(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to the Oral Abstract Session: Genitourinary Cancer—Prostate, Testicular, and Penile. Dr. Andrew Armstrong presented the 5-year follow-up overall survival (OS) analysis of enzalutamide (ENZA) plus androgen-deprivation therapy (ADT) in patients with metastatic hormone-sensitive prostate cancer (mHSPC) in the ARCHES study.
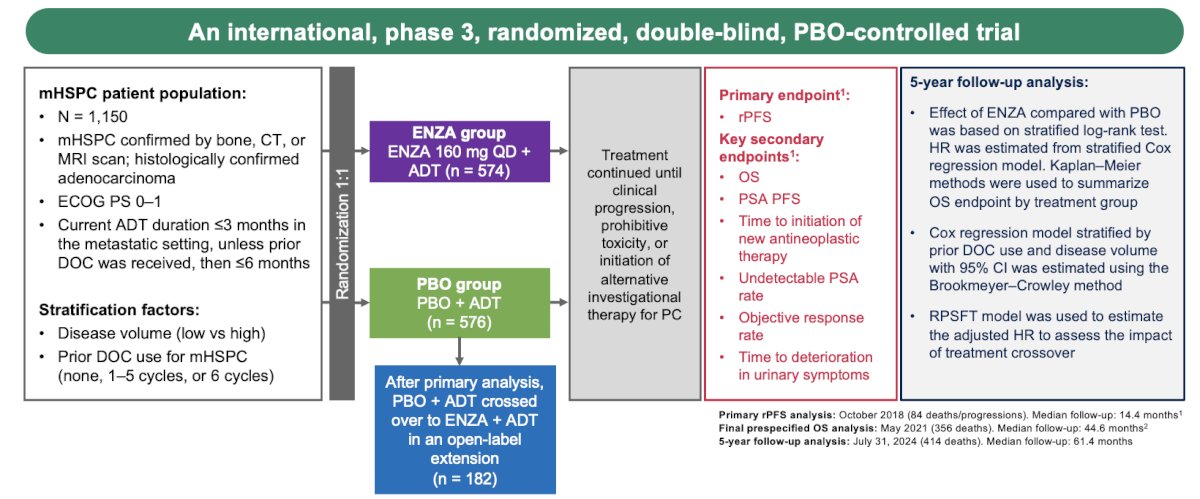
Dr. Armstrong began by highlighting the key findings from the ARCHES trial (NCT02677896), which evaluated enzalutamide (ENZA) plus androgen deprivation therapy (ADT) in patients with metastatic hormone-sensitive prostate cancer (mHSPC). The primary analysis, conducted in October 2018, demonstrated that ENZA + ADT significantly reduced the risk of radiographic progression or death by 61% compared to placebo + ADT (median not reached vs. 19.0 months; HR 0.39; 95% CI: 0.30–0.50; P<0.001) after a median follow-up of 14.4 months. With extended follow-up to May 2021 (median 44.6 months), ENZA + ADT also significantly reduced the risk of death by 34% (HR 0.66; 95% CI: 0.53–0.81; P<0.0001), although median OS was not reached in either group.1 Dr. Armstrong presented a post hoc analysis aimed at describing 5-year survival outcomes and long-term safety of ENZA + ADT versus PBO + ADT, with a data cutoff of July 31, 2024.
The study design of ARCHES involved 1,150 patients with mHSPC, randomized to receive either ENZA or placebo, both in combination with ADT. For the 5-year follow-up analysis, OS was assessed using Kaplan-Meier methods by treatment group. The effect of ENZA versus placebo was analyzed using a stratified log-rank test, and hazard ratios were estimated with a stratified Cox regression model, accounting for prior docetaxel use and disease volume. Confidence intervals were calculated using the Brookmeyer-Crowley method. To address the impact of treatment crossover, a rank-preserving structural failure time (RPSFT) model was used to estimate adjusted hazard ratios.
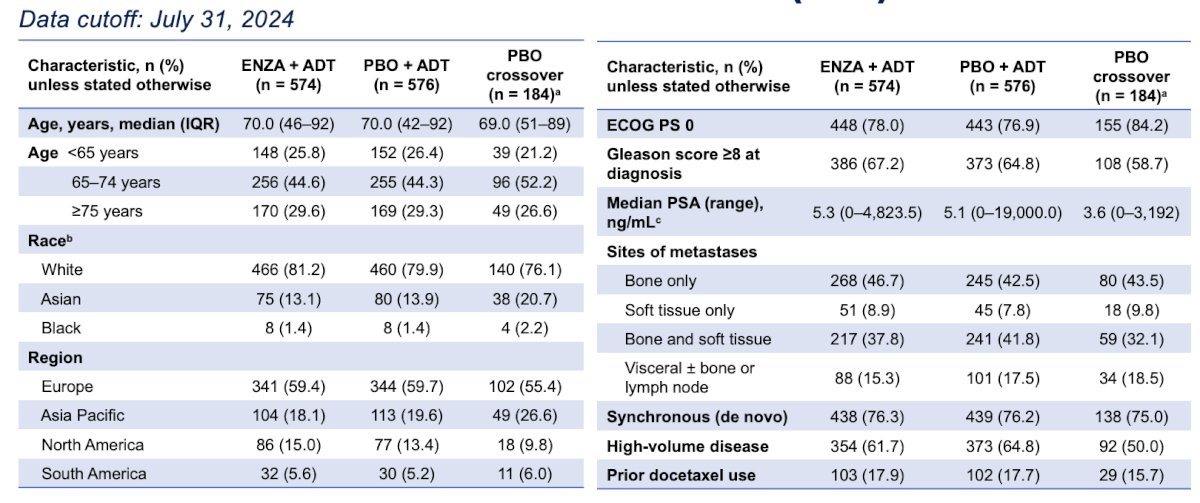
Baseline characteristics were well balanced between the ENZA and placebo groups. Importantly, 184 patients from the placebo arm crossed over to receive enzalutamide and were included in the intent-to-treat (ITT) population. As shown in the data, the majority of patients in both groups had synchronous metastatic disease (>75%) and high-volume disease. Additionally, between 15% and 17% of patients had received prior docetaxel.
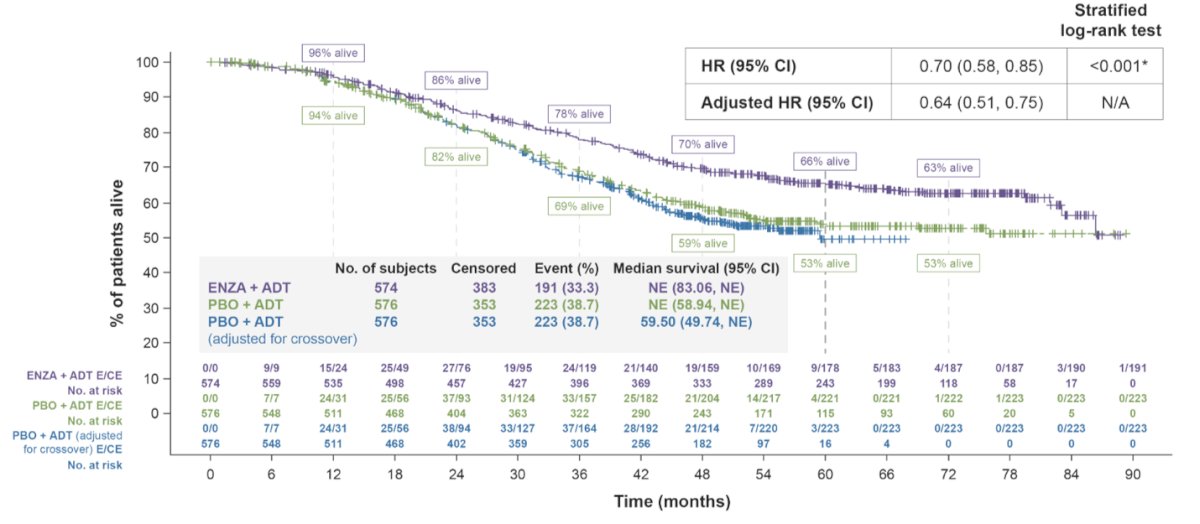
With a median follow-up of 61.4 months (range: 0.03–89.33), enzalutamide plus ADT continued to show a significant overall survival (OS) benefit compared to placebo plus ADT (HR 0.70; 95% CI: 0.58–0.85; P<0.001). A sensitivity analysis, which accounted for the substantial crossover after study-wide unblinding (n = 182, 32%, starting at month 18), confirmed a similar treatment effect (HR 0.64; 95% CI: 0.51–0.75). These findings underscore the long-term survival benefit of ENZA + ADT, even in the context of crossover.
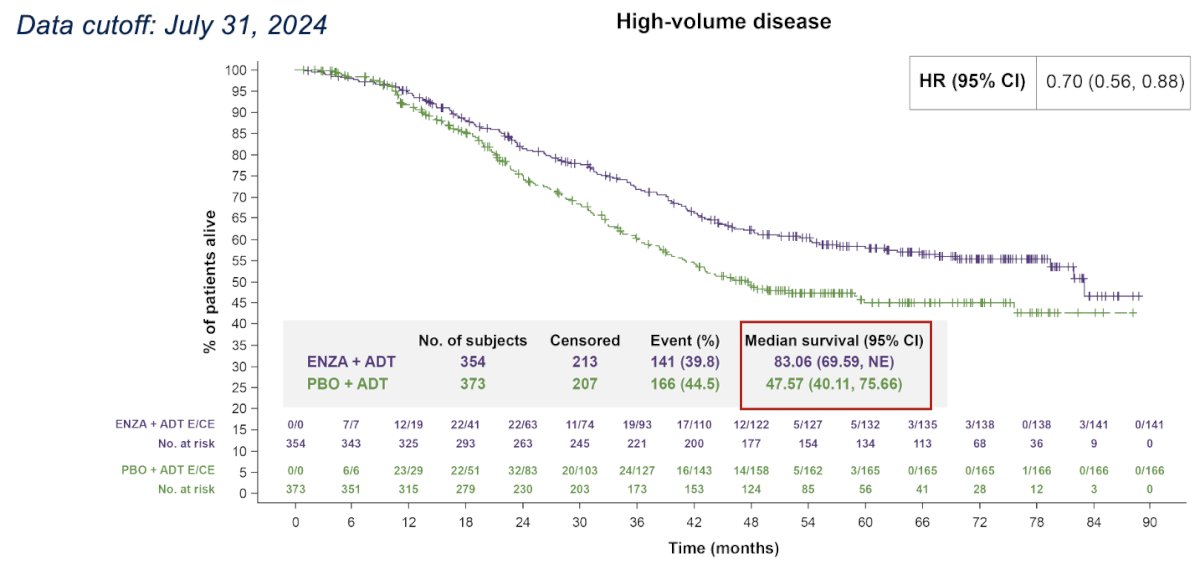
In the subset of patients with high-volume disease, enzalutamide plus ADT demonstrated a substantial overall survival benefit. The median OS in the ENZA + ADT group was 83.0 months, compared to 47.67 months in the placebo + ADT group, representing an extension of approximately 3 years.
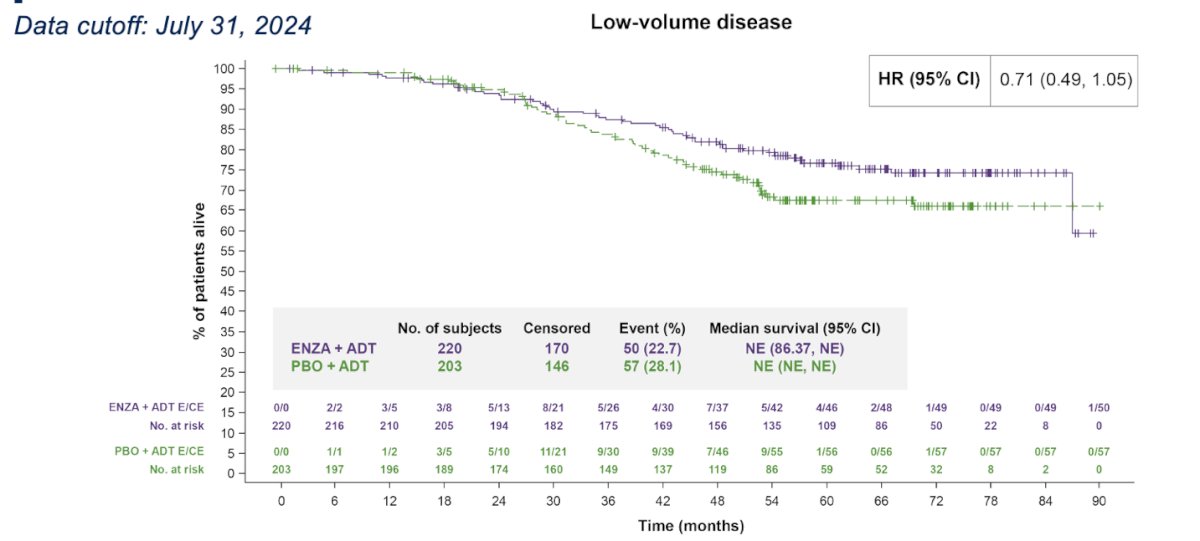
There is no heterogeneity in outcomes by disease volume. Notably, a similar relative improvement in OS in patients with low-volume disease was observed (HR 0.71, 95% CI 0-49, 1.05)
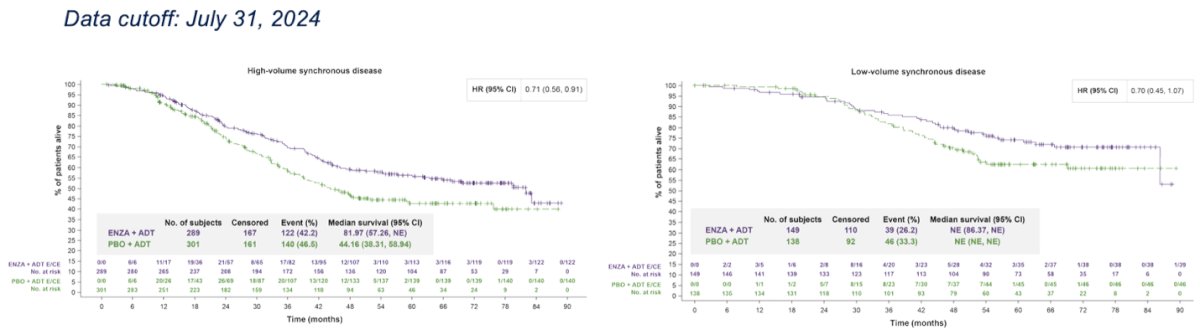
A subgroup analysis of OS by disease volume and timing of metastases showed that treatment with ENZA plus ADT resulted in a substantial survival benefit in patients with high-volume synchronous disease, with a median OS of 82 months compared to 44 months in the placebo group. In patients with low-volume synchronous disease, OS was also longer with ENZA + ADT than with PBO + ADT; however, the confidence interval crossed 1.0, indicating that the survival difference in this subgroup did not reach statistical significance.
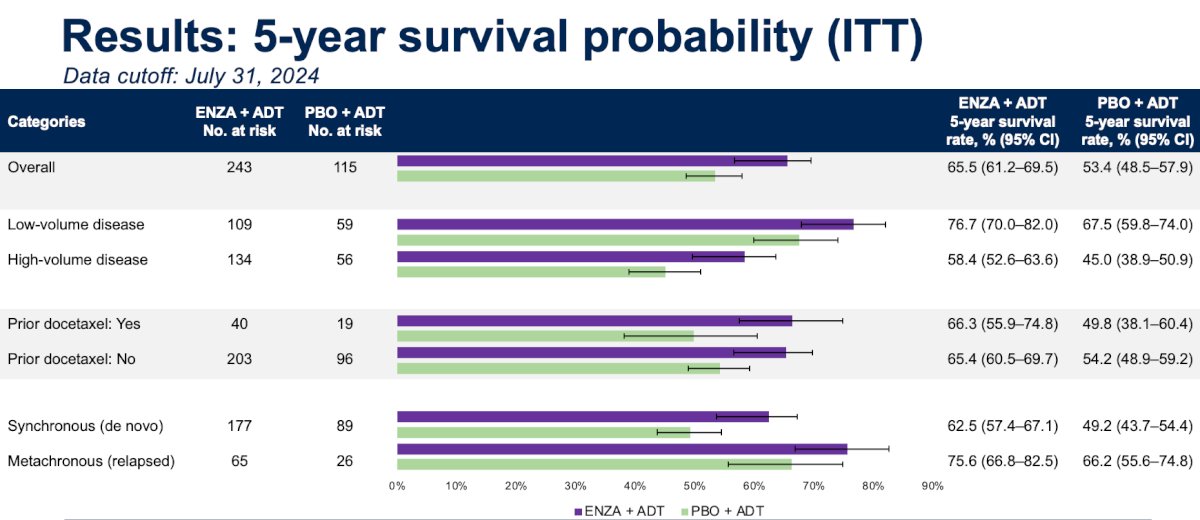
The 5-year survival rate was greater in the ENZA + ADT group vs PBO + ADT group in all clinically relevant subgroups, as shown in the graphic below. Improvement in OS at 5 years ranged from 9% to 17% based on disease volume, prior chemotherapy, and metastatic disease presentation
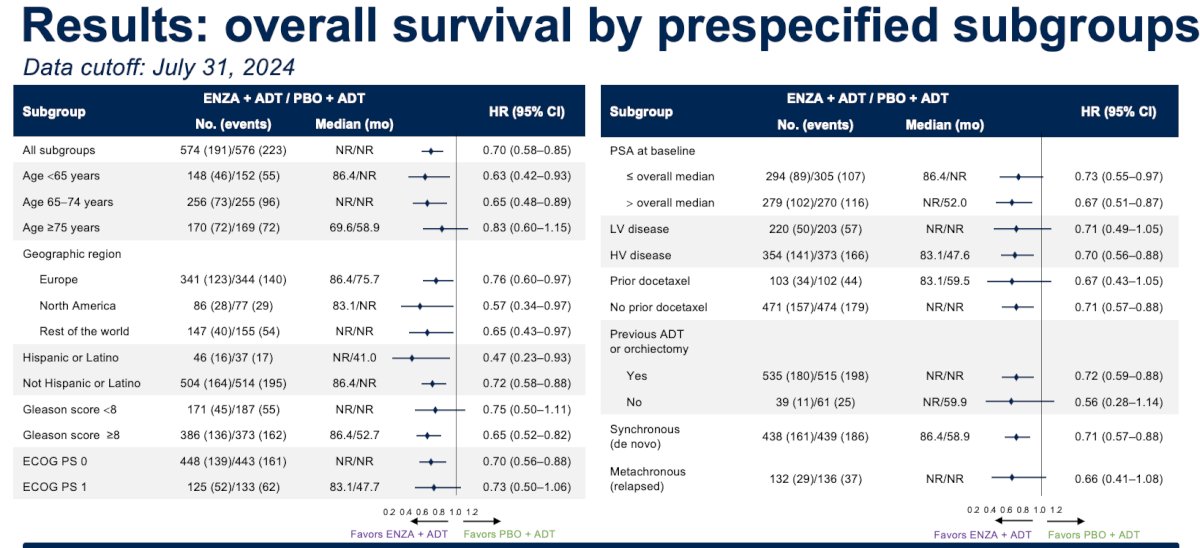
OS treatment benefit with ENZA + ADT was consistent across most prespecified subgroups, as shown in the forest plot below. Dr Armstrong highlighted that there was very little heterogeneity.
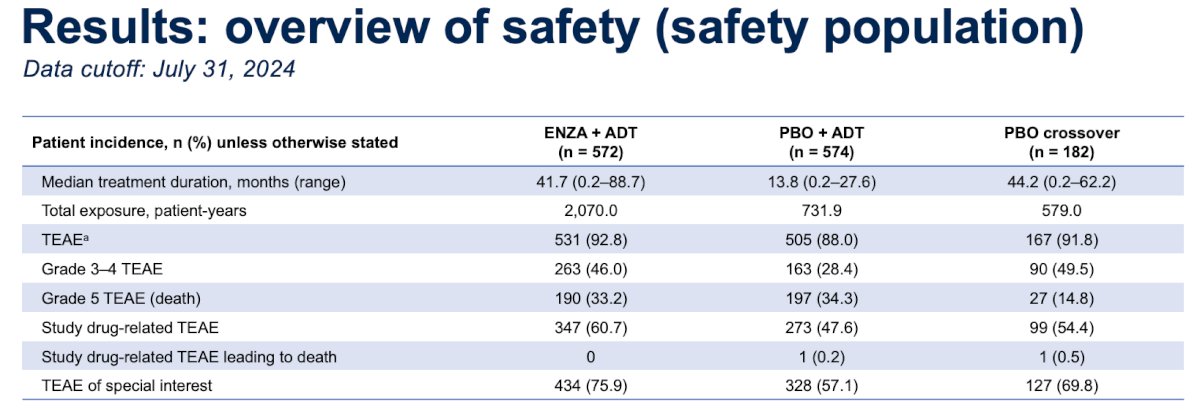
Dr. Armstrong highlighted that the overall incidence of treatment-emergent adverse events (TEAEs) was similar across treatment groups. However, the incidence of grade 3–4 TEAEs, study drug-related TEAEs, and TEAEs of special interest was higher in the ENZA + ADT group compared to the placebo + ADT group. Importantly, the types and frequency of TEAEs of special interest were consistent with previous ARCHES analyses, and no new safety signals were identified with extended follow-up.
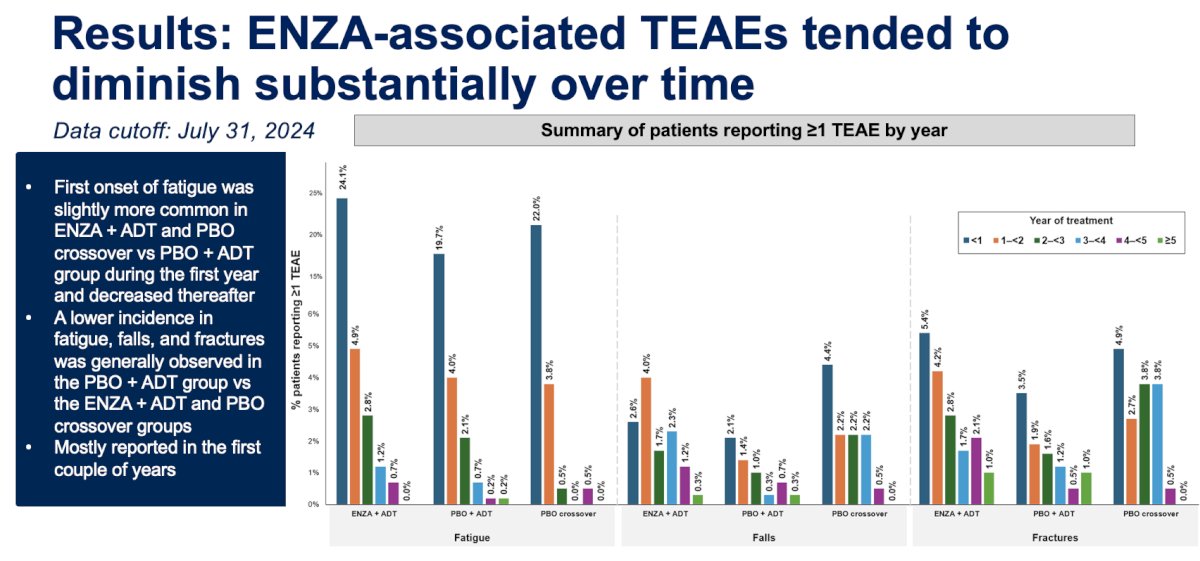
Notably, the first onset of fatigue was slightly more common in the first year and in the ENZA + ADT and placebo crossover groups compared to the placebo + ADT group, particularly during the first year of treatment, with incidence decreasing over time. Additionally, a lower overall incidence of fatigue, falls, and fractures was generally observed in the placebo + ADT group compared to both the ENZA + ADT and crossover groups, with most of these events occurring within the first couple of years of therapy. There was very little onset of these TEAEs in years three to five.
Dr. Armstrong acknowledged several limitations of the 5-year OS analysis. First, the analysis was post hoc and not alpha-protected, meaning all p-values are nominal and should be interpreted with caution. Additionally, in many subgroups, median OS has still not been reached, which, while encouraging for patients, limits mature comparative interpretation. He also noted that the RPSFT model assumes a uniform proportional treatment effect regardless of when enzalutamide is received, which may not hold true particularly if prolonged ADT diminishes the efficacy of ENZA + ADT over time. Lastly, due to operational challenges, some patients in the placebo + ADT group completed the double-blind phase but did not transition into the open-label extension. Instead, they received ENZA + ADT outside the study and were followed only for long-term adverse events and survival status, potentially introducing variability in long-term follow-up data.
Dr. Armstrong concluded the presentation with the following key takeaways from the 5-year follow-up analysis of the ARCHES study:
- Enzalutamide plus ADT was associated with a 66% probability of survival at 5 years and a 30% reduction in the risk of death compared to placebo plus ADT, despite substantial crossover.
- Patients with high-volume disease receiving ENZA + ADT experienced a median overall survival benefit of approximately 3 years compared to those on PBO + ADT. The absolute 5-year survival rate improved by 13% in patients with high-volume disease and by 9% in those with low-volume disease.
- The survival benefit of ENZA + ADT was consistent across key clinical subgroups, including disease volume (high vs low), prior docetaxel use, and timing of metastasis (synchronous vs metachronous), with no evidence of heterogeneity.
- While ENZA use was associated with an increased rate of treatment-related adverse events (TEAEs), the incidence of these events decreased substantially over time, suggesting a more favorable long-term tolerability profile.
These findings represent one of the longest OS follow-up analyses in the mHSPC setting and reinforce the durable benefit of ENZA + ADT, particularly for patients with high-volume disease
Presented by: Andrew J. Armstrong, MD, MS, Duke Cancer Institute Center for Prostate and Urologic Cancers, Duke University School of Medicine.Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Reference: