(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a prostate, testicular, and penile cancers poster session. Dr. Neal Shore presented the ongoing MEVPRO-2 study, a randomized, phase III trial of mevrometostat in combination with enzalutamide for androgen receptor pathway inhibitor (ARPI)-naïve metastatic castrate-resistant prostate cancer (mCRPC) patients.
Mevrometostat (PF-06821497) is a potent, selective inhibitor of the histone methyltransferase enhancer of zeste homolog 2 (EZH2), which is canonically involved in epigenetic repression of target genes.1 In prostate cancer, EZH2 overexpression is associated with poor prognosis, contributing to disease progression through transcriptional repression of tumor suppressor genes and androgen receptor (AR) co‑activation, co‑regulation of AR‑mediated transcriptional programs, and cell cycle deregulation through methylation of nonhistone targets.2–4
Given the associations between EZH2 and the AR, the addition of an EZH2 inhibitor to an ARPI is hypothesized to extend the duration of clinical response, and delay or prevent antiandrogen resistance compared with an ARPI alone.5
Enzalutamide is an ARPI approved for the treatment of patients with CRPC, metastatic castration-sensitive prostate cancer (CSPC), and nonmetastatic CSPC with biochemical recurrence at high risk for metastasis.6 Mevrometostat plus enzalutamide showed promising activity and a manageable adverse event profile in a phase I/II dose-escalation study (NCT03460977) in patients with CRPC who had received prior treatment with abiraterone or enzalutamide. Diarrhea, dysgeusia, and anemia were the most common adverse events considered to be related to mevrometostat.7 Diarrhea is manageable with supportive care.
Herein, Dr. Shore presented the study design of a phase III trial that explores whether the addition of mevrometostat to enzalutamide can delay or prevent antiandrogen resistance thereby increasing the duration of clinical benefit of enzalutamide in patients with mCRPC who have not previously received an ARPI.
MEVPRO-2 (NCT06629779) is a global, randomized, double-blind, placebo‑controlled phase III trial in ARPI-naïve mCRPC patients. The key inclusion and exclusion criteria are detailed in the table below.

Approximately 900 patients will be randomized 1:1 to receive either:
- Mevrometostat (875 mg twice daily with food) in combination with enzalutamide (160 mg once daily)
- Placebo (twice daily) with enzalutamide (160 mg once daily).
- The sample size estimation is based on the number of events needed to observe protocol-defined statistical differences between the treatment groups.
- Randomization will be stratified by:
- Previous docetaxel use in the metastatic CSPC setting and
- Presence of hepatic metastases.
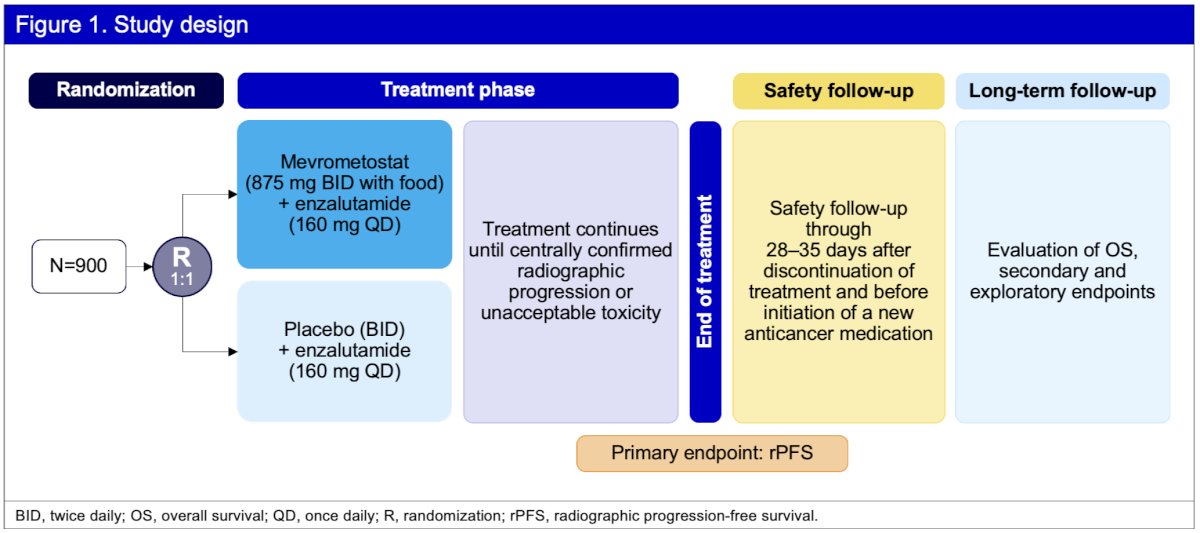
The primary efficacy endpoint is radiographic progression-free survival (rPFS) per RECIST 1.1 (soft tissue) and Prostate Cancer Working Group 3 (PCWG3, bone) assessed by blinded independent central review. The key secondary endpoints are overall survival (OS) and time to pain progression. Other secondary endpoints include measures of antitumor activity by overall response rate and duration of response, patient-reported outcomes, pharmacokinetics, and circulating tumor DNA burden.
The statistical methods are as follows:
- Time-to-event endpoints will be compared between treatment arms using a stratified logrank test.
- Hazard ratios and 95% confidence intervals (CIs) will be estimated using a stratified Cox proportional hazard model.
- Kaplan–Meier analysis will summarize time-to-event endpoints and will include the median and 95% CIs based on the Brookmeyer–Crowley method.
The first patient was enrolled into the study on October 22, 2024. Enrollment in MEVPRO-2 is planned/ongoing in the Asia Pacific, Europe, Latin America, North America, and South Africa. The study is estimated to be completed in November 2028.
Presented by: Neal Shore, MD, FACS, Urologist, Director, CPI, Carolina Urologic Research Center, Atlantic Urology Clinics, Myrtle Beach, SC
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:- Kung PP, Jura N, DiNitto JP, et al. Identification of inhibitors of phosphoinositide 3-kinase alpha using an integrated virtual and biochemical screening strategy. J Med Chem. 2018;61(3):650–665.
- Xu K, Wu ZJ, Groner AC, et al. EZH2 oncogenic activity in castration-resistant prostate cancer cells is Polycomb-independent. Science. 2012;338(6113):1465–1469.
- Varambally S, Dhanasekaran SM, Zhou M, et al. The polycomb group protein EZH2 is involved in progression of prostate cancer. Nature. 2002;419:624–629.
- Park SH, Brandi F, Sommariva M, et al. Selective inhibition of EZH2 by a small molecule inhibitor blocks tumor cell proliferation. Sci Adv. 2021;7(15):eabe2261.
- Ku SY, Rosario S, Wang Y, et al. Rb1 and Trp53 cooperate to suppress prostate cancer lineage plasticity, metastasis, and antiandrogen resistance. Science. 2017;355(6320):78–83.
- Astellas Pharma US Inc. Full prescribing information: XTANDI® (enzalutamide) for oral use. 2023. Available from: https://www.astellas.us/docs/12a005-enz-wpi.pdf. Accessed 2025 Jan 15.
- Schweizer MT, Alumkal JJ, Chi KN, et al. Updated results from a randomized phase III trial of XYZ agent in metastatic castration-resistant prostate cancer. J Clin Oncol. 2024;42(16_suppl):5061.