(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a New Frontiers in Prostate-Specific Membrane Antigen (PSMA) Radioligand Therapy. Dr. Bastiaan Privé presented the BULLSEYE trial of 177Lu-PSMA-617 in oligo-metastatic hormone sensitive prostate cancer (omHSPC).
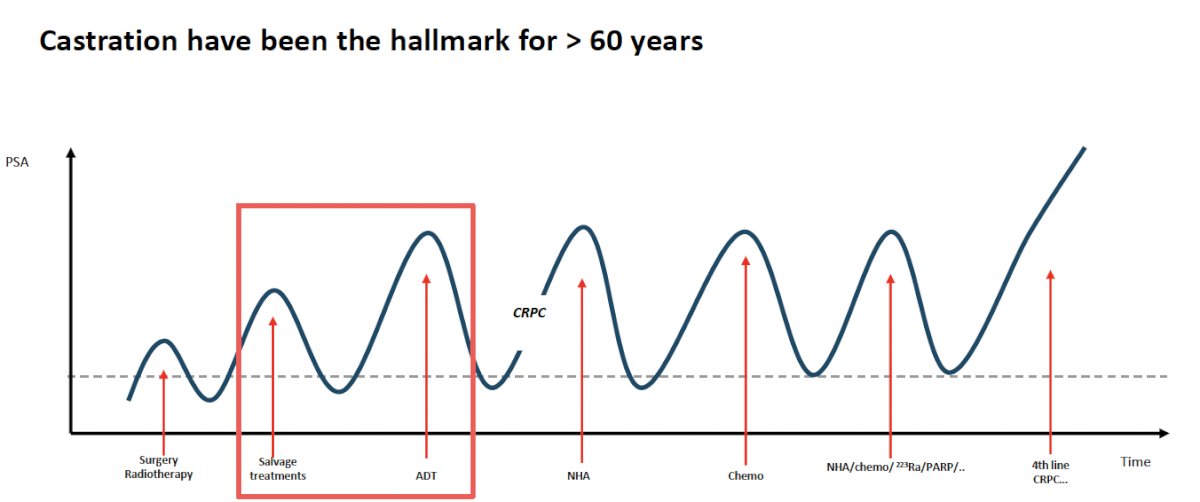
Twenty-seven to 53% of prostate cancer patients receiving primary local therapy (surgery or radiotherapy) eventually experience disease recurrence. Dr. Privé noted that medical or surgical castration has been the ‘hallmark’ treatment for >60 years.
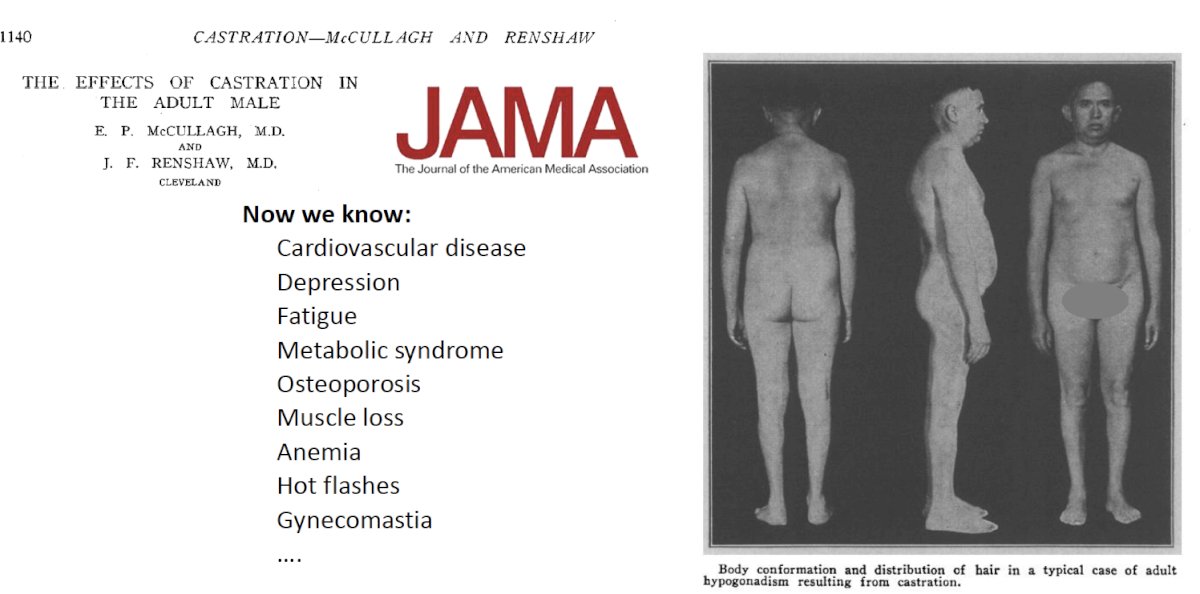
However, castration is associated with known adverse effects, as highlighted below:
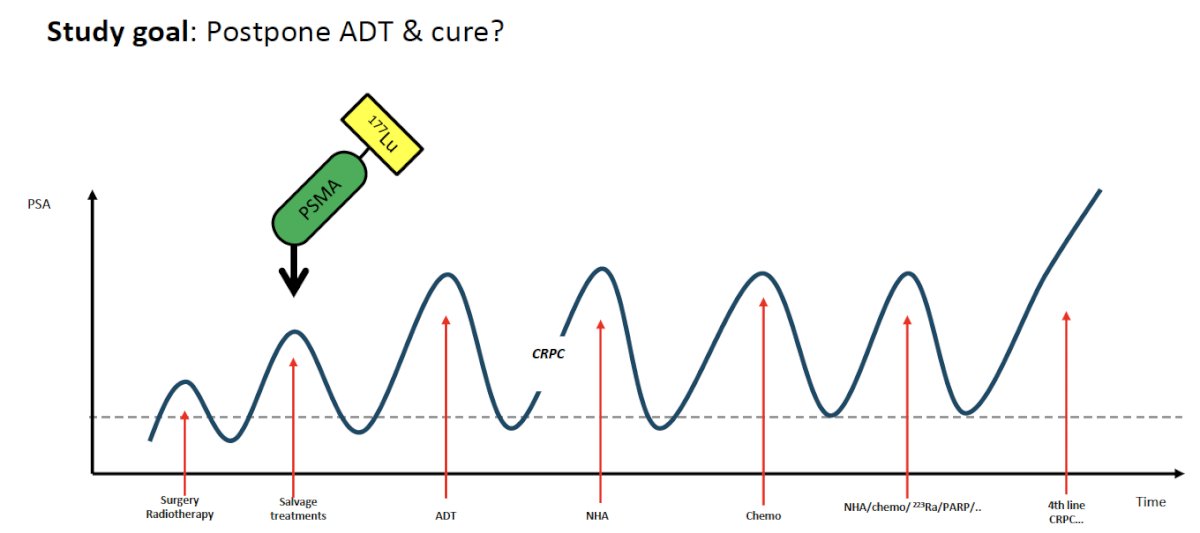
As such, Dr. Privé and colleagues investigated whether a novel agent that does not induce castration (e.g., 177Lu-PSMA-617) could be alternatively used in this setting?
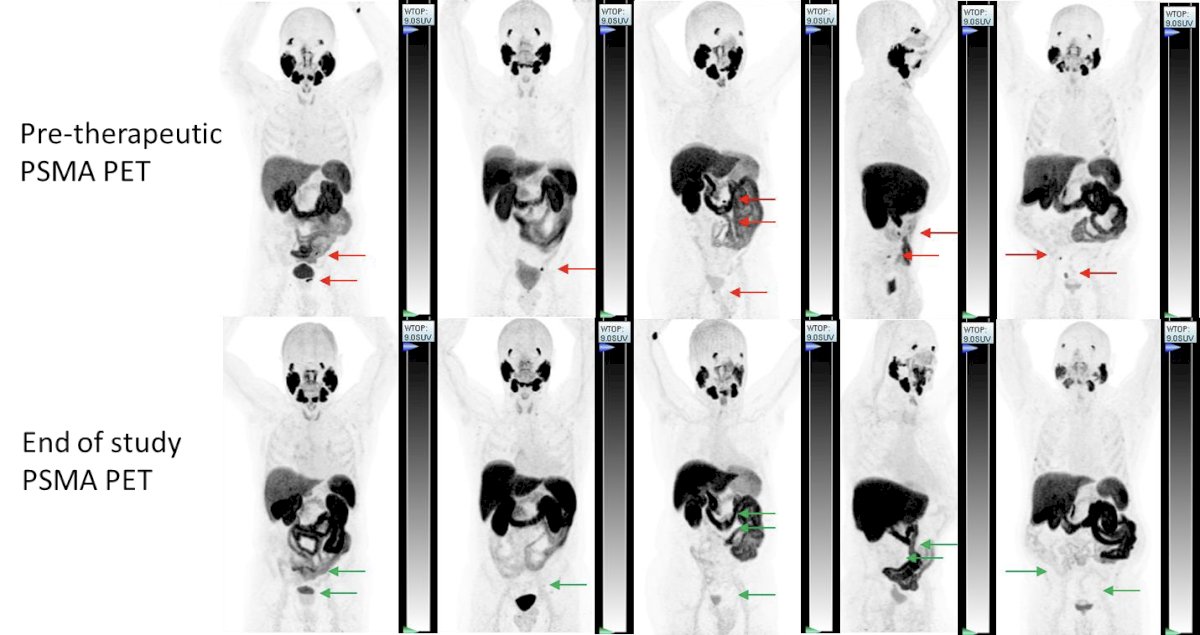
In 2021, Dr. Privé and colleagues published the results of a phase I dosimetry study of two cycles of 177Lu-PSMA-617 (3 GBq + 6 GBq) in 10 patients with progressive mHSPC following local treatment and who had ≤10 metastatic lesions on a 68Ga-PSMA-11-PET/CT with a PSA doubling time <6 months. Whole-body SPECT/CT and blood dosimetry was performed to calculate doses to the tumors and organs at risk (OAR). All patients received two cycles of 177Lu-PSMA-617 without complications. No treatment-related grade III-IV adverse events were observed. According to dosimetry, none of the OAR reached threshold doses for radiation-related toxicity. Moreover, all target lesions received a higher radiation dose than the OAR. All 10 patients showed altered PSA kinetics, postponed androgen deprivation therapy (ADT), and maintained good quality of life. Half of the patients showed a PSA response of more than 50%.2
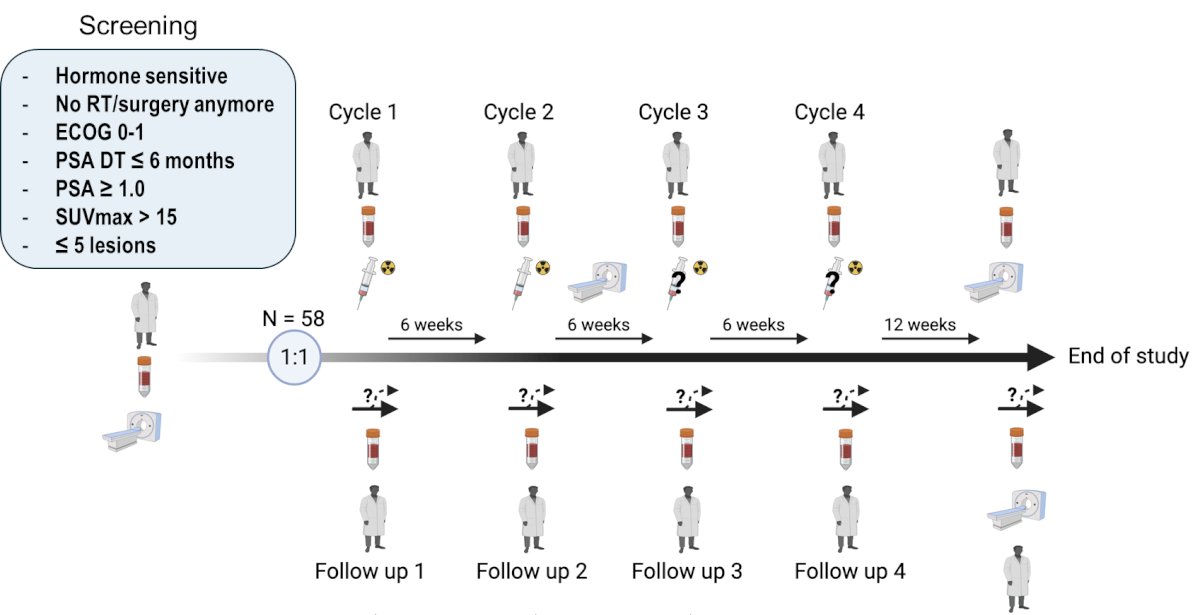
Building off the results of this phase I trial, Dr. Privé and colleagues designed the BULLSEYE trial, an international, open label, randomized trial of 2 (+2) cycles of 7.4 GBq 177Lu-PSMA-617 versus ‘standard of care’ of watchful waiting (i.e., postponing ADT). The study included 58 patients who were randomized 1:1 to the intervention and control arms. Eligible patients were those with:
- Hormone sensitive disease
- Not eligible/ideal candidates for further pelvic radiotherapy or surgery
- PSA doubling time ≤6 months
- PSA ≥1
- SUVmax >15
- ≤5 lesions
The primary study objective was disease progression, defined as a 100% increase in serum PSA levels or radiographic or clinical progression. The secondary study objectives were:
- PSA progression (utilizing the Phoenix criteria)
- PSA response
- Adverse events
- Quality of life
- Outcomes of the patients in the control arm that received 177Lu-PSMA-617
- Patients in the control arm were allowed to receive [177Lu]Lu-PSMA-617 upon reaching the primary endpoint

The trial schema with screening/follow up visits is illustrated below:
The baseline characteristics by study arm are summarized in the table below. The median patient age was 69–72 years. Almost 50% of patients had previously received both surgery (i.e., radical prostatectomy) and radiotherapy. 14-17% of patients had received prior ADT. 30–38% of patients had Gleason Score ≥8 disease. The median baseline PSA was 3.8–5.4 ng/ml. The median PSA doubling time was 3.4–3.8 months.

The study flow chart is summarized below:

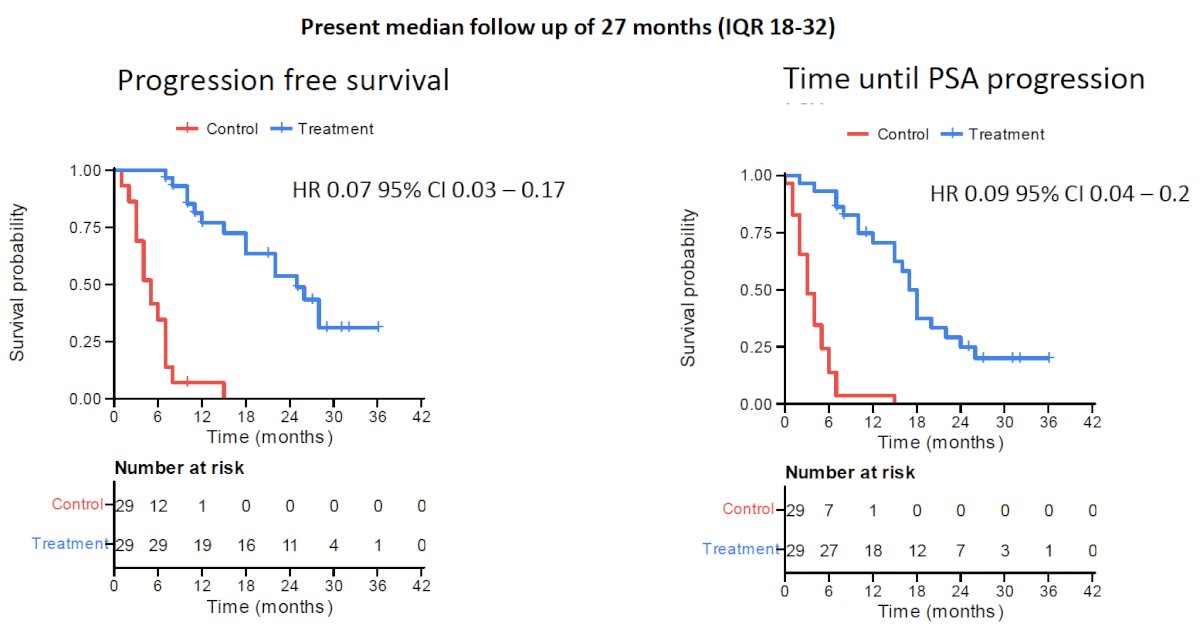
At a median follow-up of 27 months, both progression-free survival (HR: 0.07, 95% CI: 0.03–0.17) and time until PSA progression (HR: 0.09, 95% CI: 0.04–0.2) favored the treatment arm:
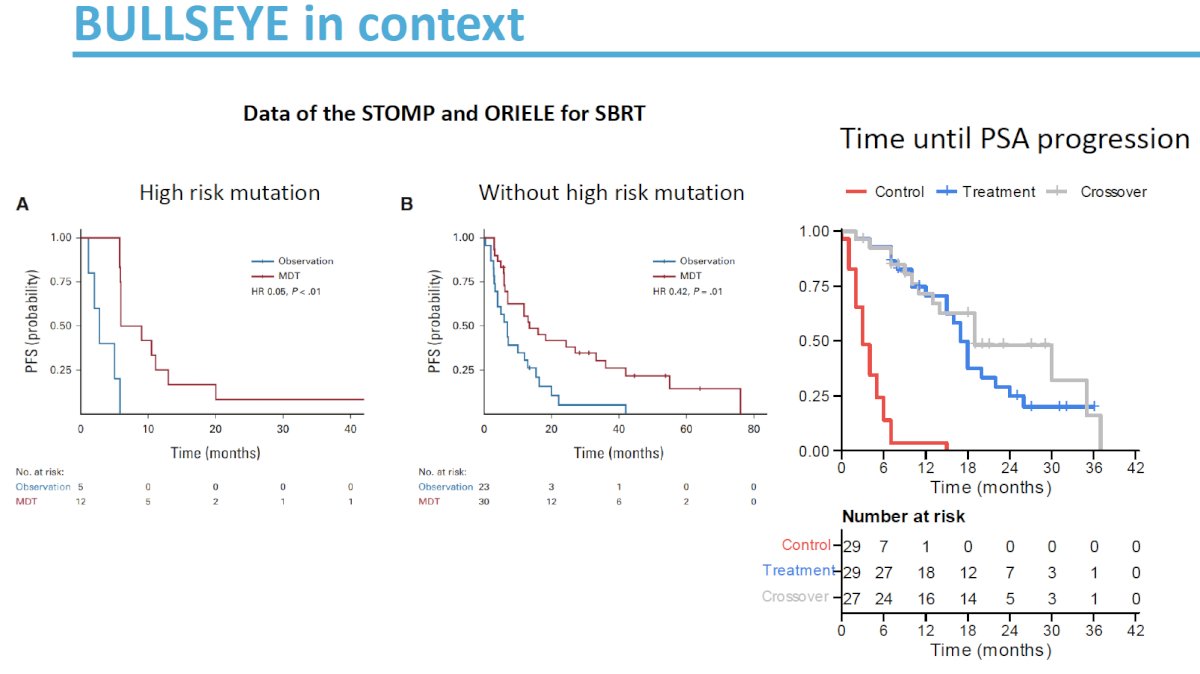
Notably, however, when patients in the control arm crossed over to receive 177Lu-PSMA-617 at time of progression, there was no difference in progression-free survival or time to PSA progression, with time of starting 177Lu-PSMA-617 therapy considered the T0.

He noted that these results are comparable, if not slightly better, to those observed in the STOMP and ORIOLE trials of stereotactic body radiotherapy (SBRT).3,4
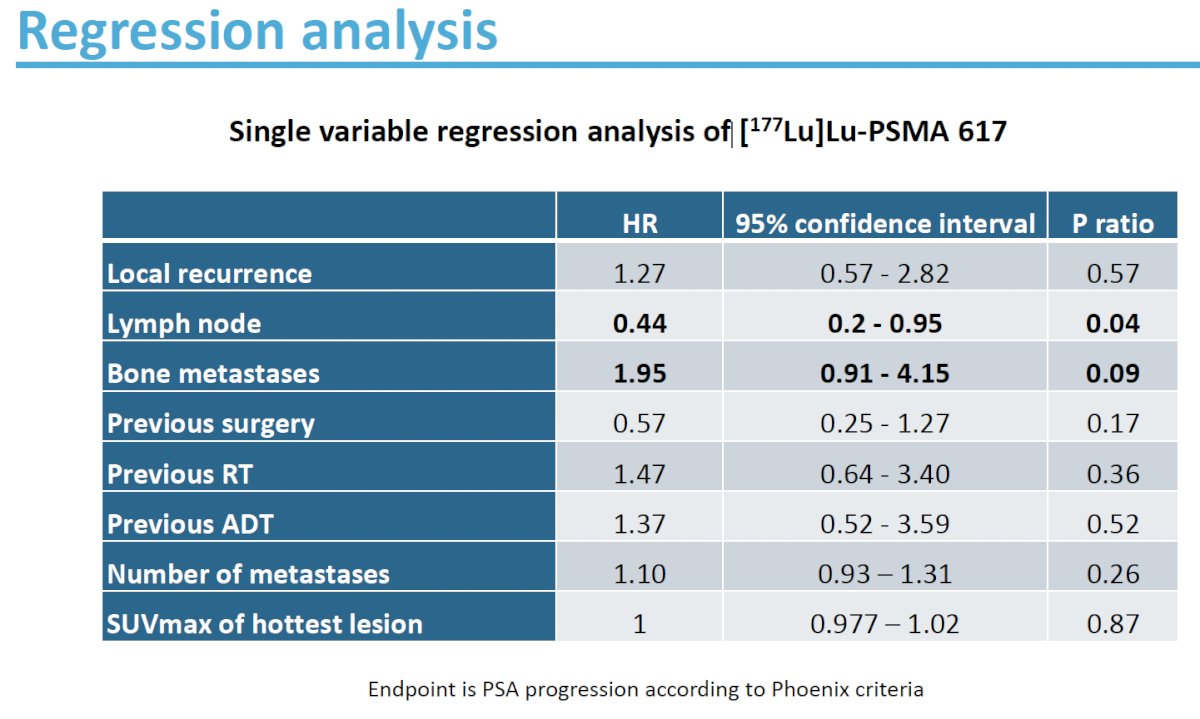
On regression analysis, patients with bone metastases had worse time to PSA progression (HR: 1.95, p=0.09), whereas those with nodal-only metastases had superior survival outcomes (HR: 0.44, p=0.04).
Overall, 14/56 (25%) of patients receiving 177Lu-PSMA-617 had a complete biochemical response. 9/56 (16%) had a PSA <0.1 ug/L at data cut-off.
The adverse event profile was consistent with that of 177Lu-PSMA-617 therapy. The most common grade 1-2 adverse events were dry mouth, fatigue, nausea, and lymphopenia. Four patients (7%) had grade 3 lymphopenic events and one patient experience grade 3 eye dryness. No grade 4 events were observed.

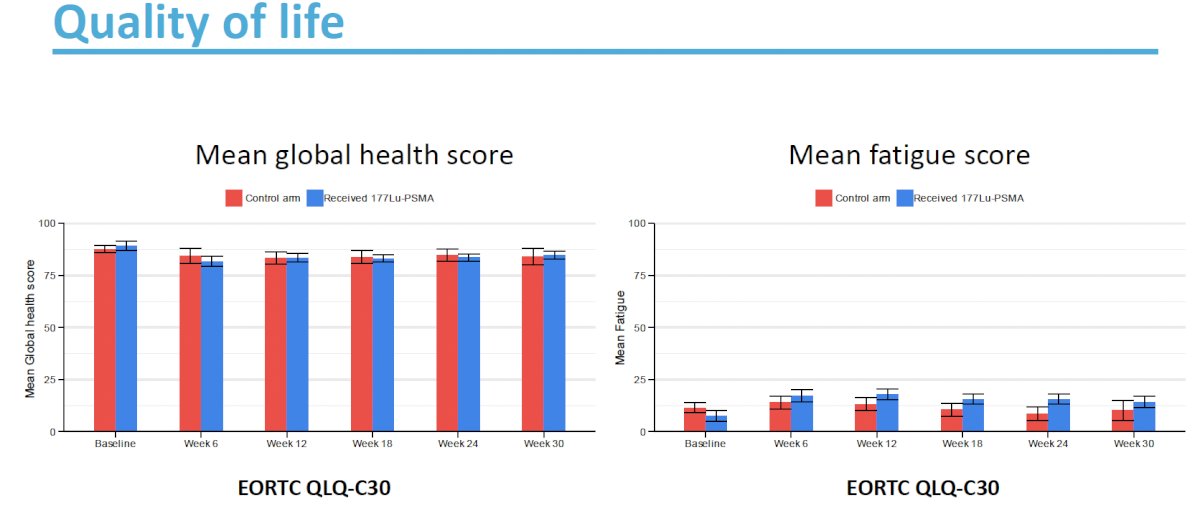
Quality of life outcomes (mean global health score and mean fatigue score) were comparable between the two study arms.
Dr. Privé concluded as follows:
- PSMA radioligand therapy is a promising novel treatment option for patients with oligorecurrent, hormone-sensitive prostate cancer.
- In this group of high-risk, oligorecurrent, hormone-sensitive prostate cancer, delaying 177Lu-PSMA-617 therapy until evidence of disease progression appears to be safe and effective
- The side effects of 177Lu-PSMA-617 therapy were overall mild in nature, and patients retained good quality of life
- No safety signals that would limit future treatment with 177Lu-PSMA-617 therapy were observed. However, long term toxicity needs to be evaluated.
Presented by: Bastiaan M. Privé, MD, PhD, Radboud University Medical Centre (Radboudumc), Nijmegen, Netherlands
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:- Conford P, Bellmunt J, Bolla M, et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part II: Treatment of Relapsing, Metastatic, and Castration-Resistant Prostate Cancer. Eur Urol. 2017; 71(4): 630-642.
- Privé BM, Peters SMB, Muselaers CH, et al. Lutetium-177-PSMA-617 in Low-Volume Hormone-Sensitive Metastatic Prostate Cancer: A Prospective Pilot Study. Clin Cancer Res. 2021; 27(13): 3595-601.
- Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol. 2020; 6(5): 650-659.
- Ost P, Reynders D, Decaestecker K, et al. Surveillance of metastasis-directed therapy for oligometastatic cancer recurrence: A prospective, randomized, multicenter phase II trial. J Clin Oncol. 2018; 36(5): 446-453.