(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a prostate, testicular, and penile cancers poster session. Dr. Stephen Freedland presented the results of a Veteran Health Administration (VHA) study evaluating the associations between various PSA response measures and clinical outcomes in metastatic castration-sensitive prostate cancer (mCSPC) patients to determine the required duration of treatment.
Clinical trials show that combining ADT with androgen receptor pathway inhibitors (ARPIs) improves PSA response, progression‑free survival, and overall survival (OS), compared to ADT monotherapy, in patients with mCSPC.1–3 There are limited real-world data on the association between PSA response and survival outcomes in patients with mCSPC.4 Dr. Freedland and colleagues used the VHA database to identify which real-world PSA response metrics are best associated with OS and disease progression in patients with mCSPC who initiated first‑line ADT, alone or in combination with other treatments.
VHA data (2017–2024) were analyzed for patients with mCSPC who:
- Initiated the index treatment, i.e., ADT ± other antineoplastic treatments (ARPIs, nonsteroidal antiandrogen [NSAA], docetaxel)
- Had available PSA values at baseline (365 days prior to ADT initiation [index date]) and during index treatment.
A PSA response was defined as:
- ≥90% decline from baseline PSA
- A PSA of <0.2 ng/mL during index treatment.
The primary outcomes were:
- OS
- Time to disease progression, defined as
- PSA progression, i.e., ≥25% rise and ≥2 ng/mL increase from nadir PSA during PSA follow‑up
- Initiation of a new antineoplastic treatment
- Castration resistance
- Death
The follow-up period was the time from the index date to the end of continuous enrollment, death, or the end of data availability (August 31, 2024). Landmark analyses with Cox proportional hazards regression modeling assessed the association of PSA response (within 9 months of initiating ADT) with OS and time to progression after 9 months post-ADT initiation in the overall population.
Overall, 4,890 patients initiated first‑line treatment for mCSPC:
- ADT alone: 47%
- ADT + ARPI: 40%
- ADT + non-steroidal anti-androgen (NSAA): 7.4%
- ADT + docetaxel (± NSAA): 3.8%
- ADT + ARPI + docetaxel (± NSAA): 2%
The median age was 74 years (IQR:69-80). 58% of patients identified as non-Hispanic White and 29% as Black. The median follow-up was 24.7 months, with a median PSA follow-up during index treatment of 14.6 months.
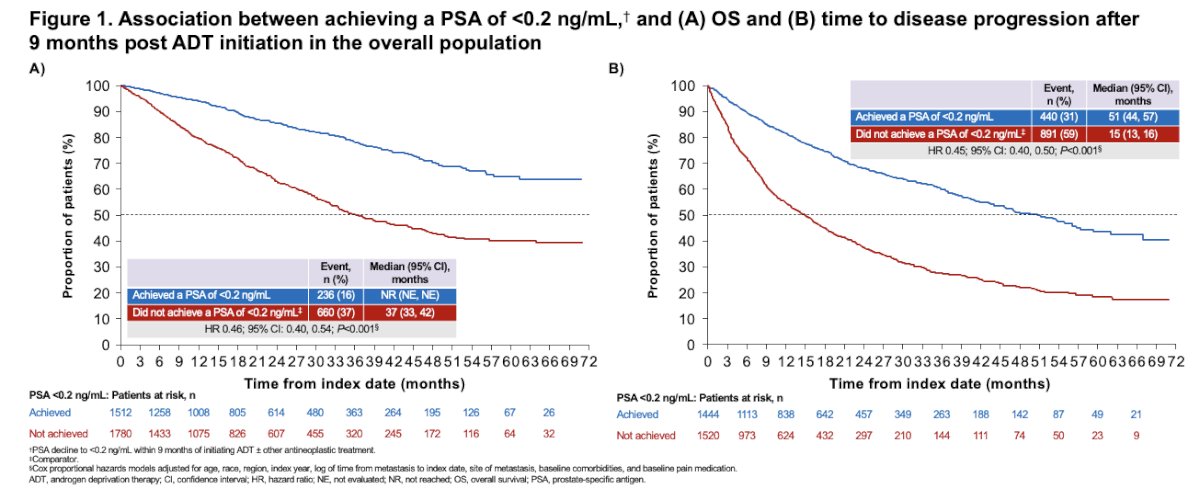
During PSA follow-up, 44% of patients reached a PSA of <0.2 ng/mL, and 74% had a ≥90% PSA decline. In the overall population, achieving a PSA of <0.2 ng/mL within 9 months of initiating ADT was significantly associated with reductions in the risk of death (54%) and disease progression (55%) after 9 months post-ADT initiation.
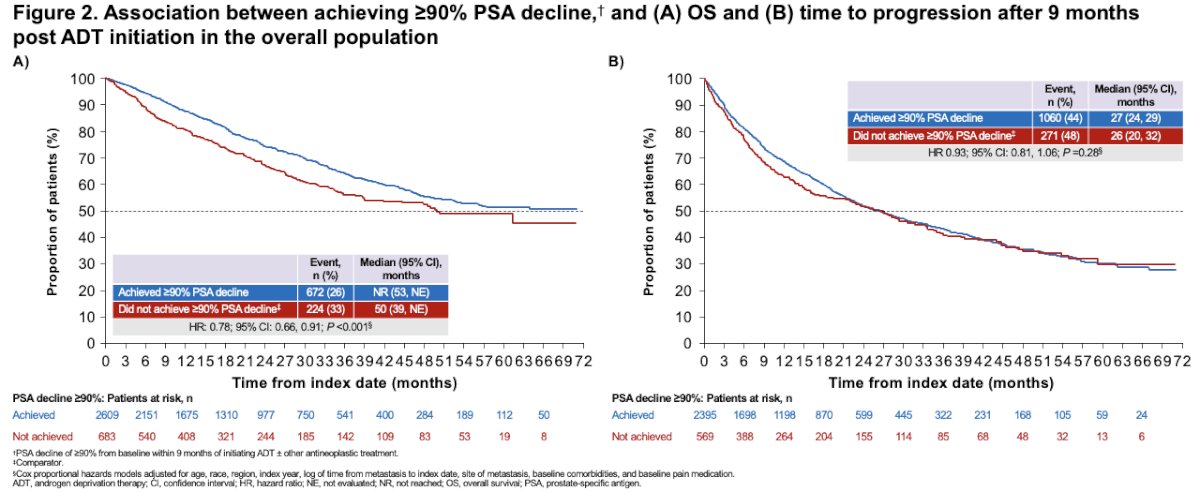
Achieving ≥90% PSA decline was associated with a 22% reduced risk of death but was unrelated to disease progression.
Compared with patients who initiated ADT alone, those who initiated ADT + ARPI were more likely to achieve a PSA of <0.2 ng/mL, both within 9 months of initiating index treatment and during PSA follow-up (while receiving index treatment).

Dr. Freedland concluded as follows:
- mCSPC patients who achieved a PSA of <0.2 ng/mL by 9 months after initiating ADT ± other treatments had lower risk of death (hazard ratio [HR] 0.46; 95% confidence interval [CI]: 0.40–0.54) and disease progression (HR 0.45; 95% CI: 0.40–0.50) after 9 months post-ADT initiation, compared with patients who did not.
- Reaching a ≥90% PSA decline was modestly associated with improved OS (HR 0.78; 95% CI: 0.66, 0.91), but not disease progression (HR 0.93; 95% CI: 0.81, 1.06).
- These results suggest a PSA nadir of <0.2 ng/mL is needed for optimal clinical outcomes.
- Patients treated with ADT + ARPIs were more likely to achieve a PSA nadir of <0.2 ng/mL, compared to those treated with ADT alone.
Presented by: Stephen Freedland, MD, Professor, Department of Urology, Cedars Sinai Hospital, Los Angeles, CA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: PSA Thresholds in mHSPC: What VA Data Reveals About Optimal Targets - Stephen Freedland
- Armstrong AJ, Szmulewitz RZ, Petrylak DP, et al. ARCHES: A randomized, phase III study of androgen deprivation therapy with enzalutamide or placebo in men with metastatic hormone-sensitive prostate cancer. J Clin Oncol. 2019;37(32):2974–2986.
- Armstrong AJ, Azad A, Iguchi T, et al. Efficacy and safety of enzalutamide plus androgen deprivation therapy in high- and low-volume metastatic hormone-sensitive prostate cancer: post hoc analysis of the ARCHES trial. J Clin Oncol. 2022;40(15):1616–1622.
- Davis ID, Martin AJ, Stockler MR, et al. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N Engl J Med. 2019;381(2):121–131.
- Gebrael G, Shea M, Taplin ME, et al. Management of metastatic castration-sensitive prostate cancer in the era of combination systemic therapy: a contemporary perspective. Prostate Cancer Prostatic Dis. 2024;27(2):279–282.