(UroToday.com) The 2025 ASCO annual meeting featured a prostate cancer rapid oral abstract session and a presentation by Dr. Andrew Parsonson discussing DB‑1311/BNT324, a novel B7H3 antibody drug conjugate, in patients with heavily pretreated castration resistant prostate cancer (CRPC).
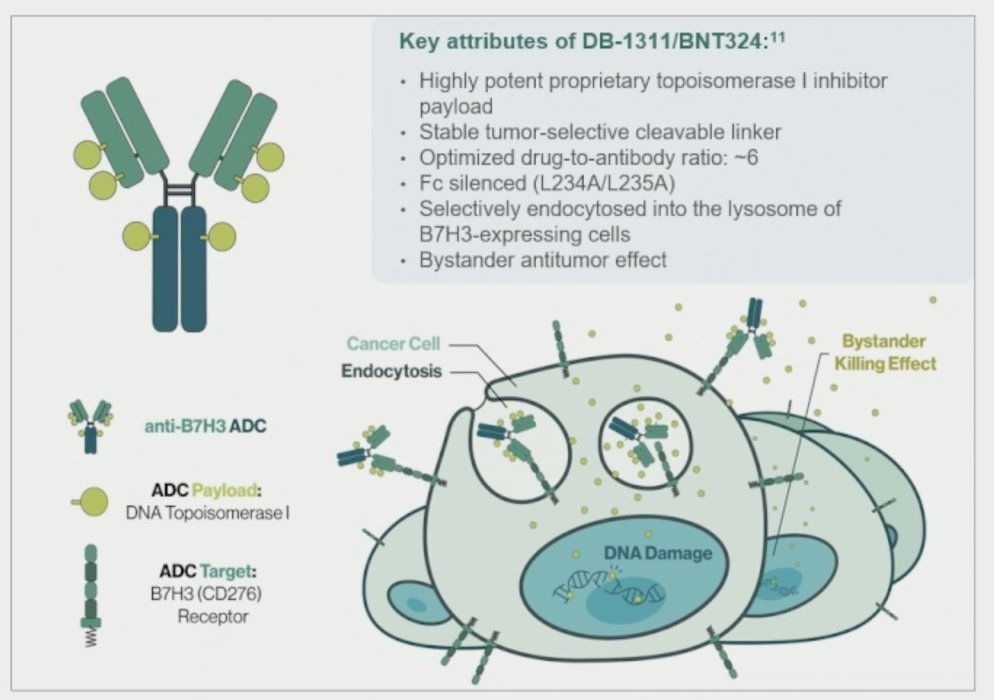
As the incidence rate of prostate cancer is increasing, there is a high unmet need for effective therapy for patients with heavily pretreated CRPC. B7H3 is an immunoregulatory protein that is highly expressed in CRPC and correlates with a poor prognosis. B7H3 antibody drug conjugates have reported early clinical activity in CRPC, including DB-1311/BNT324, an investigational B7H3 antibody drug conjugates that received FDA Fast-Track Designation for previously treated CRPC:
This phase 1/2 study enrolled patients with advanced/metastatic solid tumors, including previously treated CRPC (post docetaxel/hormonal therapy). Dose optimization cohorts randomized patients to receive 6 mg/kg or 9 mg/kg Q3W DB-1311/BNT324 until progression or unacceptable toxicity:
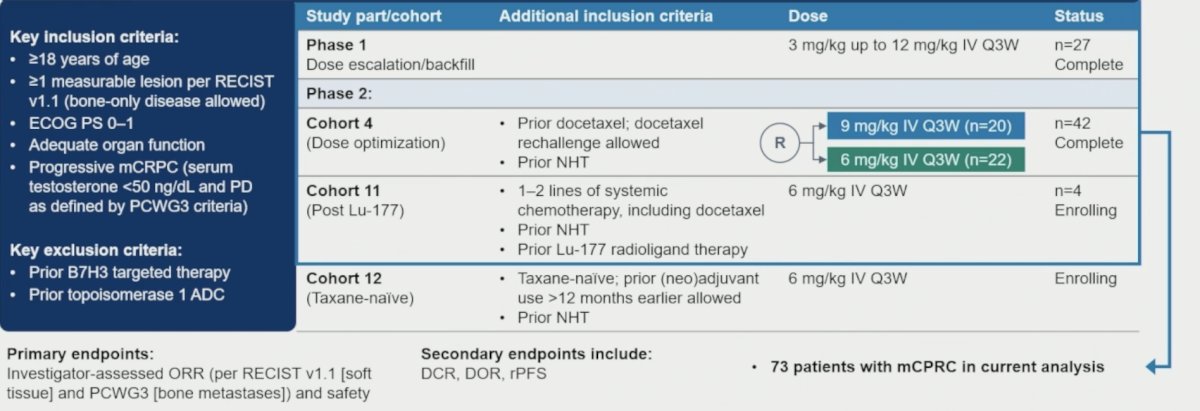
The primary endpoints were objective response rate (based on investigator assessment per RECIST 1.1 and PCWG3 criteria) and safety. Secondary endpoints included disease control rate, duration of response, and radiographic progression-free survival.
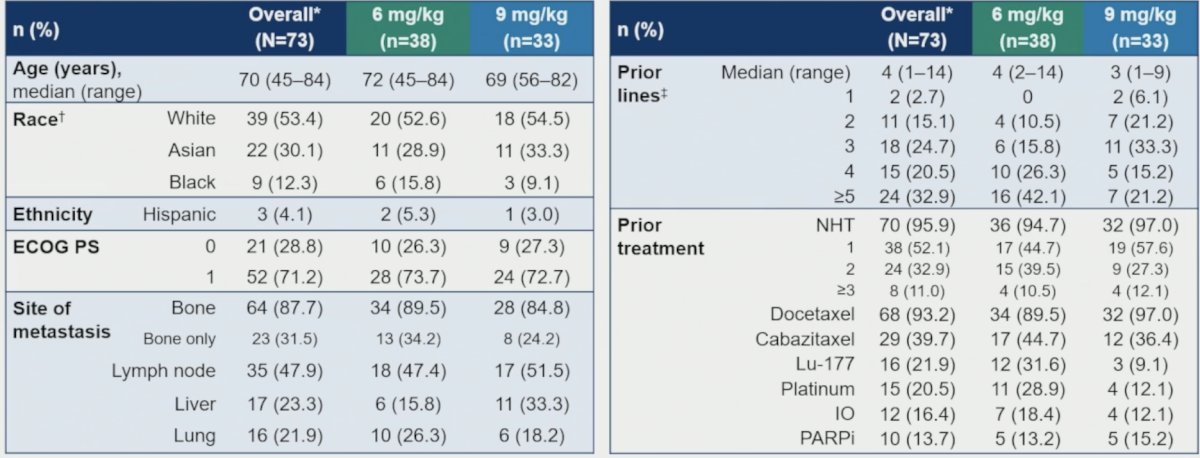
As of March 4, 2025, 465 patients were treated with DB-1311/BNT324, including 73 patients with CRPC (USA 43.8%, Australia 28.8%, and East Asia 27.4%). The median age was 70 years (range 45–84), 53.4%/30.1%/12.3% were White/Asian/Black, 71.2% had ECOG performance status 1, and 31.5% had bone only disease. The median number of prior lines was 4 (range 1–14) and 32.9% had ≥5 prior lines. Most patients received prior docetaxel (93.2%) and hormonal therapy (95.9%), and other therapies included PARP inhibitors (13.7%), Lutetium-177 (21.9%), and immunotherapy (16.4%):
Among 52 response-evaluable patients (measurable disease at baseline per RECIST 1.1), the best overall response was partial response in 22 patients and stable disease in 25 patients for an unconfirmed objective response rate of 42.3% (95% CI 28.7-56.8) and disease control rate of 90.4% (95% CI 79.0, 96.8). The median duration of response was not reached (95% CI 4.0, NE):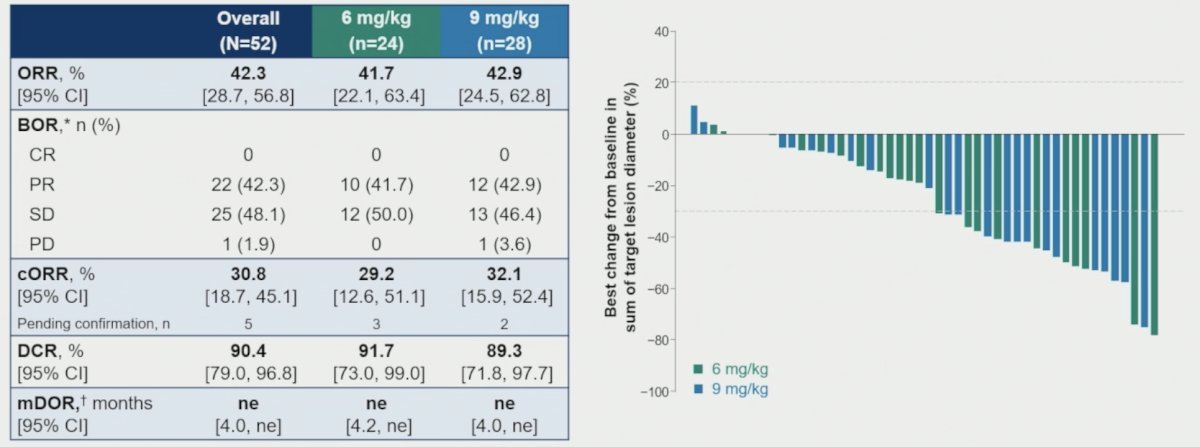
The median radiographic progression-free survival (n = 68) was not reached (95% CI 5.7, not reached) with a 6-month rate of 67.7%: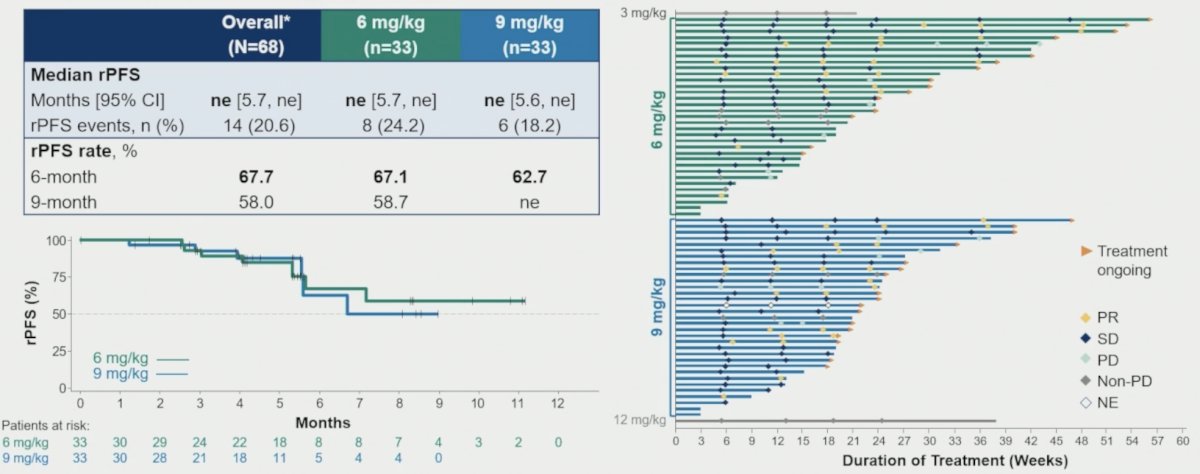
Outcomes appear better in earlier treatment lines, with encouraging activity regardless of line of treatment, type of prior treatment, or metastatic site (but small sample sizes):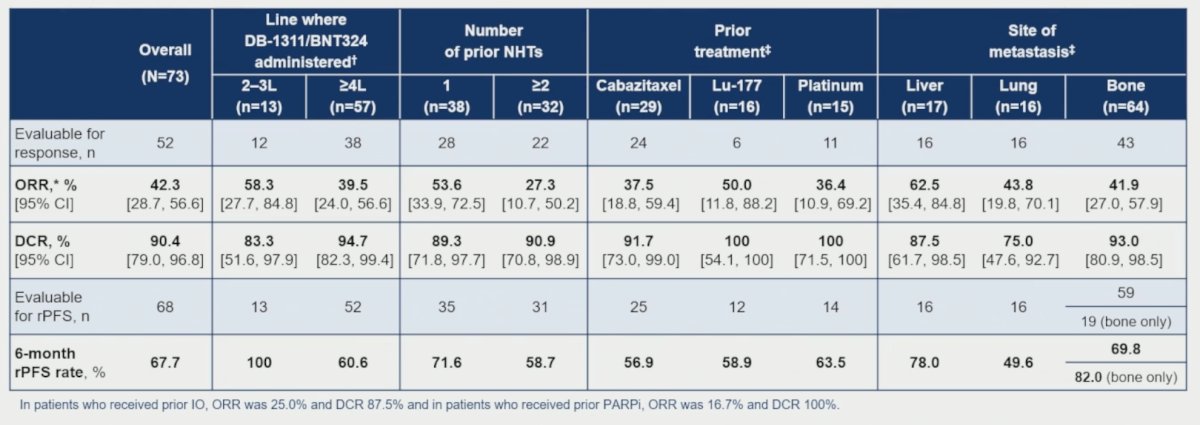
The CRPC safety profile (n = 73) is supported by the safety in the larger overall population (n = 465). Treatment-related adverse events occurred in 66 (90.4%) and 429 (92.3%) patients and were Grade ≥3 in 31 (42.5%) and 220 (47.3%) patients, respectively. Treatment related adverse events led to dose reduction in 12 (16.4%) and 71 (15.3%) patients, to discontinuation in 7 (9.6%) and 30 (6.5%) patients, and to death in 0 and 2 (0.4%) patients, respectively: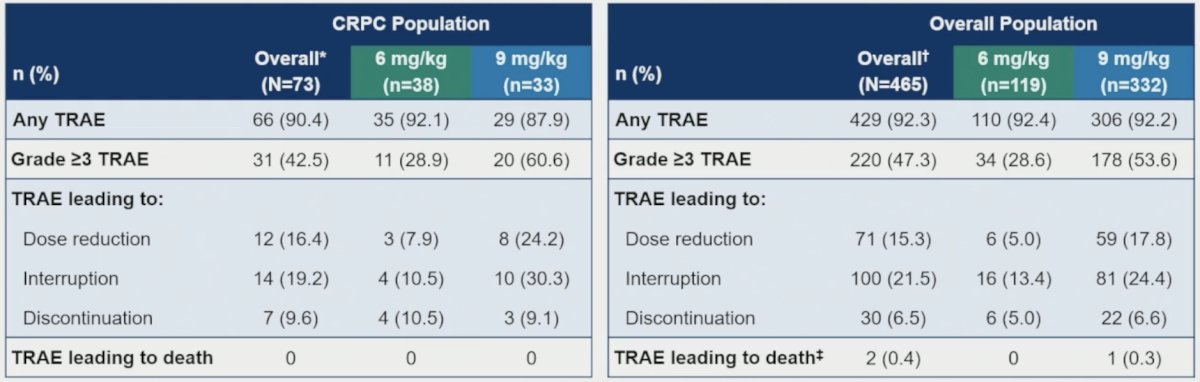
Gastrointestinal and hematological events, primarily grade 1–2, were the most common treatment related adverse events. Hematological treatment related adverse events occurred more frequently with 9 mg/kg versus 6 mg/kg, both in the CRPC and overall populations, but did not lead to treatment discontinuation: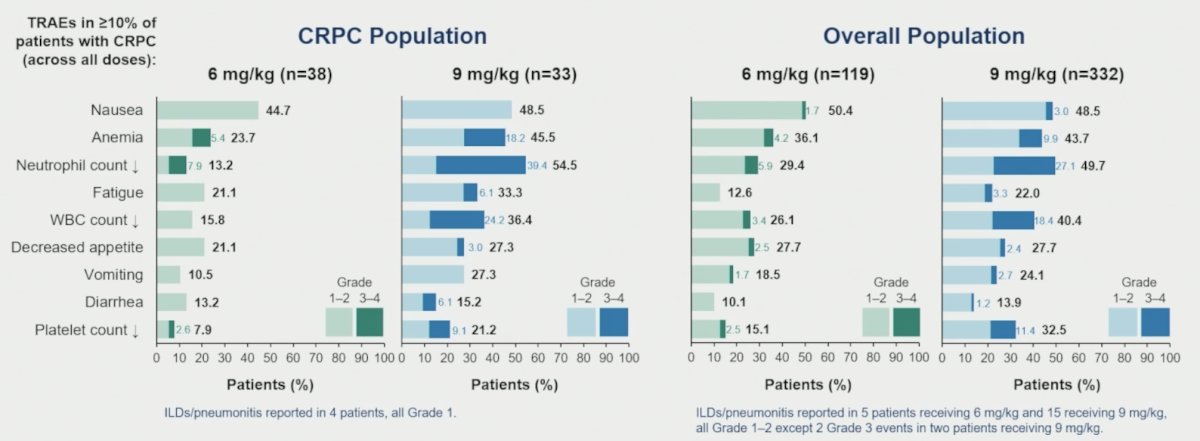
Dr. Parsonson concluded his presentation discussing DB‑1311/BNT324 in patients with heavily pretreated CRPC with the following take-home points:
- DB-1311/BNT324 showed encouraging efficacy and a manageable safety profile in heavily pretreated CRPC patients
- The objective response rate was 42.3%, disease control rate was 90.4%, and 6 month radiographic progression free survival rate was 67.7%, with similar outcomes in the 6 mg/kg and 9 mg/kg cohorts
- The outcomes appeared better in earlier lines of treatment
- There were low discontinuation rates for both the 6 mg/kg and 9 mg/kg despite higher Grade 3+ treatment related adverse events with 9 kg/mg
- Gastrointestinal and hematologic toxicities were the most common treatment related adverse events
- Cohort 11 (CRPC after Lutetium-177) and cohort 12 (taxane-naïve CRPC) are currently enrolling patients
- Further development of DB-1311/BNT324 in prostate cancer is warranted and is being planned
Presented by: Andrew O. Parsonson, MD, Macquarie University, Sydney, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: B7-H3 Targeting ADC in Castrate-Resistant Prostate Cancer Trial - Andrew Parsonson