(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to the Poster Session: Genitourinary Cancer - Prostate, Testicular, and Penile Cancer. Dr. Stephen J. Freedland presented Poster 5103: Secondary outcomes by prior definitive treatment (tx) in patients (pts) with high-risk biochemically recurrent prostate cancer (hrBCR) treated with enzalutamide (enza) monotherapy (mono): EMBARK post hoc analysis.
The phase 3 EMBARK trial demonstrated clinically meaningful improvements in several key secondary efficacy endpoints with enzalutamide monotherapy compared to leuprolide alone in patients with high-risk biochemical recurrence. These included improvements in metastasis-free survival (MFS), time to PSA progression, time to first use of new antineoplastic therapy, and overall survival. Additional secondary endpoints—such as time to distant metastasis, time to symptomatic progression, and time to first symptomatic skeletal event—also favored enzalutamide monotherapy.1
Interestingly, time to resumption of any hormonal therapy after treatment suspension was longer with leuprolide alone compared to enzalutamide monotherapy, suggesting a longer treatment-free interval in the leuprolide arm.1,2 In subgroup analyses, the MFS benefit with enzalutamide monotherapy over leuprolide was preserved among patients who had received prior radiation therapy (RT).3 However, among those without prior RT, the event rates were low, limiting the ability to draw definitive conclusions regarding MFS differences between treatment arms. (3)
Patients enrolled in the phase 3 EMBARK trial (NCT02319837) had high-risk biochemical recurrence defined as a PSA doubling time of ≤9 months and a PSA level of ≥2 ng/mL above nadir following primary radiotherapy, or ≥1 ng/mL following primary radical prostatectomy (RP) with or without postoperative RT.1
A total of 1,068 patients were randomized in a 1:1:1 ratio to receive enzalutamide plus leuprolide (n=355), leuprolide alone (n=358), or enzalutamide monotherapy (n=355). This analysis focused on secondary endpoints comparing enzalutamide monotherapy with leuprolide alone. Endpoints included:
- Time to PSA progression
- Time to first use of new antineoplastic therapy
- Time to distant metastasis
- Time to resumption of any hormonal therapy following treatment suspension
- Time to symptomatic progression.
The secondary endpoint of time to first symptomatic skeletal event was excluded from this analysis due to the limited number of events in the overall population. Post hoc subgroup analyses evaluated these secondary efficacy outcomes by prior definitive treatment, categorized as RP only, RT only, or RP + RT.
Dr Freedland highlighted that they used Cox regression models to assess the interaction between treatment arm and prior definitive treatment status for each endpoint. Each model included terms for treatment, prior definitive therapy, and the interaction between the two. The P interaction value for each endpoint was derived from a joint test evaluating the significance of the interaction effect.
Notably, in both treatment arms: enzalutamide monotherapy and leuprolide alone, the majority of patients had received prior radical prostatectomy plus radiotherapy, comprising 47% and 50% of each group, respectively. Secondary efficacy outcomes comparing enzalutamide monotherapy versus leuprolide alone across all prior definitive treatment subgroups are summarized in the table below. Across subgroups, enzalutamide monotherapy improved time to distant metastasis (Pinteraction=0.65) and time to symptomatic progression (Pinteraction=0.59) compared to leuprolide alone. Conversely, time to resumption of any hormonal therapy after treatment suspension favored leuprolide alone over enzalutamide monotherapy (Pinteraction=0.18).
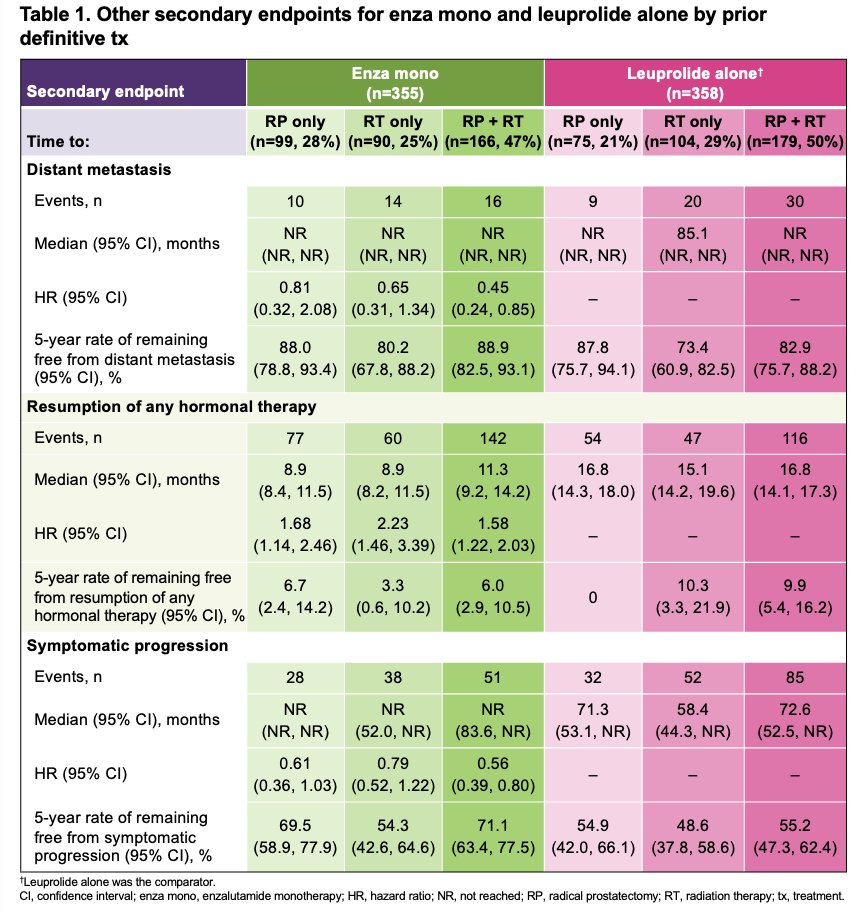
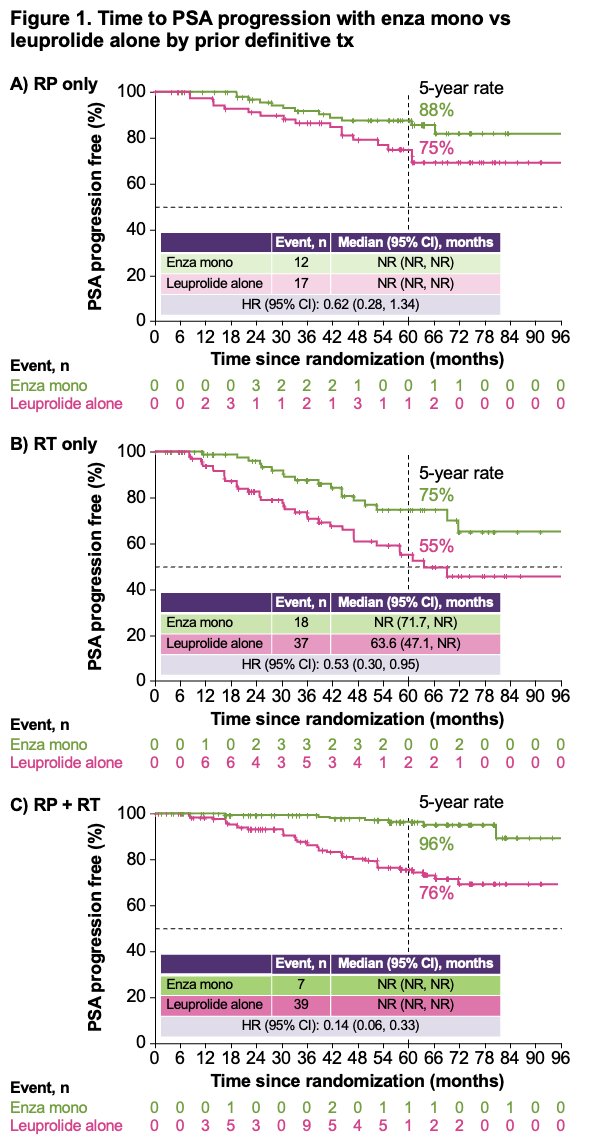
Dr. Freedland highlighted that, regardless of prior definitive treatment, enzalutamide monotherapy prolonged key secondary endpoints, including time to PSA progression compared to leuprolide alone (Pinteraction=0.07) as illustrated in the figures below.
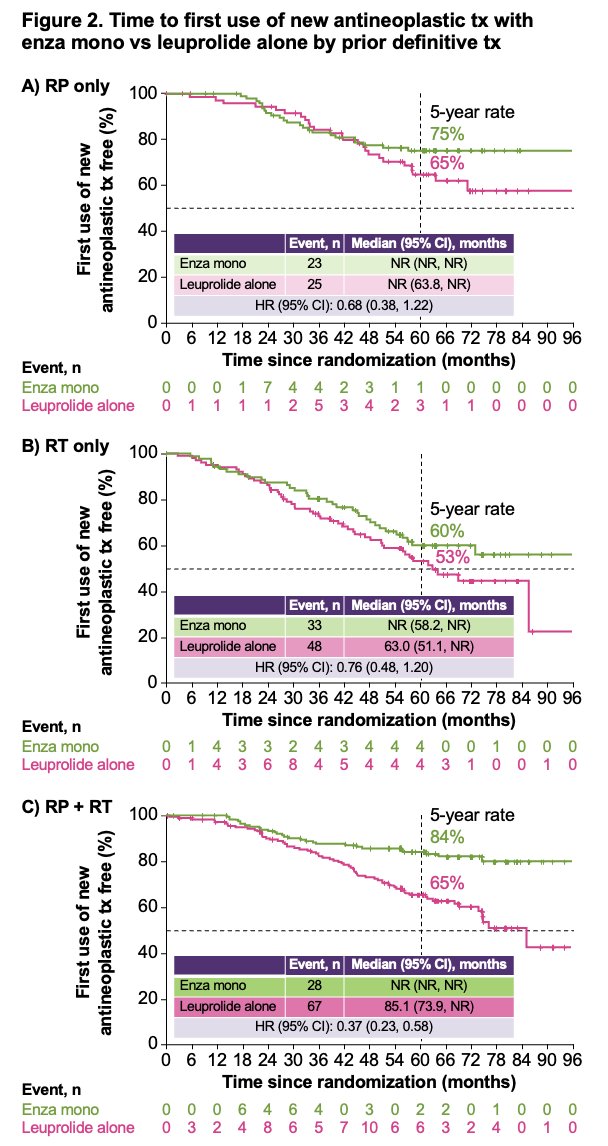
Moreover, similar outcomes were observed for the secondary endpoint of time to first use of new antineoplastic therapy, with enzalutamide monotherapy demonstrating a delay compared to leuprolide alone (Pinteraction=0.13).
Dr. Freedland concluded with the following key messages:
- Across all prior definitive treatment subgroups, enzalutamide monotherapy improved:
- Time to PSA progression (Pinteraction=0.07)
- Time to first use of new antineoplastic therapy (Pinteraction=0.13)
- Time to distant metastasis (Pinteraction=0.65)
- Time to symptomatic progression (Pinteraction=0.59)
- Time to resumption of any hormonal therapy after treatment suspension favored leuprolide alone over enzalutamide monotherapy (Pinteraction=0.18) across all subgroups.
- The nonsignificant interaction terms (Pinteraction>0.05) suggest that prior definitive treatment did not modify treatment effects, supporting the clinical benefit of enzalutamide monotherapy across treatment histories.
- Small sample sizes in nonrandomized subgroups and low event numbers should be taken into account when interpreting these findings.
Presented by: Stephen J. Freedland, MD, Department of Urology, Samuel Oschin Comprehensive Cancer Institute, Cedars-Sinai Medical Center. Los Angeles, CA.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: EMBARK Subgroup Analysis: Enzalutamide Monotherapy Effective Regardless of Prior Definitive Therapy - Stephen Freedland
- Freedland SJ, de Almeida Luz M, De Giorgi U, Gleave M, Gotto GT, Pieczonka CM, Haas GP, Kim CS, Ramirez-Backhaus M, Rannikko A, Tarazi J, Sridharan S, Sugg J, Tang Y, Tutrone RF Jr, Venugopal B, Villers A, Woo HH, Zohren F, Shore ND; EMBARK Study. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med. 2023 Oct 19;389(16):1453-1465. doi: 10.1056/NEJMoa2303974. PMID: 37851874.
- De Giorgi U, Freedland SJ, Rannikko A, Ramirez-Backhaus M, Villers A, Tarazi J, Tang Y, Haas GP, Rosales M, Shore ND. Enzalutamide in patients with high-risk biochemically recurrent prostate cancer according to the European Association of Urology definition: a post hoc analysis of EMBARK. Prostate Cancer Prostatic Dis. 2025 Mar 26. doi: 10.1038/s41391-025-00959-8. Epub ahead of print. PMID: 40140551.
- LBA02-09 EMBARK: A Phase 3 Randomized Study of Enzalutamide or Placebo Plus Leuprolide Acetate and Enzalutamide Monotherapy in High-risk Biochemically Recurrent Prostate Cancer. J Urol. 2023 Jul;210(1):224-226. doi: 10.1097/JU.0000000000003518. Epub 2023 May 2. PMID: 37119051.