(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a prostate, testicular, and penile cancers poster session. Dr. Alan Bryce presented the preliminary results from a phase II trial of PT-112 monotherapy in late-line metastatic castration-resistant prostate cancer (mCRPC).
Late-line mCRPC patients have poor survival and quality of life outcomes due to disease heterogeneity and bone/visceral metastases. PT-112 is a novel therapy that inhibits ribosome biogenesis and induces immune activation, resulting in tumor regression and disease control in both soft tissue and bone in heavily pre-treated mCRPC patients.1,2 Its biodistribution produces significant uptake in mineralized bone, enabling a beneficial impact in bone metastatic sites common in mCRPC. Herein, Dr. Bryce reported the results of a phase II study of PT-112 monotherapy in a late-line mCRPC population (NCT02266745).
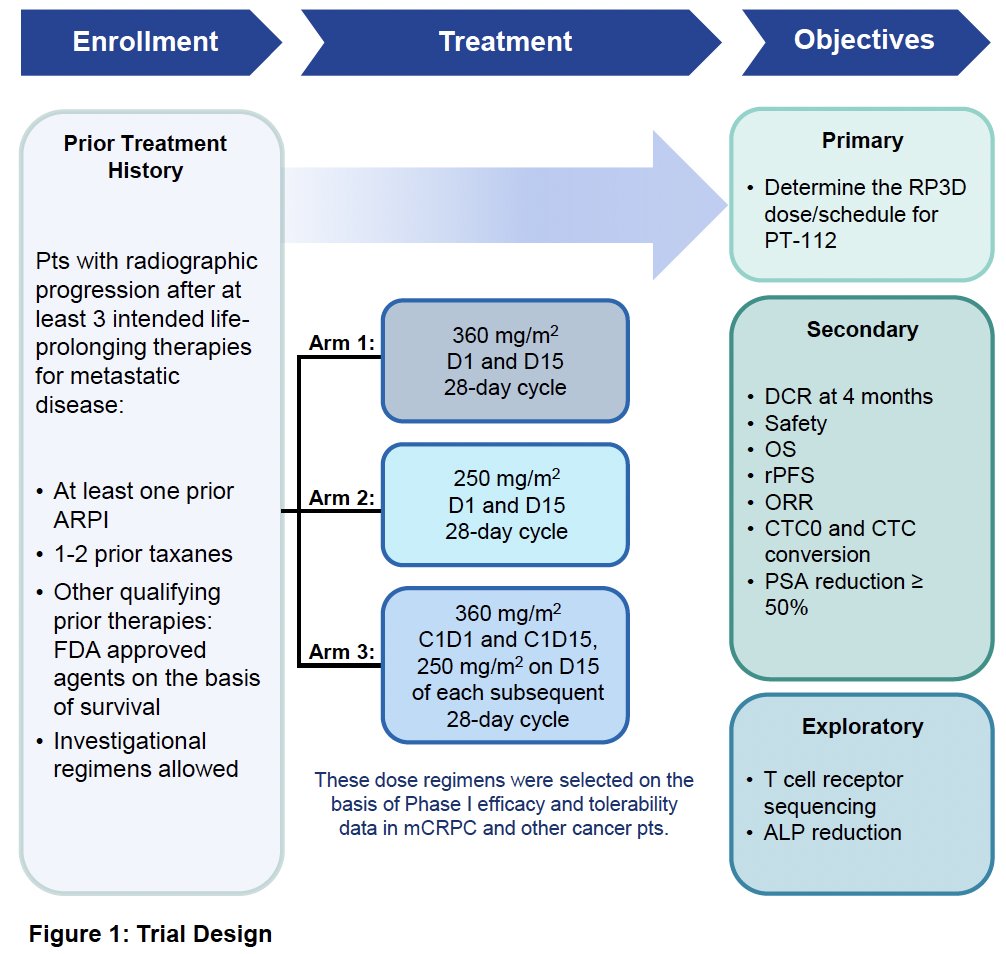
This phase II trial includes patients with radiographic progression after ≥3 ‘life-prolonging’ therapies for metastatic disease, including ≥1 prior ARPI and 1–2 prior taxanes. Patients were randomized to one of three PT-112 arms:
- 360 mg/m2 on Days 1 and 15 of a 28-day cycle
- 250 mg/m2 on Days 1 and 15 of a 28-day cycle
- 360 mg/m2 on Days 1 and 15 of a 28-day cycle, followed by 250 mg/m2 on Day 15 of each subsequent 28-day cycle
The primary study objective was to determine the recommended phase III dose (RP3D) and schedule for PT-112. Secondary endpoints included:
- Disease control rate (DCR) at 4 months
- Safety
- Overall survival
- Radiographic progression-free survival
- Objective response rate
- Circulating tumor cell (CTC) kinetics
- PSA50 reduction
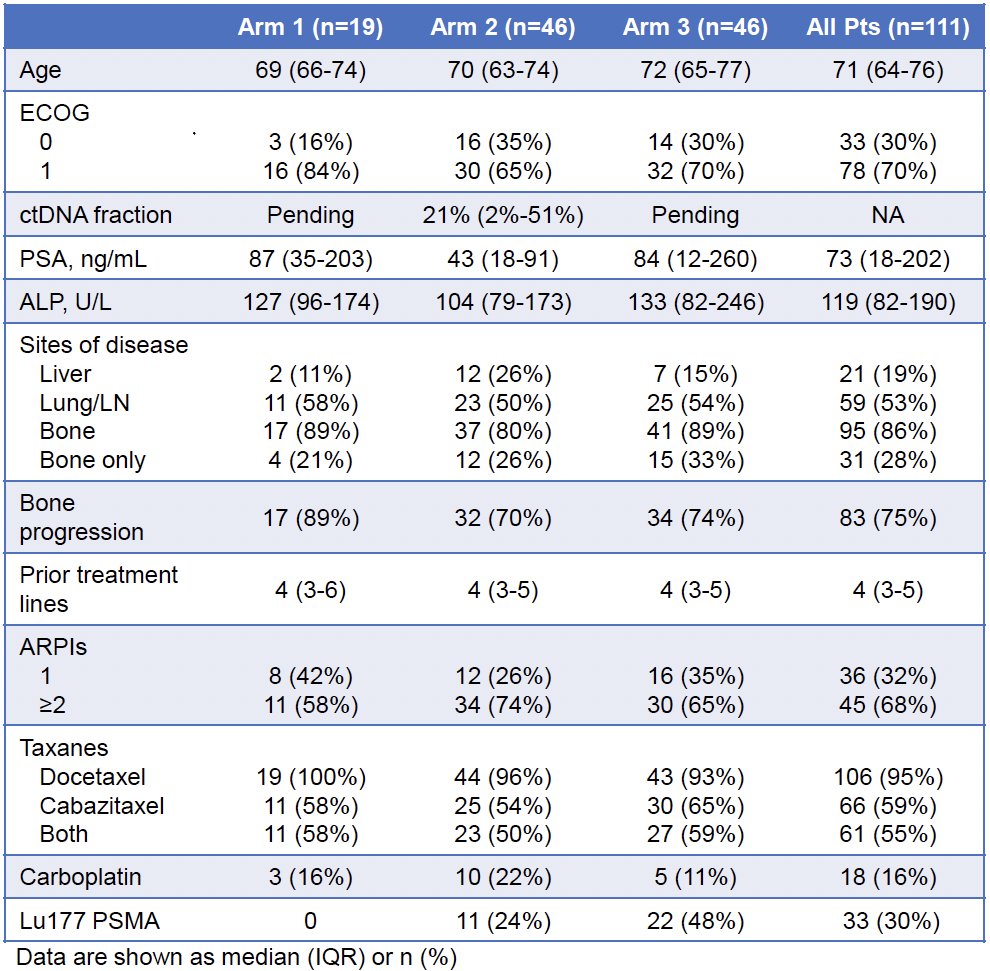
The baseline patient characteristics are summarized below. The median patient age was 71 years. The median PSA was 73 ng/ml. 19% of patients had liver metastases. The median number of prior treatment lines was four. 68% of patients had received ≥2 prior APRIs. 95% of patients had received prior docetaxel, and 55% had received both docetaxel and cabazitaxel. Other common treatments included carboplatin (16%) and 177Lu-PSMA (30%).
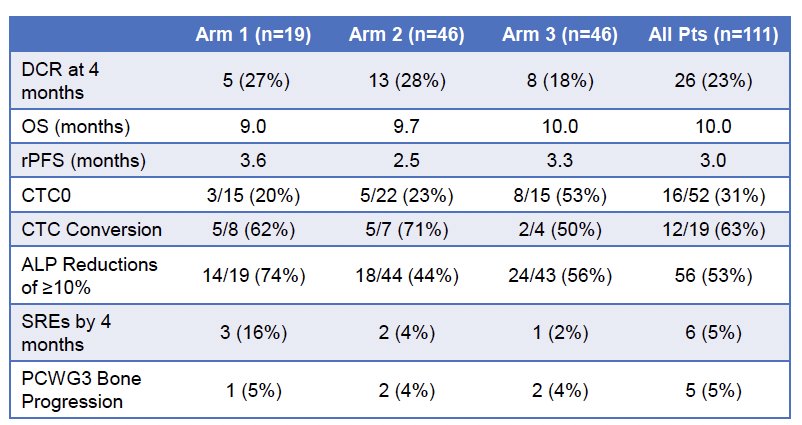
Select efficacy outcomes are summarized in the table below. Due to superior balance of efficacy and tolerance at interim analysis, Arms 2 and 3 proceeded to full enrollment, while Arm 1 was discontinued. The 4-months DCR was 23%. The median overall survival was 10 months. The median rPFS was 3 months. A CTC conversion was observed in 12/19 patients (63%). A ≥10% reduction in ALP levels was observed in 53% of patients. Only 5% of patients experienced skeletal-related events by 4 months or bone progression per the PCWG3 criteria.
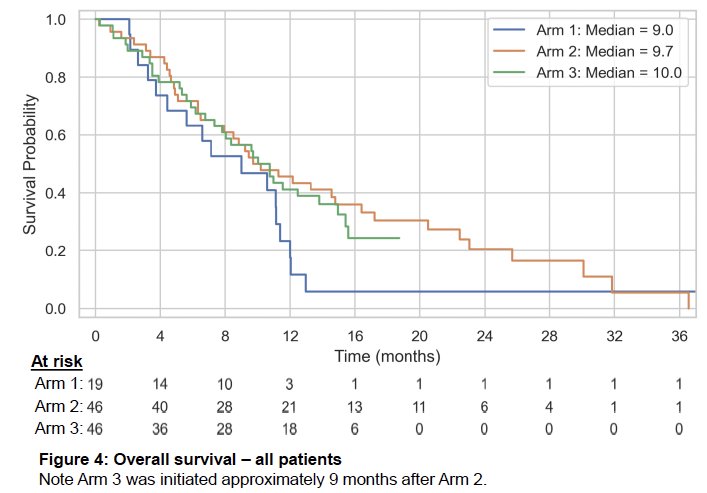
In the more mature Arm 2, the median overall survival in patients without prior cabazitaxel (n=22) was 16.4 months and in those without cabazitaxel or 177Lu-PSMA (n=17) was 20.5 months.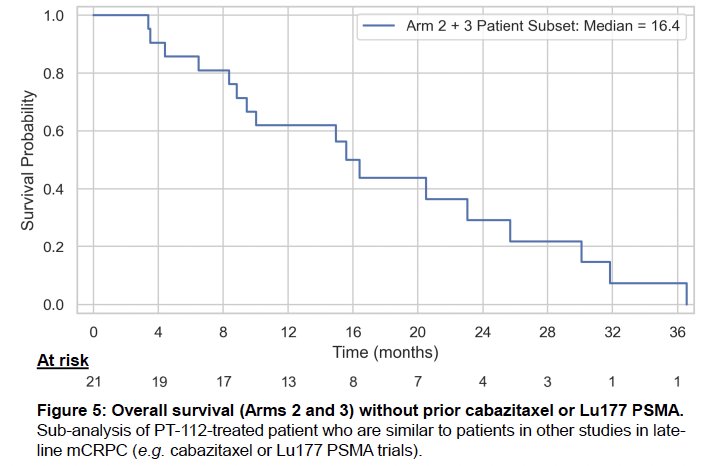
A signal of immune response was observed via T-cell receptor (TCR) sequencing with a statistically significant 20% increase in the percentage of TCR+ blood cells.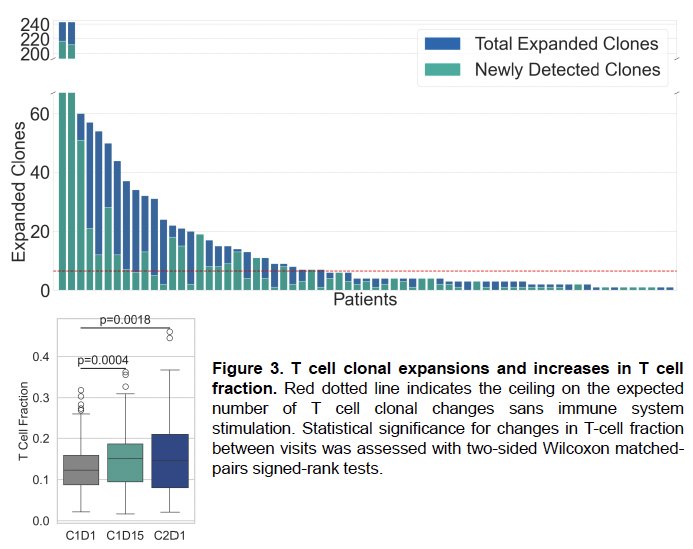
The most common reason for treatment discontinuation was clinical or radiographic progression (61%). Discontinuation due to adverse events was observed in 12% of patients.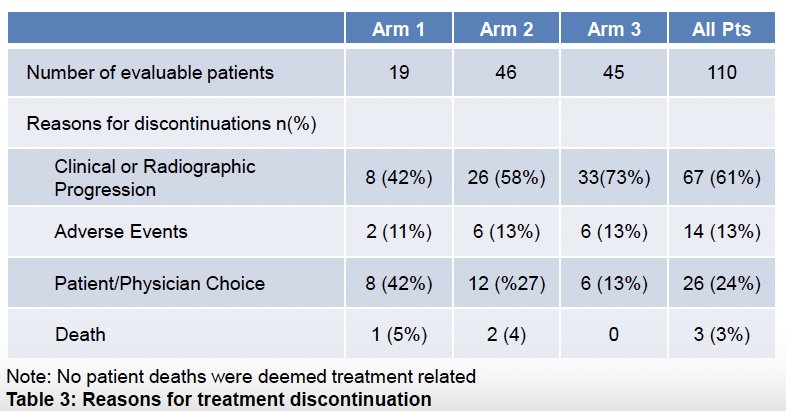
The treatment-related adverse events (TRAEs) are summarized below. Overall, grade 1–2, 3, and 4 TRAEs were observed in 58%, 29%, and 7% of patients, respectively. The most common TRAE was nausea (40%), followed by anemia (32%) and fatigue (25%). The most common grade 3 TRAEs were anemia (8%), fatigue (7%), and thrombocytopenia (5%).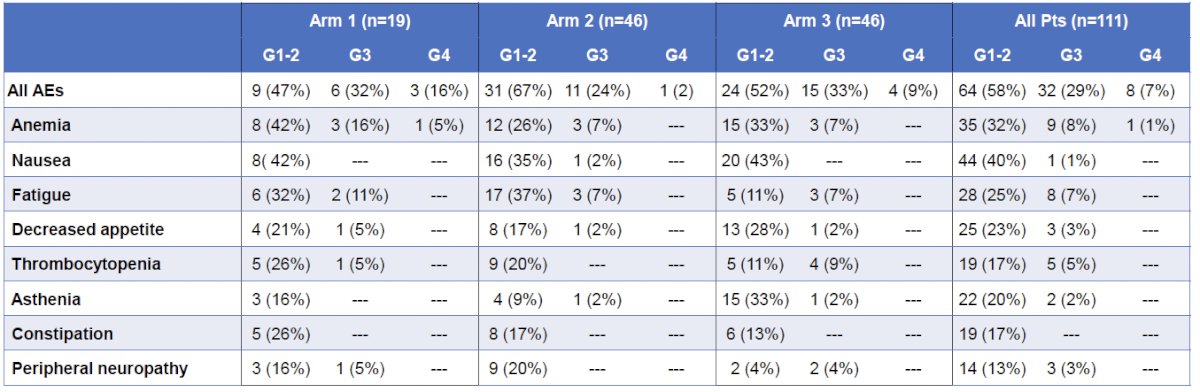
Dr. Bryce concluded his presentation as follows:
- Patients in this trial had very late-line mCRPC (median of 4 prior lines), required radiographic progression at entry, and were heavily disease burdened, as evidenced by multi-site metastases and a high ctDNA fraction.
- PT-112 treatment resulted in a reasonably low rate of grade 3–4 TRAEs. A therapeutic benefit was demonstrated by reductions in ALP levels and CTC counts, with an increase in T cell fraction and clones. Additionally, despite a high rate of progressive bone disease at study entry (75%), low rates of bone progression (5% confirmed by PCWG3) and skeletal-related events (5% at 4 months) on study suggest marked control of metastatic bone disease, consistent with PT-112’s biodistribution.
- The median overall survival duration, ranging from 10 months overall to 16.4 months by sub-analysis of relevant patients not yet exposed to cabazitaxel or 177Lu-PSMA, is encouraging given the late treatment setting and heavy disease burden.
- Arm 3 was selected as the RP3D due to a better balance of efficacy and safety.
- Overall evidence of safety, immune activation, and treatment benefit underscore the novelty of PT-112 and support the initiation of a phase III study versus standard of care.
Presented by: Alan Haruo Bryce, MD, Professor, Department of Medical Oncology & Therapeutics Research, City of Hope, Phoenix, AZ
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:- Yamazaki T, Andre F, Galluzzi L, et al. Defining immunogenic cell death in cancer and its therapeutic potential. Oncoimmunology. 2020;9:1721810.
- Rajan A, Thomas CJ, Gulley JL, et al. Mechanisms of resistance to immunotherapy in lung and other solid tumors. Cancer Res. 2025;85:5819.