(UroToday.com) The 2025 ASCO annual meeting featured a prostate cancer rapid oral abstract session and a presentation by Dr. Capucine Baldini discussing phase 1 results of JNJ-78278343 (pasritamig) in metastatic castration-resistant prostate cancer (mCRPC).
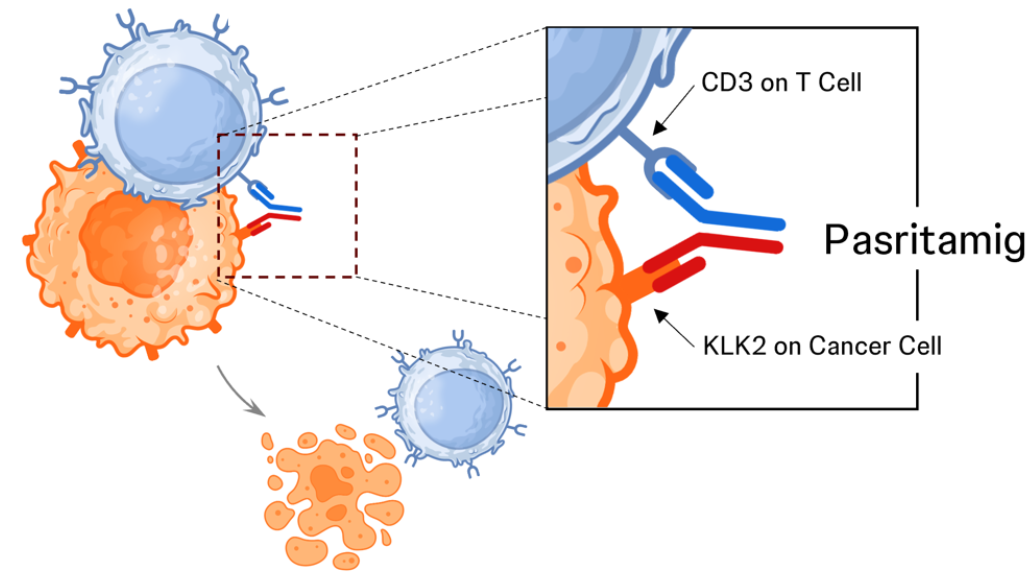
Human kallikrein 2 (encoded by the KLK2 gene) is a novel target expressed on prostate cancer cells with limited normal tissue expression. Pasritamig is a first-in-class T-cell-redirecting bispecific antibody targeting human kallikrein 2. Pasritamig simultaneously binds KLK2 on prostate cancer cells and CD3 receptor complexes on T cells, leading to T-cell activation and subsequent lysis of cancer cells:
At the 2025 ASCO annual meeting, Dr. Baldini reported dose escalation and expansion results from a first-in-human study evaluating pasritamig in patients with mCRPC.
Pasritamig target doses were escalated from 0.5-2000 mg SC and 150-900 mg IV QW-Q6W, with various step-up dosing schedules. Pre-medication with dexamethasone (16 mg) was required in step-up and first target dose. The primary objective was to determine the safety and the recommended phase 2 dose, whereas secondary objectives included preliminary assessment of antitumor activity: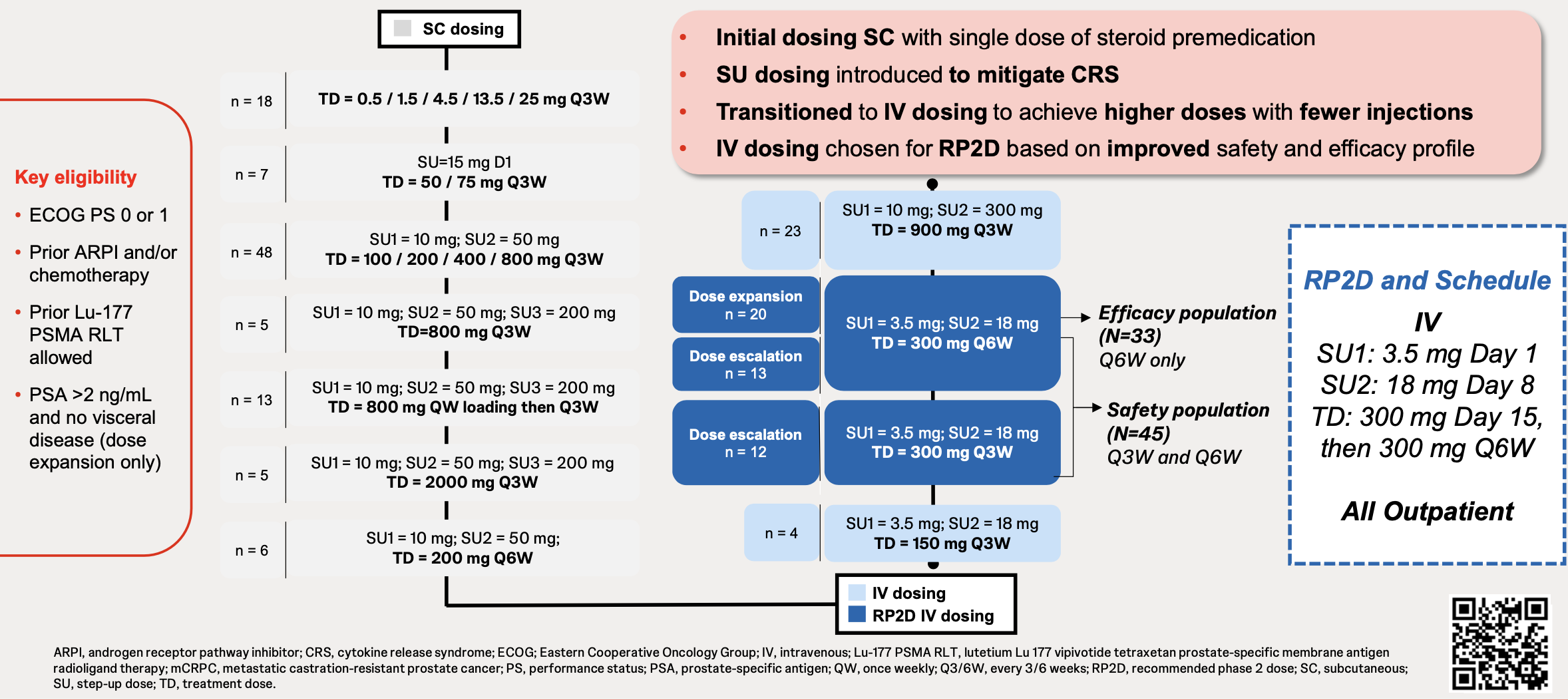 As of March 7, 2025, 174 patients (median age 69 [range: 36-89] years) had received ≥1 pasritamig dose. Patients had a median of 4 prior therapies (range 1-13; 99.4% androgen receptor pathway inhibitor, 78.2% taxane chemotherapy, 17.8% 177Lu-PSMA-617):
As of March 7, 2025, 174 patients (median age 69 [range: 36-89] years) had received ≥1 pasritamig dose. Patients had a median of 4 prior therapies (range 1-13; 99.4% androgen receptor pathway inhibitor, 78.2% taxane chemotherapy, 17.8% 177Lu-PSMA-617):
![As of March 7, 2025, 174 patients (median age 69 [range: 36-89] years) had received ≥1 pasritamig dose. Patients had a median of 4 prior therapies (range 1-13; 99.4% androgen receptor pathway inhibitor, 78.2% taxane chemotherapy, 17.8% 177Lu-PSMA-617):](/images/a98d027d-7162-4377-b455-473cc10479cd.png) There were no pasritamig-related deaths. One patient experienced a dose limiting toxicity of transient grade 3 ALT/AST elevation after 50 mg step-up 2 SC administration. While most patients reported ≥1 treatment related adverse events (82.8% overall), these were mostly low grade, with only 9.8% of patients experiencing a grade ≥3 treatment related adverse event:
There were no pasritamig-related deaths. One patient experienced a dose limiting toxicity of transient grade 3 ALT/AST elevation after 50 mg step-up 2 SC administration. While most patients reported ≥1 treatment related adverse events (82.8% overall), these were mostly low grade, with only 9.8% of patients experiencing a grade ≥3 treatment related adverse event: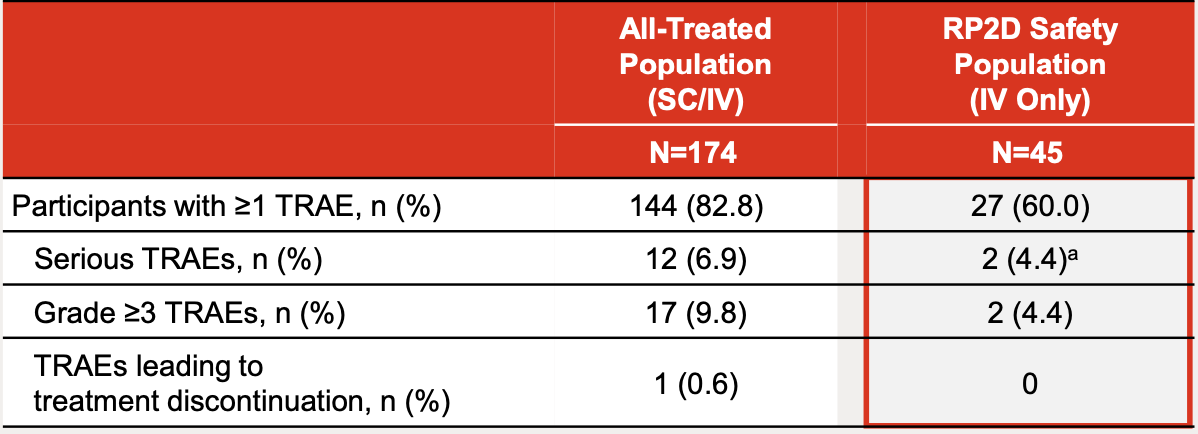
In the recommended phase 2 dose safety population (n = 45; 3.5 mg [Day 1], 18 mg [Day 8], 300 mg Q3W or Q6W IV), the most common treatment related adverse events were infusion-related reactions (24.4%; grade 1/2), fatigue (15.6%; grade 1/2), and cytokine release syndrome (8.9%; all grade 1, no tocilizumab was administered). No treatment related adverse events led to treatment discontinuation, no immune effector cell-associated neurotoxicity syndrome was observed, and 2 serious treatment related adverse events (grade 1 cytokine release syndrome) were reported.
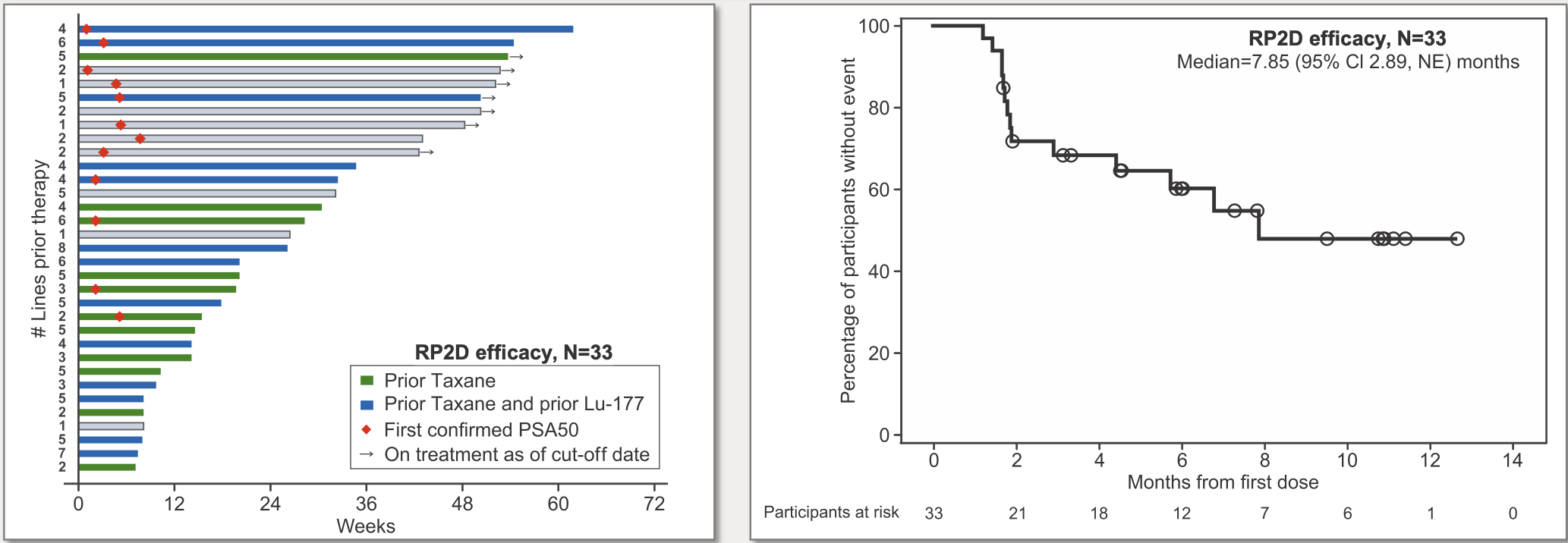
In the recommended phase 2 dose efficacy population (n = 33; 3.5 mg [Day 1], 18 mg [Day 8], 300 mg Q6W IV), PSA50 was 42.4% (14/33):
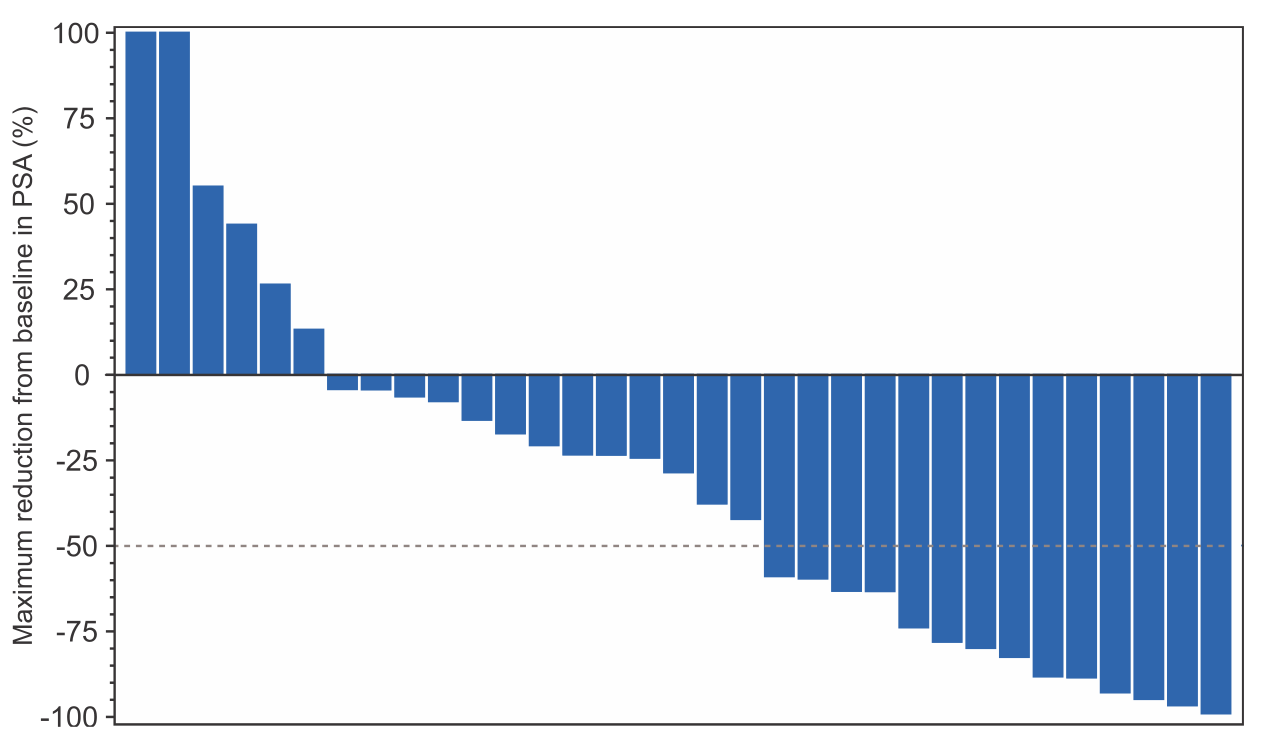 The objective response rate in the 84 patients with measurable disease was 8.3% and the median duration of response of 8.9 (95% CI 3.6, NE) months. In the recommended phase 2 dose efficacy population, the median radiographic progression free survival was 7.9 (95% CI 2.9, NE) months, with 21.2% of patients with treatment ongoing. PSA50 responses and durable disease control were observed irrespective of prior treatment with taxanes or PSMA targeted radioligand therapy:
The objective response rate in the 84 patients with measurable disease was 8.3% and the median duration of response of 8.9 (95% CI 3.6, NE) months. In the recommended phase 2 dose efficacy population, the median radiographic progression free survival was 7.9 (95% CI 2.9, NE) months, with 21.2% of patients with treatment ongoing. PSA50 responses and durable disease control were observed irrespective of prior treatment with taxanes or PSMA targeted radioligand therapy:
Dr. Baldini concluded her presentation discussing phase 1 results of JNJ-78278343 (pasritamig) in mCRPC with the following take-home points:
- Pasritamig demonstrated a remarkable safety profile:
- Low rates of treatment related adverse events and infrequent cytokine release syndrome (only Grade 1) with no tocilizumab use
- Safety of the recommended phase 2 dose regimen allowed for outpatient dosing on a patient friendly, every 6 week schedule
- This facilitates utilization of T-cell engagers in a community oncology setting
- Safety and convenience of the recommended phase 2 regimen readily supports monotherapy and combination therapy approaches
- Pasritamig achieved durable responses and radiographic progression free survival that compared favorably to historical data in heavily pretreated participants with mCRPC
- Multiple pivotal studies of pasritamig are being developed
Presented by: Capucine Baldini, MD, Institut Gustave Roussy, Villejuif, France
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: Pasritamig Safety and Efficacy Data from Metastatic CRPC Phase I Study - Capucine Baldini