant cytoplasm, and high nuclear-to-cytoplasmic ratio. Frequently shows mitotic figures, apoptosis, and necrosis.
- Poorly differentiated carcinoma: Lacks glandular formation, morphologically indistinct from high-grade carcinomas of other origins. May show variable neuroendocrine marker expression.
- Other morphologic variants: Includes squamous, sarcomatoid, pleomorphic giant cell, and large cell neuroendocrine carcinoma.
- Mixed morphology: Presence of two or more distinct morphologic populations; each subtype should be quantified by percentage.
- IHC Classifiers
- Neuroendocrine markers
- Recommended: synaptophysin (SYP) and INSM1
- Other discussed: chromogranin A, CD56
- AR signaling markers
- Recommended: AR and NKX3.1
- Other discussed: PSA, prostein, PSMA
- Proliferation index – Ki-67
- In localized adenocarcinoma: typically low (median ~2%)
- In CRPC: elevated (median ~20%)
- In NEPC: markedly high (>60%)
- Reporting: Percentage of positive cells and predominant staining intensity (0, 1+, 2+, 3+) should be documented. Mixed intensity populations (e.g., 1+ and 3+) should be noted. AR staining should include an aggregate score for nuclear and cytoplasmic reactivity.
- Additional markers (context-dependent)
- Example: DLL3 may be useful in select cases
A consensus framework for the pathology workup of mCRPC biopsies was recently proposed, incorporating three key components: morphologic classification, IHC profiling, and proliferation index assessment. This structured approach allows for more precise characterization of tumor biology. Notably, a profile of "prostatic adenocarcinoma, AR-positive, NE-negative, Ki-67 20%" is considered the least aggressive, whereas "small cell carcinoma, AR-negative, NE-positive, Ki-67 70%" reflects a highly aggressive disease phenotype with poor clinical outcomes.
Genomic testing
- Next-generation sequencing (NGS) is now standard for all patients with mCRPC.
- RB1 and TP53 alterations are commonly observed in neuroendocrine prostate cancer (NEPC) but may also be seen in prostatic adenocarcinoma and other malignancies.
- These alterations may aid in risk stratification or guide patient selection for platinum-based therapies, particularly in the context of clinical trials.
Confirming prostate origin
- TMPRSS2-ERG rearrangements, detectable via FISH or NGS, are present in approximately 50% of prostate cancers and are highly specific for prostate origin.
- When the diagnosis is uncertain, comparing genomic profiles between the primary tumor and metastatic lesions via NGS can help confirm prostate origin.
Double-negative prostate cancer
- A subset of CRPC tumors lack both androgen receptor (AR) and neuroendocrine (NE) marker expression, commonly referred to as "double-negative prostate cancer."
- This is a diagnosis of exclusion and may require additional testing to establish a prostatic origin.
- The number and type of luminal and NE markers needed to confidently confirm a double-negative phenotype remain uncertain, as no single marker offers 100% sensitivity.
Dr. Beltran emphasized that this is a rapidly evolving area. She noted that integrating standardized assessments of morphology, IHC, and genomics may help clarify the clinical implications of prostate cancer variants that emerge along the spectrum of lineage plasticity.
Molecular diagnostics will play a critical role in the future of prostate cancer care, particularly as our understanding of lineage plasticity deepens. This biologic process is driven in part by the loss of tumor suppressors such as TP53 and RB1, along with activation of lineage-defining transcription factors and epigenetic reprogramming. These insights are helping to define new therapeutic targets and may ultimately guide the development of more precise treatment strategies and are illustrated below.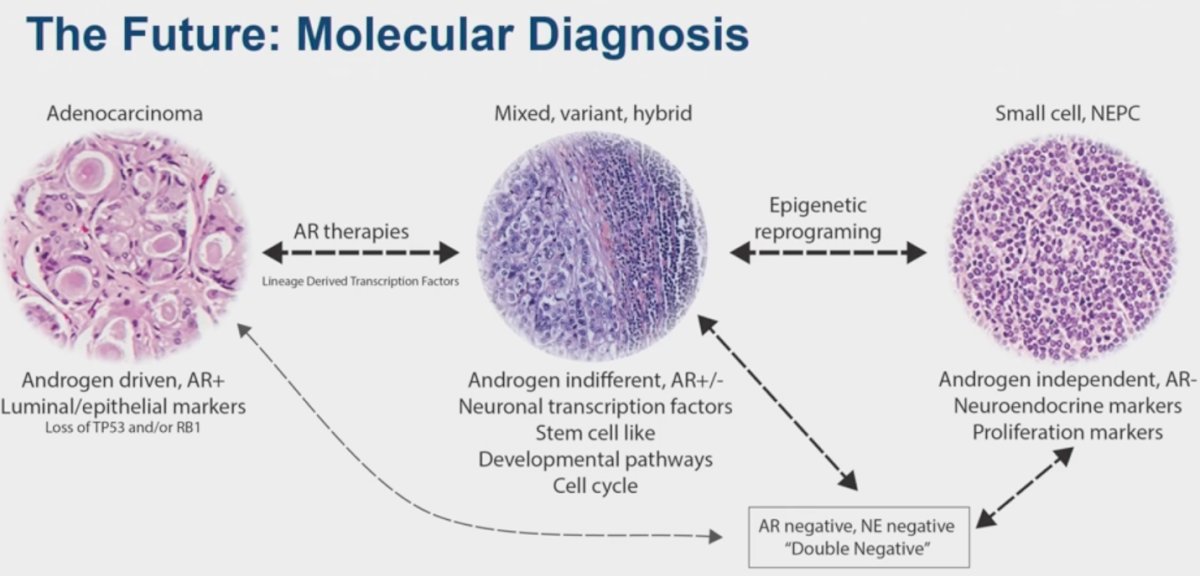
Epigenetic profiling is emerging as a promising tool for identifying novel biomarkers in prostate cancer. The NEuroendocrine MOnitoring (NEMO) targeted methylation panel analyzes cell-free DNA (cfDNA) to quantify a phenotypic score based on differential methylation patterns. This platform allows for the inference of tumor content, neuroendocrine phenotype scores, and transcriptional state. Techniques such as methylation panels, ChIP-seq, and others are contributing to a deeper understanding of lineage plasticity and may support future precision diagnostics in CRPC.

Treatment Considerations for NEPC
Dr. Beltran emphasized that, for now, patients with NEPC or aggressive variant prostate cancer should continue androgen deprivation therapy (ADT). Platinum-based chemotherapy remains a cornerstone, with specific regimens tailored to clinical context. For patients who have not previously received docetaxel, a combination of carboplatin and docetaxel may be considered, though data remain limited. Alternatively, phase II evidence supports the use of carboplatin and cabazitaxel in patients with aggressive variant CRPC. In cases of pure small cell carcinoma, especially de novo presentations, a regimen of platinum plus etoposide, with or without immune checkpoint inhibitors, followed by IO maintenance, may be appropriate, extrapolated from small cell lung cancer protocols.
The use of CRPC-directed therapies such as ARPIs or Lu-PSMA-617 may still be considered, depending on the disease context, including factors such as PSA level, bone-only disease, mixed histology, or PSMA-PET positivity
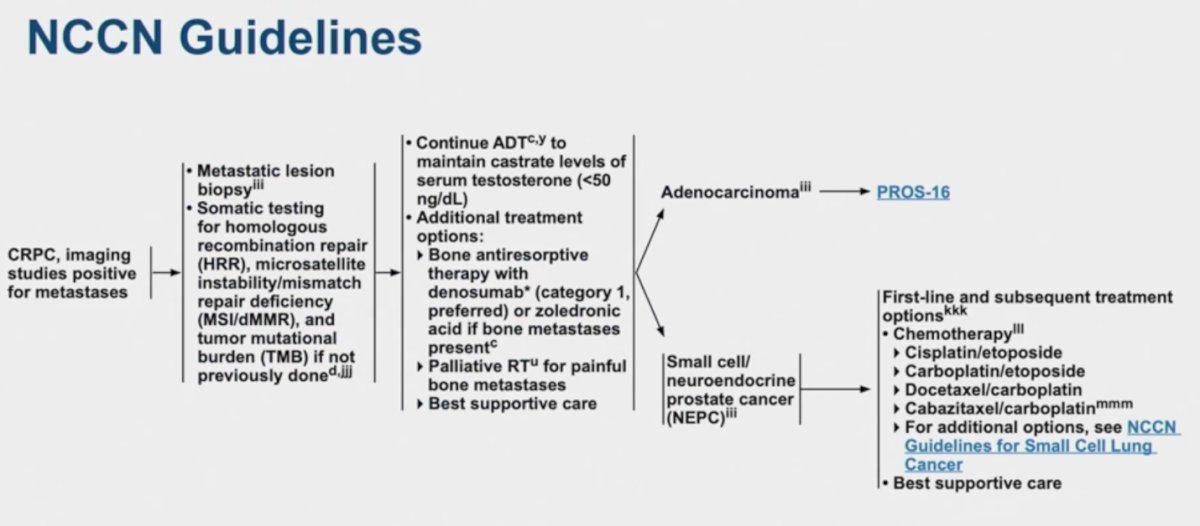
The NCCN Guidelines recommend platinum-based chemotherapy for NEPC and refer to treatment protocols established for small cell lung cancer (SCLC) as a reference framework.
When selecting the next line of therapy for patients with NEPC, treatment decisions should be guided by the dominant histologic subtype and associated clinical features. If the tumor exhibits a small cell morphology, regimens commonly used for small cell lung cancer may be considered. These include agents such as tarlatamab, lurbinectedin, and topotecan. While immune checkpoint blockade with ipilimumab/nivolumab has shown limited data in NEPC, it may be an option in select cases. Alternatively, if the clinical context is more consistent with castration-resistant prostate cancer (CRPC), standard CRPC therapies should be considered. Molecularly driven approaches, such as PARP inhibitors in patients with BRCA2 mutations, also play an important role. Whenever feasible, enrollment in a clinical trial is encouraged to access investigational therapies and help define optimal management strategies.
Delta-like protein 3 (DLL3) is a surface-expressed protein that is highly enriched in neuroendocrine prostate cancer (NEPC), with expression observed in approximately 77% of cases. Notably, DLL3 is not expressed in benign prostate tissue or localized prostate cancer. While a subset of mCRPC tumors may express DLL3 (approximately 12.5%), the staining tends to be more focal and less homogeneous compared to NEPC, as demonstrated in the figure below.
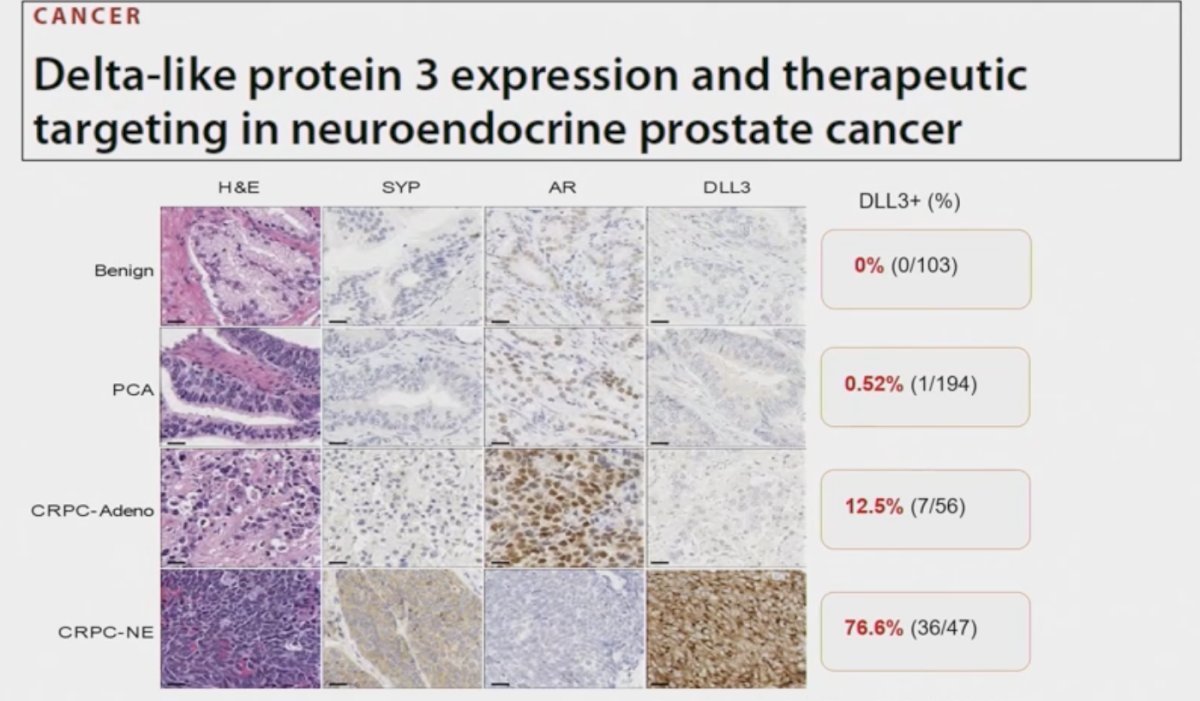

Dr. Beltran noted that DLL3 may serve not only as a therapeutic target but also as a biomarker to distinguish between prostate cancer phenotypes. As illustrated below, patients with adenocarcinoma typically exhibit high PSMA expression and are DLL3-negative, whereas those with NEPC show low or absent PSMA expression and high DLL3 levels. This inverse relationship could support the use of DLL3 in both diagnostic stratification and treatment selection.

Neuroendocrine differentiation can also be observed in hormone-sensitive prostate cancer. "De novo" NEPC shares similar pathological and molecular features with treatment-emergent NEPC (t-NEPC), though it remains a heterogeneous entity. This includes pure small cell carcinoma as well as tumors with mixed adenocarcinoma and NE characteristics. In clinical practice, some patients present with NE features while still expressing androgen receptor (AR), maintaining high PSA levels, and demonstrating PSMA positivity features more typical of conventional prostate adenocarcinoma. These patients are often managed according to HSPC treatment guidelines. However, this raises important treatment considerations, such as whether more intensive approaches like triplet or quadruplet therapy, ADT, AR pathway inhibitor, docetaxel, and carboplatin may be appropriate. Additionally, such patients may benefit from closer imaging surveillance and consideration of repeat biopsy at progression to monitor for lineage plasticity or emerging NE dominance.
Dr. Beltran concluded her presentation with the following take-home messages:
- Increased awareness of AR-independent CRPC has enhanced diagnostic accuracy and deepened understanding of the molecular pathogenesis of NEPC.
- NEPC remains difficult to diagnose due to marked heterogeneity and the current lack of standardized workup for mCRPC biopsies, including morphology and IHC markers.
- It is critical to recognize the prognostic and therapeutic implications of NE differentiation.
- Molecular biomarkers, including non-invasive approaches such as ctDNA and molecular imaging, may improve the detection of NEPC and other phenotypic subtypes.
- Emerging therapeutic targets, such as DLL3, are under clinical investigation. Enrollment in clinical trials should be considered whenever possible.
Presented by: Himisha Beltran, MD, FASCO, Associate Professor of Medicine in the Lank Center for Genitourinary Oncology and the Division of Molecular and Cellular Oncology at Dana-Farber Cancer Institute, Boston, MA.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Reference:
- Aggarwal R, Huang J, Alumkal JJ, Zhang L, Feng FY, Thomas GV, Weinstein AS, Friedl V, Zhang C, Witte ON, Lloyd P, Gleave M, Evans CP, Youngren J, Beer TM, Rettig M, Wong CK, True L, Foye A, Playdle D, Ryan CJ, Lara P, Chi KN, Uzunangelov V, Sokolov A, Newton Y, Beltran H, Demichelis F, Rubin MA, Stuart JM, Small EJ. Clinical and Genomic Characterization of Treatment-Emergent Small-Cell Neuroendocrine Prostate Cancer: A Multi-institutional Prospective Study. J Clin Oncol. 2018 Aug 20;36(24):2492-2503. doi: 10.1200/JCO.2017.77.6880. Epub 2018 Jul 9. PMID: 29985747; PMCID: PMC6366813.
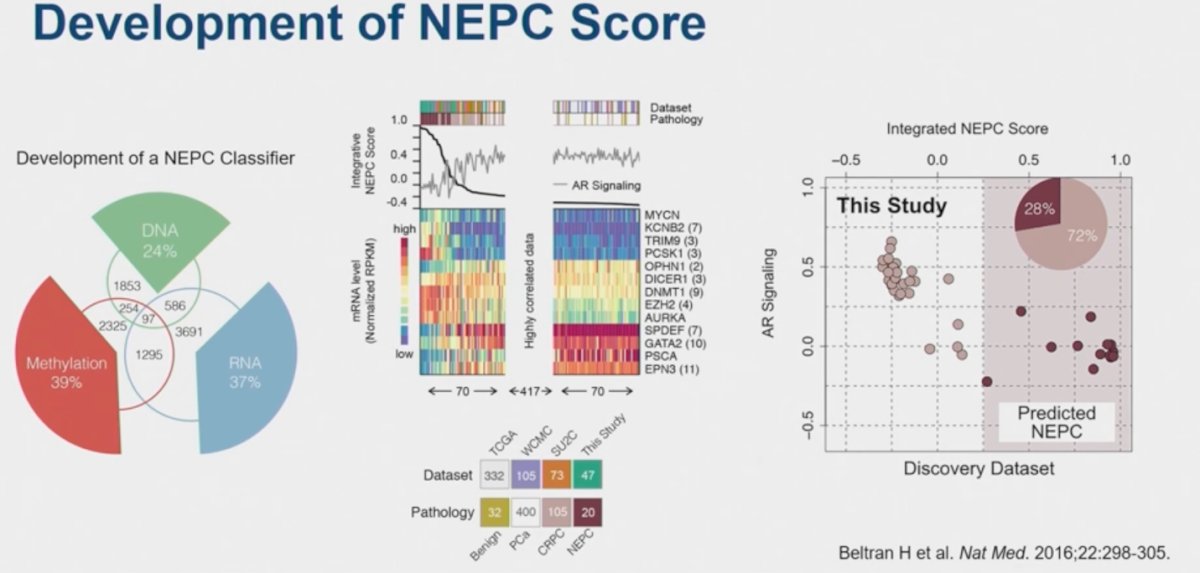
- Beltran H, Prandi D, Mosquera JM, Benelli M, Puca L, Cyrta J, Marotz C, Giannopoulou E, Chakravarthi BV, Varambally S, Tomlins SA, Nanus DM, Tagawa ST, Van Allen EM, Elemento O, Sboner A, Garraway LA, Rubin MA, Demichelis F. Divergent clonal evolution of castration-resistant neuroendocrine prostate cancer. Nat Med. 2016 Mar;22(3):298-305. doi: 10.1038/nm.4045. Epub 2016 Feb 8. PMID: 26855148; PMCID: PMC4777652.