(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to the Session New Frontiers in Prostate-Specific Membrane Antigen Radioligand Therapy. Dr. Jeremie Calais delivered a presentation titled: Radioligand Therapy Remix: Finding the Right Patient for the Perfect Track.
Dr. Calais opened his presentation by emphasizing that the variability in patient responses to Lutetium-PSMA therapy reflects the underlying biological heterogeneity of metastatic prostate cancer. He proposed that distinct patterns of response should be recognized and interpreted in clinical context. For instance, immediate progression following the first cycle may raise the question of whether treatment was initiated too late or whether LuPSMA is triggering a biological effect. Continuous progression after the second cycle may suggest true resistance to therapy, while eventual acquired resistance or flare phenomena should also be considered. Dr. Calais underscored the importance of understanding and accurately interpreting PSMA imaging response patterns during Lutetium-PSMA therapy to better guide clinical decision-making.

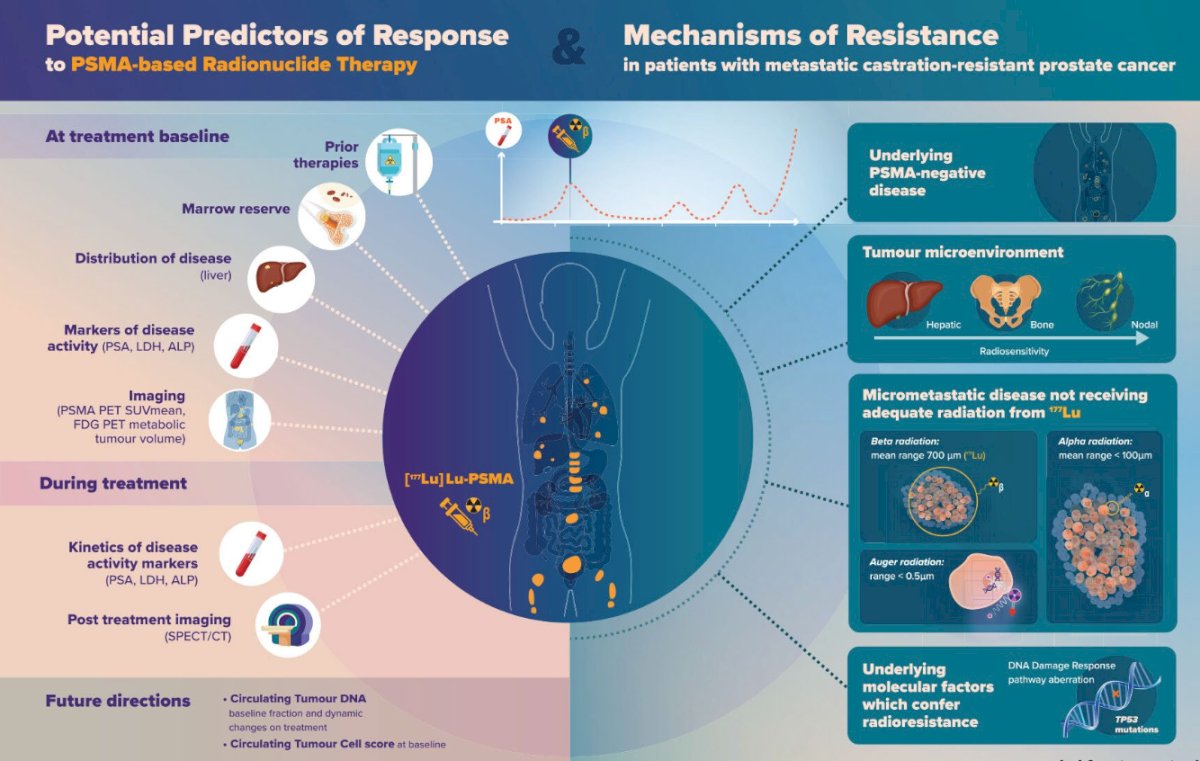
Potential predictors of response to PSMA-based radioligand therapy (RLT) are multifactorial and reflect both disease biology and treatment context. These include prior therapies received, bone marrow reserve, disease distribution, and established markers of tumor burden. Imaging biomarkers such as PSMA PET SUVmean, along with kinetics of disease activity markers and post-treatment imaging (e.g., SPECT/CT), may provide further predictive insights.
Importantly, clinicians should remain mindful of potential mechanisms of resistance. These may include the presence of PSMA-negative tumor clones, a tumor microenvironment that influences radiosensitivity, micrometastatic disease not receiving adequate radiation dose from 177Lu-PSMA, or underlying molecular features such as defects in DNA damage repair pathways that may contribute to radioresistance, as illustrated below.
Dr. Calais noted key limitations of PSMA PET imaging, particularly its reduced sensitivity in detecting small-volume or microscopic disease due to the partial volume effect. This limitation is especially relevant in the context of pelvic nodal metastases. He highlighted that, when compared to histopathology, the sensitivity of PSMA PET for detecting pelvic lymph node metastases is less than 40%. Additional limitations of PSMA PET include its spatial resolution and inability to fully capture target expression heterogeneity. While PSMA PET can illustrate inter-lesion heterogeneity showing differences in PSMA expression between metastatic sites it cannot reliably assess intra-lesion variability. As a result, subtle or heterogeneous expression within individual lesions may go undetected, potentially impacting therapeutic planning and response assessment.2
Although PSMA PET is currently the most sensitive imaging modality available for prostate cancer, it is not without limitations. As Dr. Calais remarked, “PSMA PET is the best—but still not perfect.” A key unmet need remains in its limited ability to detect micrometastatic disease, which may fall below the spatial resolution threshold of PET imaging.
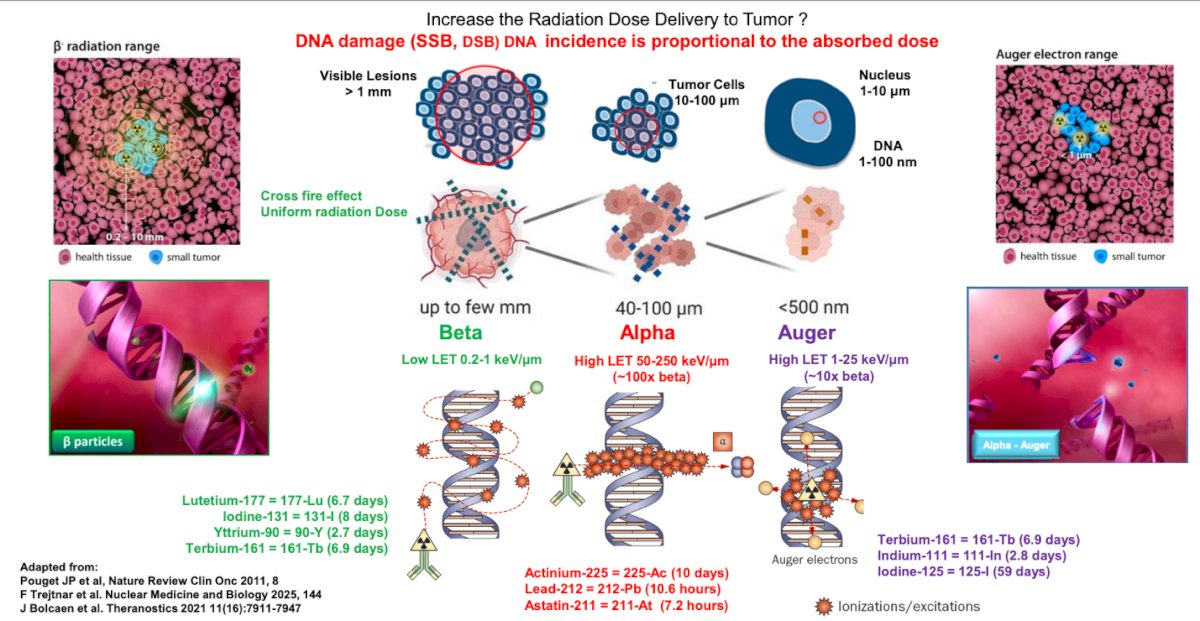
Dr Calais highlighted that there is a potential for optimizing radiation dose delivery to tumors by selecting radionuclides with distinct radiation properties. DNA damage, particularly single-strand breaks (SSBs) and double-strand breaks (DSBs), is directly proportional to the absorbed radiation dose. Three types of radiation particles are available: beta particles (e.g., Lutetium-177, Yttrium-90), alpha particles (e.g., Actinium-225, Lead-212), and Auger electrons (e.g., Terbium-161, Indium-111). Beta emitters have a low linear energy transfer (LET) and penetrate up to a few millimeters, creating a uniform "crossfire" effect suited for visible lesions. Alpha emitters exhibit high LET and deliver intense, localized damage within 40–100 μm, approximately 100 times the LET of beta particles, making them highly effective against clusters of tumor cells. Auger emitters deposit energy over submicron distances (<500 nm), with intermediate LET values, potentially targeting single cells or micrometastases.
The importance of micro-biodistribution and micro-dosimetry is especially pronounced in the context of alpha and Auger-emitting radionuclides, as their radiobiological effects are highly dependent on cellular geometry and proximity to the nucleus. Due to the short range and high linear energy transfer (LET) of these particles, precise localization at the subcellular level is critical to achieve tumoricidal activity while minimizing off-target damage. This raises important considerations regarding potential toxicity to normal tissues with high PSMA expression or absorbed doses during radioligand therapy, particularly the kidneys, parotid glands, and submandibular glands. Further refinement in micro-dosimetry and targeted delivery is essential to maximize efficacy while mitigating risks in these sensitive organs.
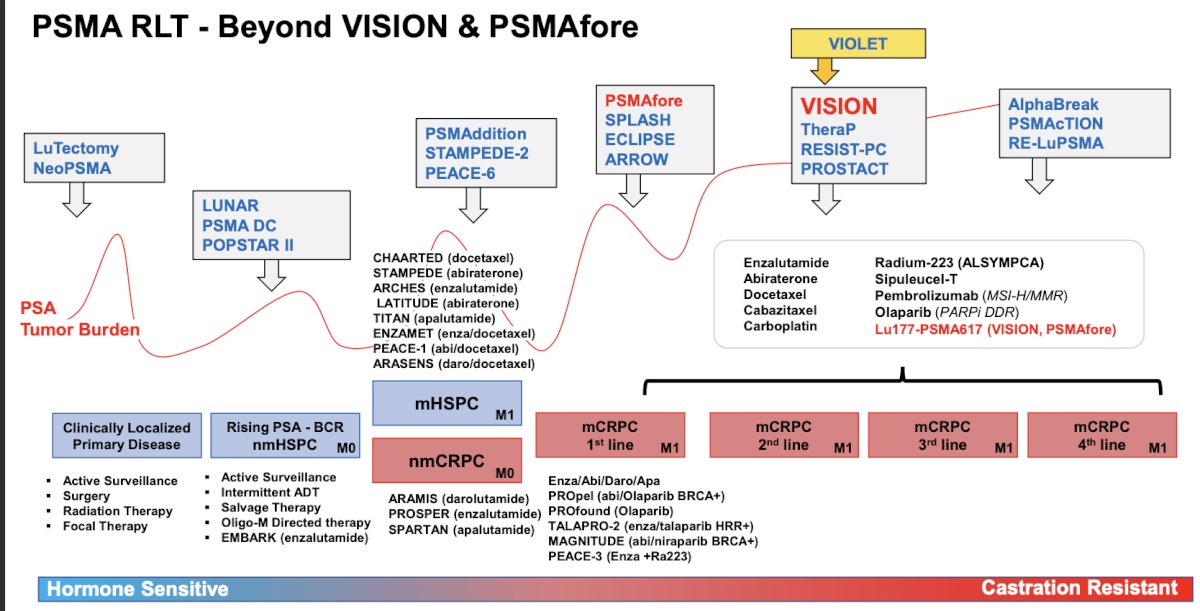
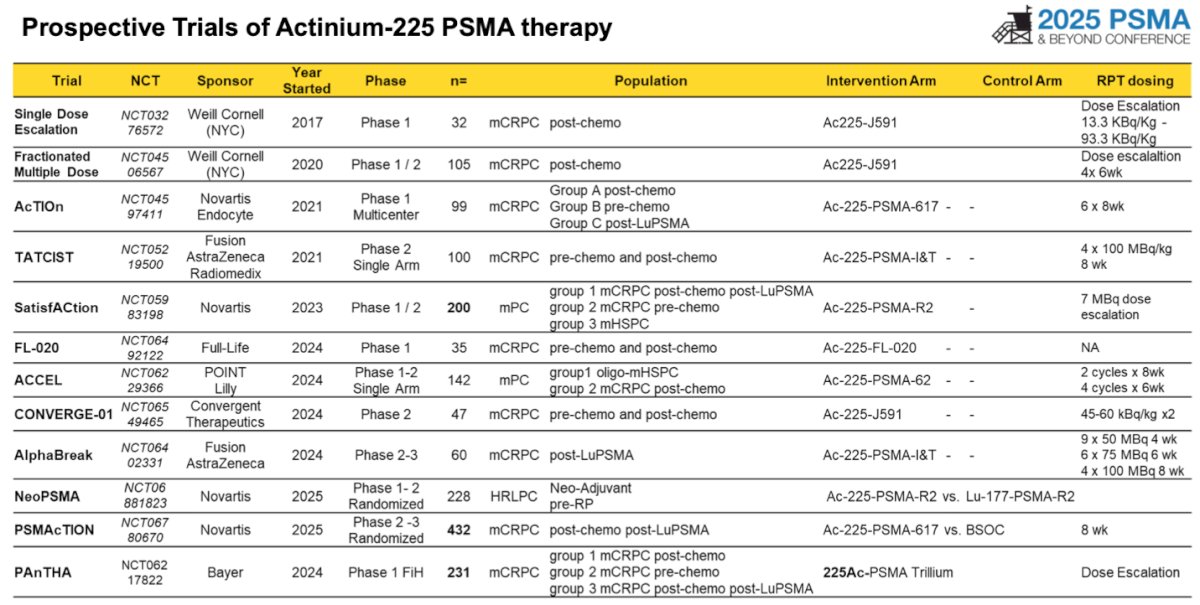
Dr. Calais noted that PSMA-targeted radioligand therapy (RLT) has rapidly expanded over the past decade and is now being evaluated across the full spectrum of prostate cancer. While trials like VISION and PSMAfore have been pivotal, he emphasized that the field extends far beyond these landmark studies. The figure presented illustrates the broad clinical landscape of PSMA RLT, highlighting ongoing and completed trials in various disease settings from early biochemical recurrence to advanced metastatic castration-resistant prostate cancer, underscoring the growing interest in leveraging PSMA RLT across multiple therapeutic windows.
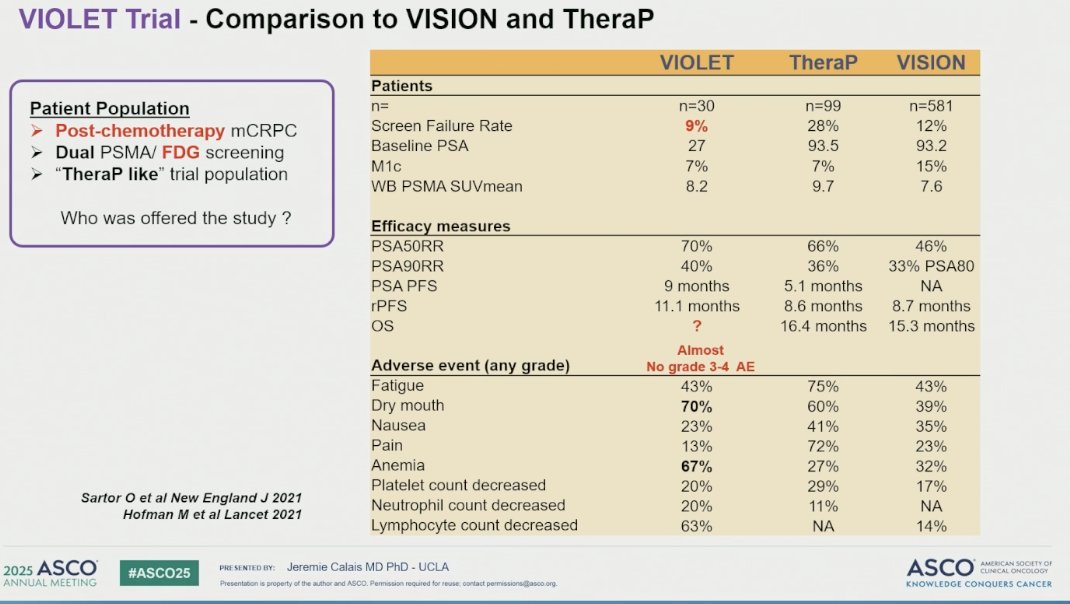
Dr. Calais spotlighted the VIOLET trial as a meaningful addition to the evolving field of PSMA radioligand therapy (RLT) in prostate cancer. The VIOLET trial is a single-center, open-label, phase I/II study evaluating the safety, tolerability, and preliminary efficacy of 161Tb-PSMA-I&T in patients with mCRPC. Terbium-161 (161Tb) is a novel radionuclide that emits both beta particles and high-linear energy transfer, Auger, and conversion electrons, offering the potential to more effectively target micrometastatic disease compared to the more commonly used lutetium-177 (177Lu).
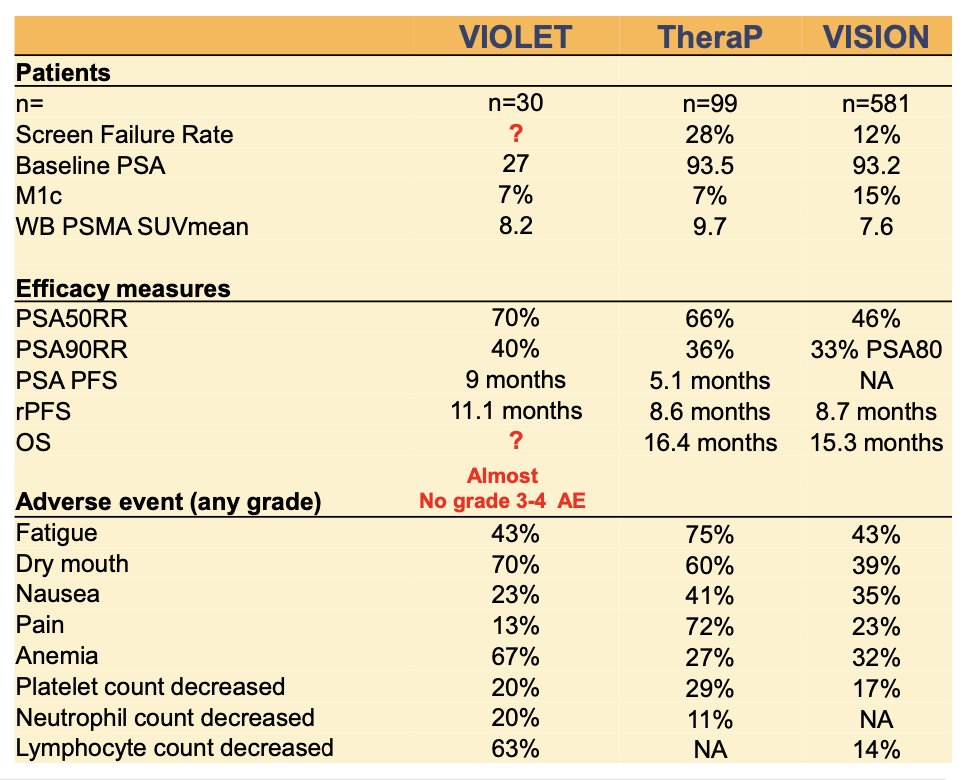
Unlike the larger VISION and TheraP trials, VIOLET enrolled a smaller, more selective cohort of 30 post-chemotherapy mCRPC patients. The trial employed dual-tracer imaging with PSMA PET and FDG PET—similar to the TheraP trial—to enrich for PSMA-avid and metabolically active disease. VIOLET reported a median radiographic progression-free survival (rPFS) that was approximately three months longer compared to results from other trials. However, overall survival data were not reported due to the study’s early phase and limited sample size. Importantly, the safety profile was favorable, with almost no grade 3–4 adverse events observed.3
Actinium-225 (225Ac) is an alpha-emitting radionuclide with potent cytotoxic potential and is under investigation across multiple stages of prostate cancer, including metastatic hormone-sensitive prostate cancer (mHSPC), pre-AR pathway inhibitor (pre-ARDT), and pre-chemotherapy mCRPC, as well as in heavily pretreated mCRPC with diffuse disease. One notable limitation of 225Ac-PSMA radioligand therapy is its strong uptake in salivary glands, often resulting in xerostomia.
A large retrospective study of 488 men with mCRPC treated with 225Ac-PSMA RLT reported a median of 2 cycles (IQR 2–4). The median overall survival (OS) was 15.5 months, and median progression-free survival (PFS) was 7.9 months. However, xerostomia was observed in 236 of 347 evaluable patients (68%), highlighting a significant and common adverse effect associated with salivary gland toxicity.4
Despite encouraging results with 225Ac-PSMA radioligand therapy, several key questions remain unanswered. Long-term toxicity—particularly to the salivary glands, kidneys, and bone marrow—continues to be a major concern, with xerostomia being the most commonly reported adverse event. Additionally, the optimal sequencing of 225Ac-PSMA relative to 177Lu-PSMA is unclear: should it be used before, after, or even in combination with LuPSMA as a “cocktail” strategy?
Patient selection is another critical area of investigation. It remains to be seen whether 225Ac-PSMA is better suited for high- vs. low-volume disease, heterogeneous PSMA expression, or specific imaging patterns such as infiltrative vs. spotty lesions. Numerous ongoing clinical trials are now underway aiming to address these questions and better define the role of 225Ac-PSMA therapy in prostate cancer management.
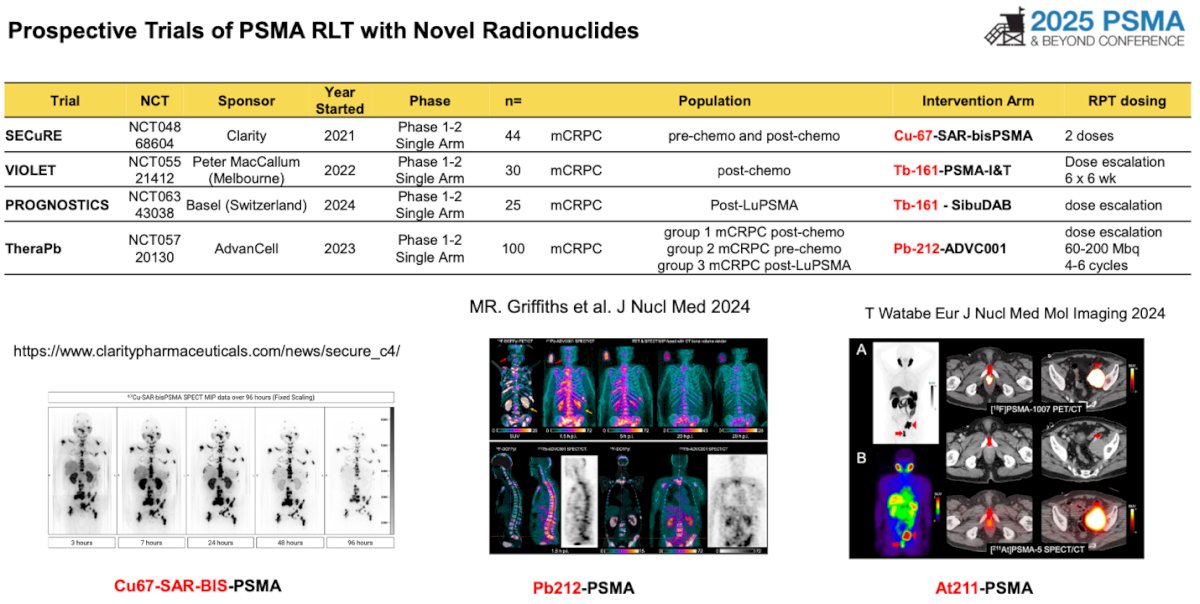
Furthermore, several prospective trials are underway exploring PSMA RLT with novel radionuclides beyond the commonly used 177Lu and 225Ac. These include agents such as 67Cu-SAR-bisPSMA, 161Tb-PSMA-I&T, 161Tb-SibuDAB, and 212Pb-ADVC001. Each of these radionuclides offers unique physical and radiobiological properties that may improve targeting, enhance tumor cell kill, or reduce toxicity. As shown below, these trials represent the next wave of innovation in PSMA RLT, aiming to optimize efficacy across a broader range of prostate cancer phenotypes.
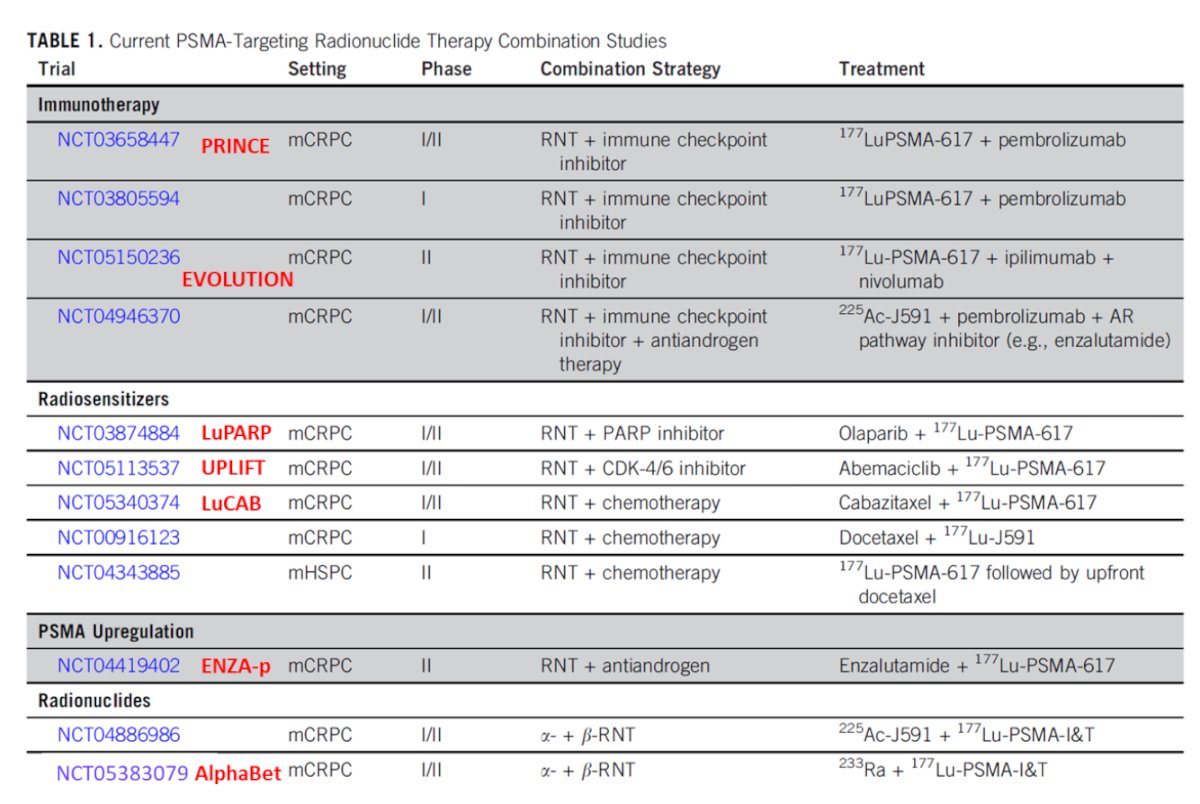
The mechanistic rationale for combining different therapies with PSMA RLT lies in exploiting synergistic pathways that enhance tumor cell kill and overcome resistance mechanisms. As illustrated, PSMA RLT induces DNA double-strand breaks in prostate cancer cells, providing a foundation for synergy with radiosensitizers such as chemotherapy, PARP inhibitors, and CDK4/6 inhibitors. Chemotherapy and taxanes enhance RLT efficacy by disrupting the cell cycle and increasing DNA damage. PARP inhibitors further impair DNA repair mechanisms, amplifying the cytotoxic effect of radioligand-induced DNA damage. Moreover, androgen receptor (AR) blockade with agents like enzalutamide or abiraterone can upregulate PSMA expression on tumor cells, improving the targeting and uptake of RLT

Multiple clinical trials are currently underway exploring a broad range of RLT combination strategies across the prostate cancer treatment spectrum. These include combinations with immune checkpoint inhibitors to enhance anti-tumor immune responses, androgen receptor pathway inhibitors (ARPIs) like enzalutamide or abiraterone to upregulate PSMA expression, and PARP inhibitors to exploit DNA repair deficiencies.
Dr. Calais described the ENZA-p trial, a randomized phase 2 study evaluating the addition of 177Lu-PSMA-617 to enzalutamide in men with mCRPC Eligible patients had rising PSA levels >5 ng/mL, were chemotherapy-naïve for mCRPC, had a positive 68Ga-PSMA PET/CT, and exhibited at least two risk factors for early enzalutamide failure. The trial demonstrated a significant overall survival benefit with the combination therapy, with a median OS of 34 months in the 177Lu-PSMA-617 plus enzalutamide arm versus 26 months in the enzalutamide monotherapy group.
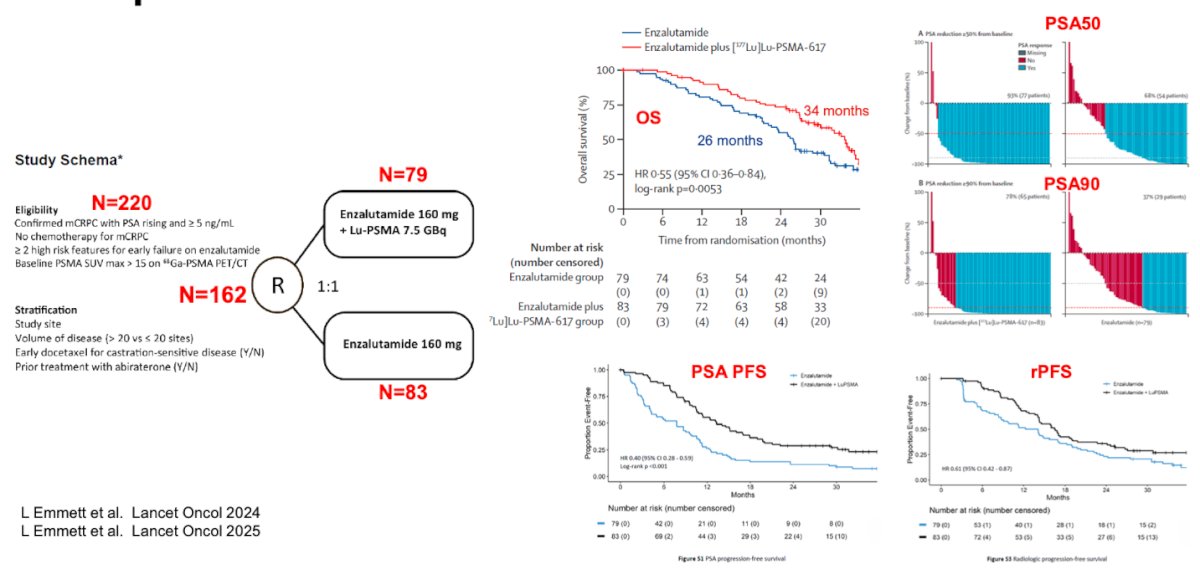
The ENZA-p and PSMAfore trials both explore the use of 177Lu-PSMA-617 in earlier-stage mCRPC, but differ in design and applicability. ENZA-p enrolled a more selective high-risk population, chemotherapy-naïve men with rising PSA >5 ng/mL, PSMA PET SUVmax >15 at one site and >10 at all lesions ≥1 cm, and ≥2 risk factors for early enzalutamide failure. Lastly, administering 4 cycles of 177Lu-PSMA-617 plus enzalutamide. In contrast, PSMAfore included a broader mCRPC population, allowed prior ARPI use in the hormone-sensitive setting, required only PSMA PET positivity without strict SUV thresholds, and randomized patients to 177Lu-PSMA-617 (up to 6 cycles) Notably, all the efficacy measure outcomes were superior in the ENZA-P study as shown in the table below.

The question of whether the combination of enzalutamide and 177Lu-PSMA-617 provides an additive or synergistic effect remains under investigation. An international multicenter retrospective study evaluated 56 mCRPC patients who initiated a new ARPI and underwent PSMA PET imaging within 30 days of starting therapy. Findings revealed that 75% of patients showed no significant whole-body PSMA upregulation, while 25% exhibited an increase in whole-body PSMA tumor volume by ≥30%. These results suggest that while ARPI therapy may upregulate PSMA expression in some patients, this effect is not uniform and raises uncertainty as to whether the combination with LuPSMA yields true synergy or simply additive benefit in selected cases.
PSMA PET BiomarkerPSMA PET imaging is emerging as a valuable biomarker in PSMA-targeted radioligand therapy (RLT), offering insights beyond diagnosis. It can be used to estimate the biodistribution of PSMA-targeted agents for each individual patient, guiding personalized treatment planning. By quantifying whole-body PSMA tumor burden, PSMA PET allows for the identification of likely non-responders, supports prediction of toxicity based on uptake in organs such as salivary glands and kidneys, and provides a surrogate for estimating the radiation dose delivered to tumor sites.
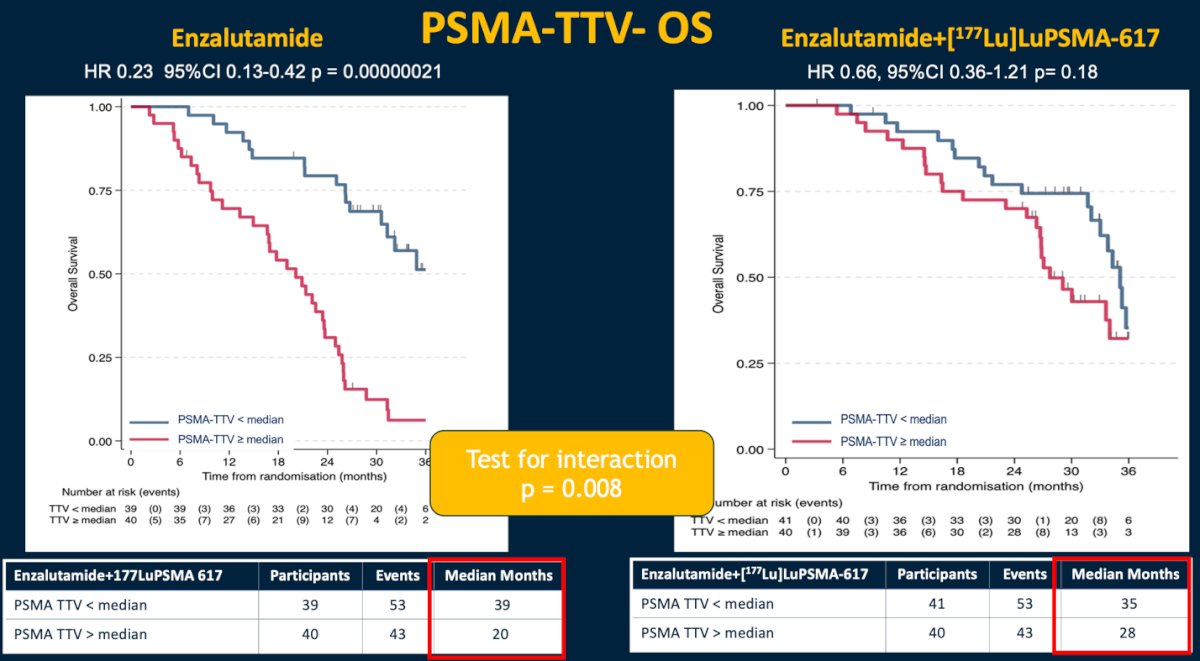
As previously presented by Dr. Emmett, the ENZA-P study was the first to demonstrate the prognostic value of PSMA total tumor volume (PSMA-TTV) for overall survival in patients receiving enzalutamide monotherapy. Beyond its prognostic significance, PSMA-TTV also emerged as a predictive biomarker, identifying patients more likely to benefit from the addition of ¹⁷⁷Lu-PSMA-617 to enzalutamide in this high-risk population. Notably, PSMA SUVmean was neither prognostic nor predictive for progression-free or overall survival in patients treated with the combination of ¹⁷⁷Lu-PSMA-617 and enzalutamide.
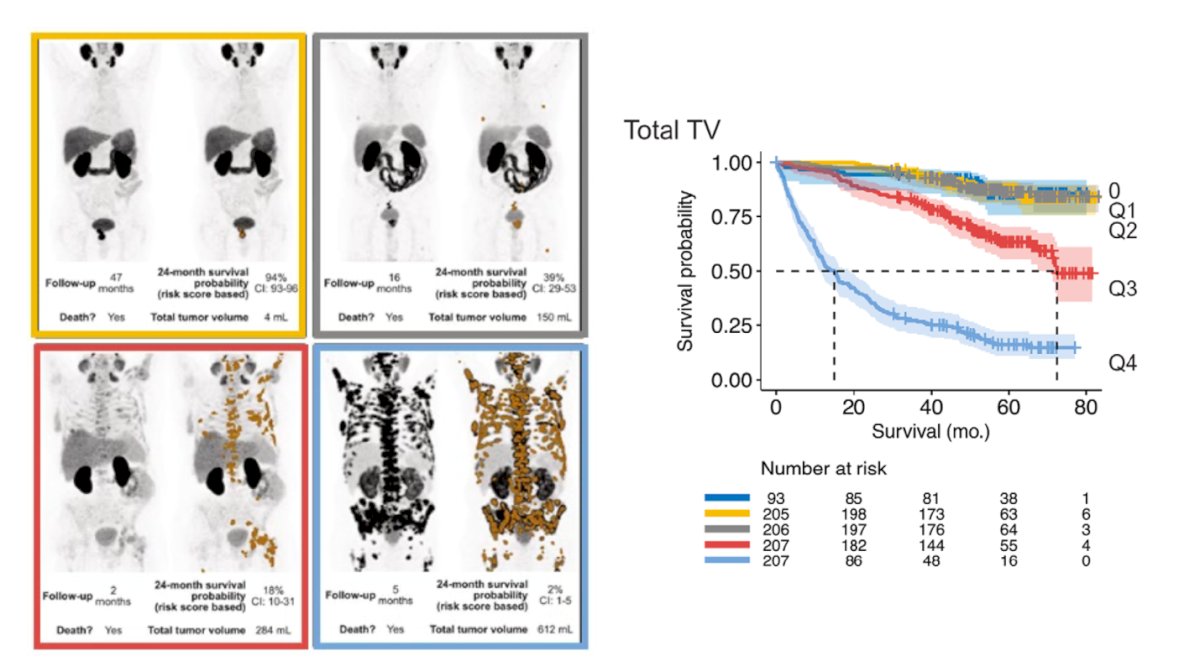
PSMA whole-body tumor volume, expressed in milliliters, is a quantitative imaging metric that reflects the total burden of PSMA-avid disease and closely correlates with the total number of metastatic lesions. This parameter has consistently demonstrated prognostic value for overall survival (OS) across various disease stages and treatment modalities in prostate cancer. Regardless of whether patients are receiving AR-targeted therapy, chemotherapy, or PSMA radioligand therapy, higher PSMA total tumor volume is associated with poorer outcomes, reinforcing its utility as a robust and clinically meaningful imaging biomarker.5
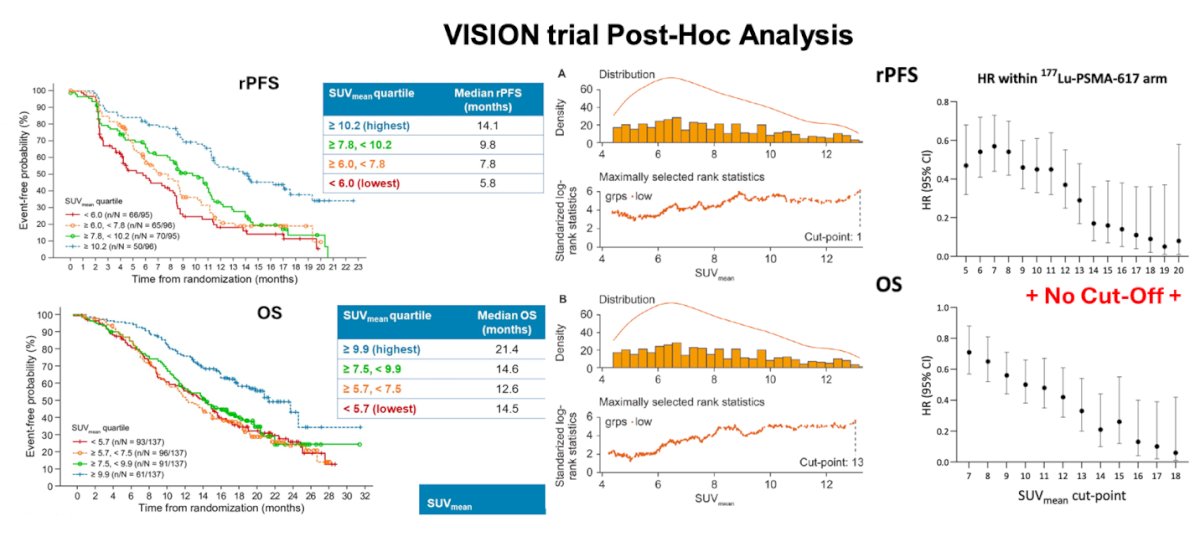
Moreover, PSMA whole-body tumor SUVmean reflects the overall degree and homogeneity of PSMA expression across all disease sites. A higher SUVmean generally indicates more uniform and intense PSMA expression, which facilitates effective targeting with PSMA RLT. Robust evidence has shown that lower SUVmean values are associated with poorer response to PSMA RLT (OS and rPFS), highlighting its role as a predictive biomarker. This underscores the importance of SUVmean in treatment planning, as it may help identify patients less likely to benefit from PSMA-targeted therapies.
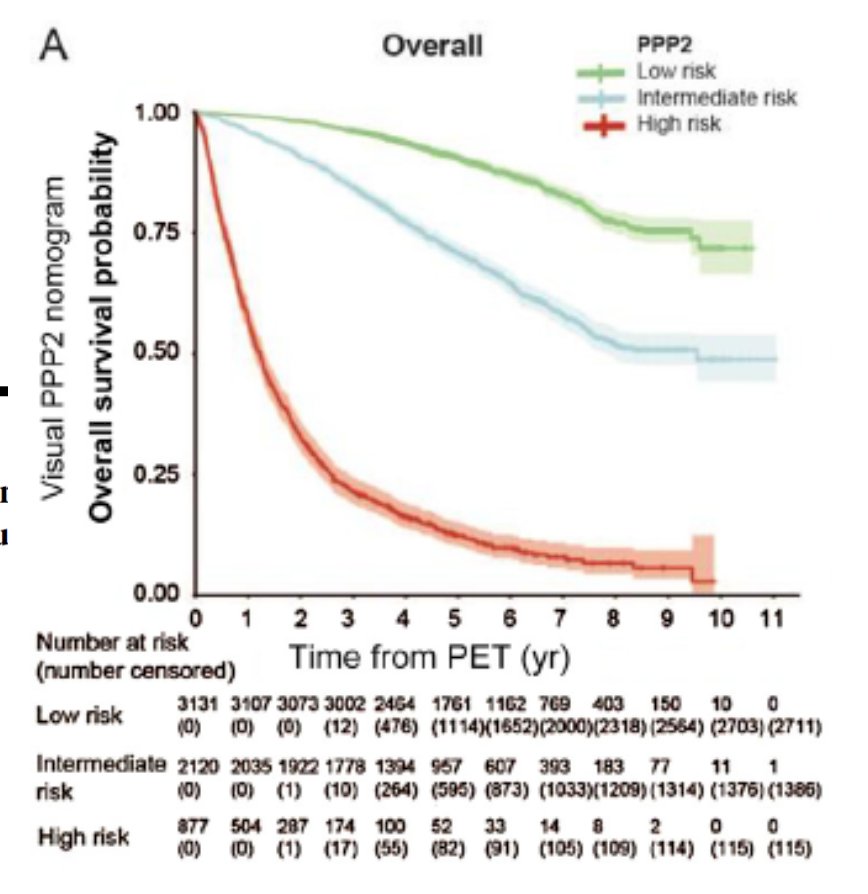
PSMA PET has been increasingly integrated into clinical nomograms across all stages of prostate cancer, including in the mCRPC prior to LuPSMA therapy. These imaging-based tools enhance prognostication by incorporating quantitative PSMA PET metrics such as SUVmean and whole-body tumor volume to better predict treatment response and survival outcomes. One such example is the Prostate-specific Membrane Antigen Positron Emission Tomography Prostate Cancer Molecular Imaging Standardized Evaluation (PPP2) nomogram, which leverages PSMA PET data to refine risk stratification and guide therapeutic decision-making across various treatment modalities.6
Dr. Calais discussed findings from a study presented by Dr. Emmett at ASCO 2025, which showed that low PSMA SUVmean was paradoxically associated with higher PSA90 response rates in patients receiving enzalutamide monotherapy for mCRPC. However, SUVmean did not demonstrate predictive or prognostic value for PFS or OS in patients treated with the combination of LuPSMA and enzalutamide. In contrast, PSMA total tumor volume (TTV) emerged as a strong prognostic marker for OS with enzalutamide alone and was also predictive of improved survival when 177Lu-PSMA-617 was added. These findings support the potential utility of PSMA TTV for patient selection and treatment monitoring.
Dr Calais discussed the critical role of micro-biodistribution and micro-dosimetry in optimizing radionuclide therapy. DNA damage (single- and double-strand breaks) is proportional to absorbed radiation dose, which is influenced by both the type of radionuclide and its spatial distribution within tumors. The Radiation modality matters:
- Beta emitters (low LET, up to a few mm range) deliver a uniform radiation dose but are less effective at targeting microscopic disease.
- Alpha particles (high LET, ~40–100 µm range) induce significantly greater DNA damage—approximately 100× more than beta emitters—making them highly effective in micrometastatic settings.
- Auger electrons (very high LET, <500 nm range) are most effective when localized within or adjacent to DNA, given their ultra-short path length.

There have been few reports to date on the clinical application of Terbium-161 (TB161) PSMA-targeted therapy in prostate cancer. Dr. Calais emphasized the significance of the VIOLET trial presented by Dr. Hofman, noting it represents a major step forward in evaluating this novel radiopharmaceutical.
The VIOLET trial marks the first-in-human use of Terbium-161. In patients with progressive mCRPC, TB161-PSMA-I&T demonstrated a favorable safety profile, and PSA declines ≥90% were observed in 40% of patients.
When comparing the VIOLET trial with prior pivotal studies such as TheraP and VISION, the efficacy outcomes observed with Terbium-161 PSMA-I&T appeared favorable. Notably, PSA response rates and radiographic progression-free survival in VIOLET exceeded those reported in either TheraP or VISION, suggesting a potentially enhanced therapeutic effect with this novel radionuclide as shown below.
However, it’s important to recognize that certain treatment-related adverse events were more frequent in VIOLET. Dry mouth occurred in 70% of patients, and anemia in 67%, both higher than the corresponding rates reported in TheraP and VISION. These findings highlight the need for further comparative studies to validate the clinical advantages and better characterize the safety profile of Terbium-161–based therapies.
While the prognostic and predictive value of both PSMA SUVmean and TTV has been demonstrated in the context of LuPSMA monotherapy in advanced mCRPC, further validation is needed in earlier disease settings, including second-line ARPI use and metastatic hormone-sensitive prostate cancer (mHSPC) as explored in trials like PSMAfore and PSMAddition. Importantly, these imaging biomarkers may also require re-evaluation in the context of emerging radiotherapies using alpha or Auger emitters. There are multiple ongoing prospective trials of combination PSMA RLT and ARPI.
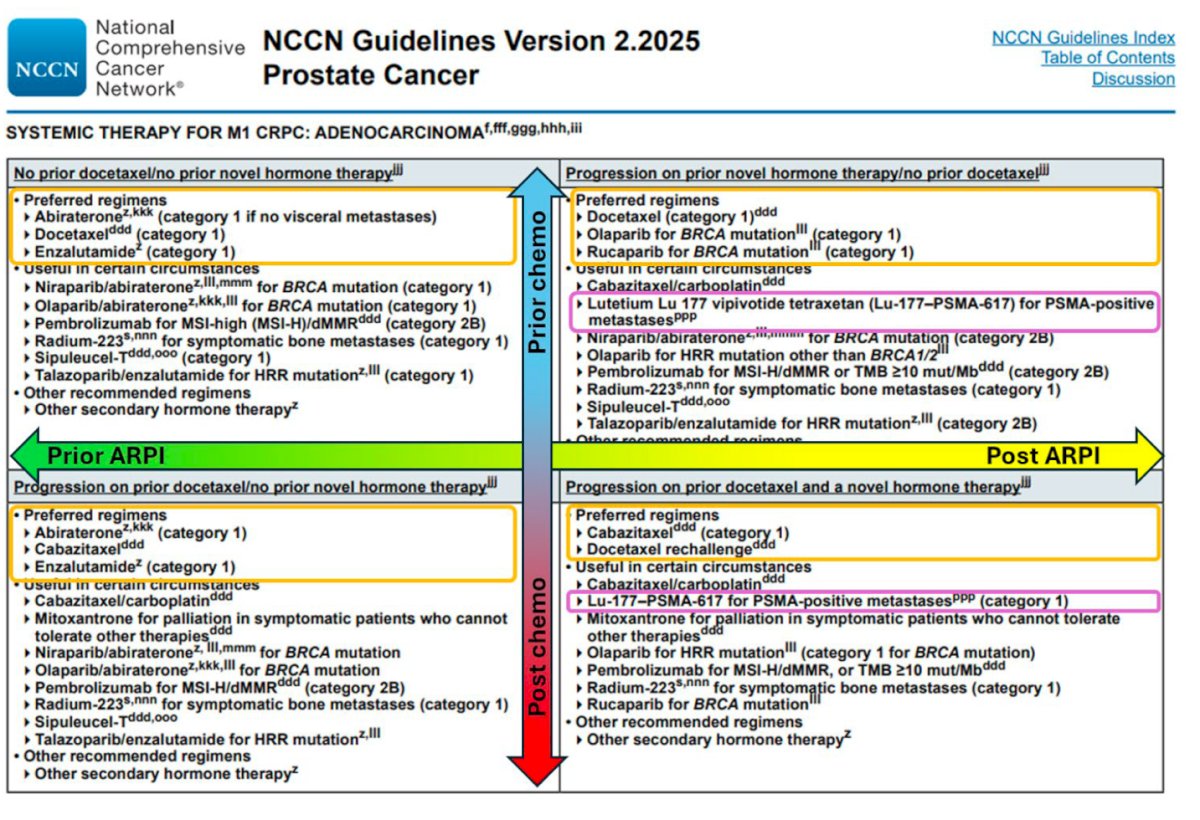
Dr. Calais discussed the evolving challenge of identifying the right patient for the optimal sequence of radioligand therapy (“the perfect track”) in what he called the Radioligand Therapy Remix. While current NCCN guidelines recommend 177Lu-PSMA-617 after ARPI and docetaxel, but before cabazitaxel, future decision-making will become increasingly complex. Key questions include whether LuPSMA should be given before or after ARPIs, chemotherapy, or alpha/Auger-based PSMA therapies, and whether combination approaches (e.g., LuPSMA + ARPI or LuPSMA + alpha/Auger therapy) may offer added benefit. The best treatment sequencing could be very different for each patient, relying on these multiple factors, noted Dr Calais.
Dr. Calais concluded the presentation with the following key messages:
- Auger and alpha emitters deliver significantly higher radiation doses than the beta emitter 177Lu, potentially offering improved efficacy in treating microscopic disease.
- The prognostic value of whole-body quantitative PSMA PET parameters such as total tumor volume and SUVmean varies depending on disease stage and treatment mechanism.
- Optimal sequencing of RLT in metastatic prostate cancer is patient-dependent and remains to be determined through further research.
Presented by: Jeremie Calais, MD, PhD, Ahmanson Translational Theranostics Division, University of California, Los Angeles, CA.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Reference:
- Kostos L, Buteau JP, Hofman MS, Azad AA. Determinants of outcome following PSMA-based radioligand therapy and mechanisms of resistance in patients with metastatic castration-resistant prostate cancer. Ther Adv Med Oncol. 2023 Jun 6;15:17588359231179309. doi: 10.1177/17588359231179309. PMID: 37323184; PMCID: PMC10262652.
- Bakht MK, Beltran H. Biological determinants of PSMA expression, regulation and heterogeneity in prostate cancer. Nat Rev Urol. 2025 Jan;22(1):26-45. doi: 10.1038/s41585-024-00900-z. Epub 2024 Jul 8. PMID: 38977769; PMCID: PMC11841200.
- Buteau JP, Kostos L, Alipour R, Jackson P, McInstosh L, Emmerson B, Haskali MB, Xie J, Medhurst E, Ravi R, Gonzalez BD, Fettke H, Blyth B, Furic L, Owen K, Sandhu S, Murphy DG, Azad AA, Hofman MS. Clinical Trial Protocol for VIOLET: A Single-Center, Phase I/II Trial Evaluation of Radioligand Treatment in Patients with Metastatic Castration-Resistant Prostate Cancer with [161Tb]Tb-PSMA-I&T. J Nucl Med. 2024 Aug 1;65(8):1231-1238. doi: 10.2967/jnumed.124.267650. PMID: 38991752.
- Sathekge MM, Lawal IO, Bal C, Bruchertseifer F, Ballal S, Cardaci G, Davis C, Eiber M, Hekimsoy T, Knoesen O, Kratochwil C, Lenzo NP, Mahapane J, Maserumule LC, Mdlophane AH, Mokoala KMG, Ndlovu H, Pant V, Rathke H, Reed J, Sen IB, Singh A, Sood A, Tauber R, Thakral P, Yadav MP, Morgenstern A. Actinium-225-PSMA radioligand therapy of metastatic castration-resistant prostate cancer (WARMTH Act): a multicentre, retrospective study. Lancet Oncol. 2024 Feb;25(2):175-183. doi: 10.1016/S1470-2045(23)00638-1. Epub 2024 Jan 11. PMID: 38218192.
- Seifert R, Rasul S, Seifert KE, Eveslage M, Rahbar Nikoukar L, Kessel K, Schäfers M, Yu J, Haug AR, Hacker M, Bögemann M, Bodei L, Morris MJ, Hofman MS, Rahbar K. A Prognostic Risk Score for Prostate Cancer Based on PSMA PET-derived Organ-specific Tumor Volumes. Radiology. 2023 May;307(4):e222010. doi: 10.1148/radiol.222010. Epub 2023 Apr 18. PMID: 37070991; PMCID: PMC10838189.
- Karpinski, Madeleine J. et al. Updated Prostate Cancer Risk Groups by Prostate-specific Membrane Antigen Positron Emission Tomography Prostate Cancer Molecular Imaging Standardized Evaluation (PPP2): Results from an International Multicentre Registry Study. European Urology.