(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to the Poster Session: Genitourinary Cancer - Kidney and Bladder. Darren R. Feldman, MD, presented the trial in progress Poster TPS4612: STARLITE 2: Phase 2 study of nivolumab plus 177lutetium-labeled anti–carbonic anhydrase IX (CAIX) monoclonal antibody girentuximab (177Lu-girentuximab) in patients with advanced clear cell renal cell carcinoma (ccRCC).
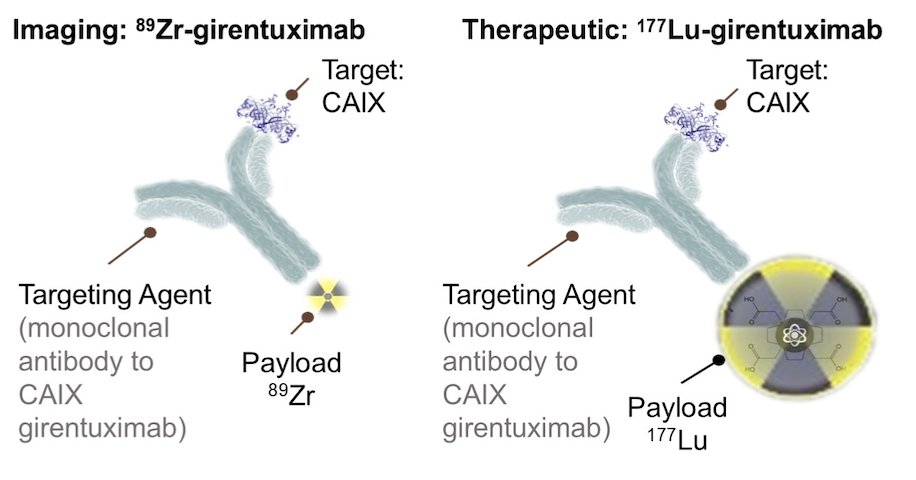
Carbonic anhydrase IX (CAIX) is a cell surface glycoprotein expressed in over 90% of clear cell renal cell carcinoma (ccRCC) but rarely found in normal tissues, making it a promising target for both imaging and therapeutic applications. Radiolabeling the anti-CAIX monoclonal antibody girentuximab with zirconium-89 (⁸⁹Zr) has demonstrated potential as a positron emission tomography (PET) tracer for detecting ccRCC.1 Additionally, labeling girentuximab with lutetium-177 (¹⁷⁷Lu) presents a compelling therapeutic approach, as targeted radiation delivery to ccRCC cells may enhance tumor antigen presentation and prime the immune response. This provides a strong rationale for combining ¹⁷⁷Lu-girentuximab with nivolumab to potentially improve treatment outcomes.2 A graphic representation of anti-CAIX monoclonal antibody girentuximab with zirconium-89 (⁸⁹Zr) or ¹⁷⁷Lu-girentuximab is shown below.
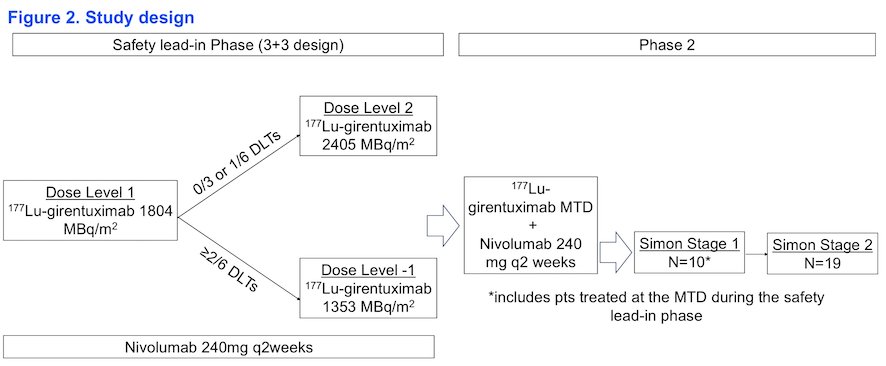
The STARLITE 2 trial is a phase 2, open-label, single-arm study evaluating the combination of lutetium-177 (¹⁷⁷Lu)-girentuximab and nivolumab in patients with previously treated ccRCC. The study includes a safety lead-in phase to determine the maximum tolerated dose (MTD) of ¹⁷⁷Lu-girentuximab in combination with nivolumab, starting at 75% of the single-agent ¹⁷⁷Lu dose. Once the MTD is established, a Simon two-stage design will be implemented to assess the efficacy of this combination. Patients treated at the MTD during the safety lead-in will be included in the first stage of the phase 2 portion. Notably, the prespecified number of dose-limiting toxicities (DLTs) was exceeded in cohort 2, leading to a dose adjustment back to 1804 MBq/m².
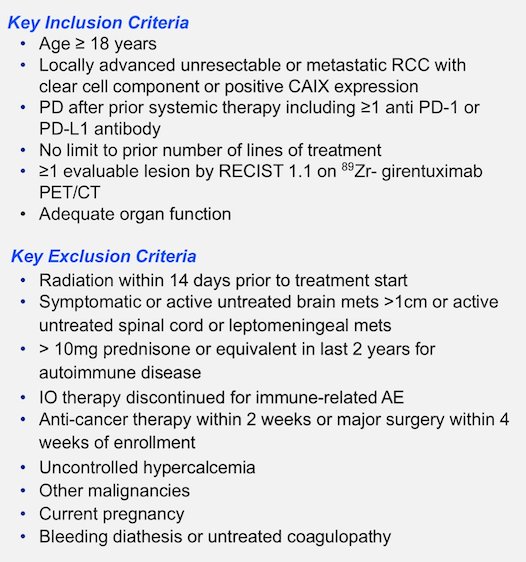
The inclusion criteria for STARLITE 2 require patients to have biopsy-confirmed ccRCC or demonstrate CAIX expression. Eligible patients must have progressive disease following at least one prior immunotherapy agent, adequate organ and bone marrow function, and at least one measurable lesion per RECIST 1.1 that is also avid on ⁸⁹Zr-girentuximab PET. There is no restriction on the number of prior systemic therapy lines; however, patients who discontinued immunotherapy due to immune-related toxicity are excluded from enrollment. Key inclusion and exclusion criteria are summarized below.
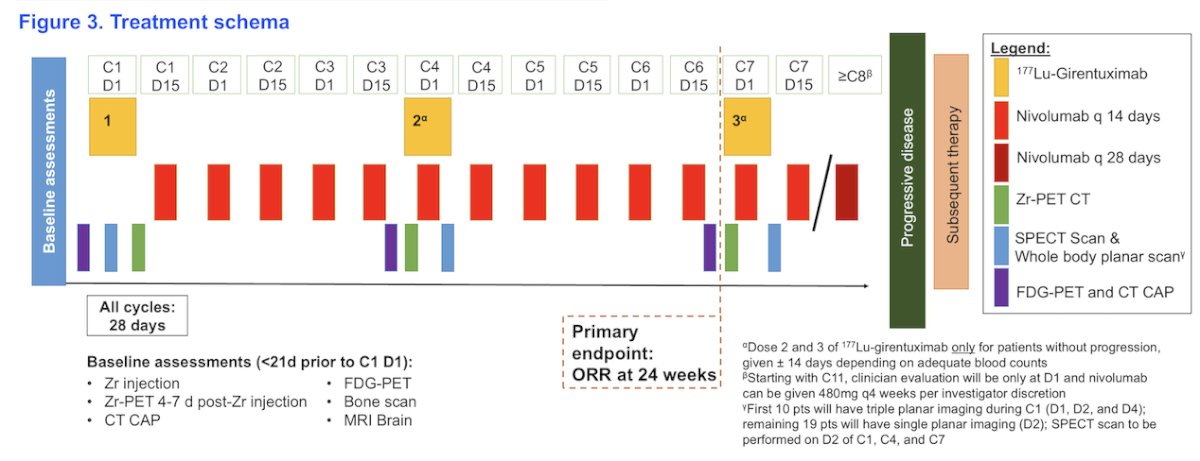
Treatment consists of 28-day cycles. Cycle 1, day 1 (C1D1) is the date of the first 177Lu-girentuximab dose, with subsequent doses administered every 12-14 weeks (e.g., C4D1 and C7D1) for a maximum of three doses. Dose 2 of 177Lu-girentuximab is 75% of Dose 1, and Dose 3 is 75% of Dose 2. Nivolumab 240 mg is given on D1 and D15 of all cycles except C1D1, where the first nivolumab dose is administered on C1D15. Starting with C10, nivolumab may be switched to 480 mg q4 weeks. The treatment schema is shown below.
The primary endpoints are divided in two phases:
- Safety lead-in: Establish MTD of 177 Lu-girentuximab in combination with nivolumab
- DLT in 0/3 or 1/6 patients is considered acceptable
- Probability of dose escalation is 0.91 if the true DLT rate is 20% and 0.71 if it is 30%
- Phase 2 Portion: Best ORR by RECIST 1.1 within 24 weeks
- Simon two stage optimal design to differentiation ORR of 5% (uninteresting) vs. 20% (worthy of further study) with a = 0.05 and power of 80%
- First stage: enroll 10 pts; if ≥ 1 response, proceed to stage 2
- Second stage: enroll 19 pts; if ≥ 4 responses out of all 29 patients, regimen will be considered worthy of further study
- Probability of early stopping is 0.60 if the true ORR is 5%
Key Secondary endpoints are:
- Best ORR by RECIST 1.1 at any timepoint
- Best ORR by investigator reported RECIST within 24 weeks and at any timepoint
- PFS and OS (Kaplan Meier method)
- Time free from skeletal-related events (Kaplan Meier method)
- Adverse event reporting using descriptive statistics (frequency)
Presented by: Darren R. Feldman, MD, Medical Oncologist at Memorial Sloan Kettering Cancer Center (MSKCC). New York, NY, United States.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Reference:
- Shuch B, Pantuck AJ, Bernhard JC, Morris MA, Master V, Scott AM, van Praet C, Bailly C, Önal B, Aksoy T, Merkx R, Schuster DM, Lee ST, Pandit-Taskar N, Fan AC, Allman P, Schmidt K, Tauchmanova L, Wheatcroft M, Behrenbruch C, Hayward CRW, Mulders P. [89Zr]Zr-girentuximab for PET-CT imaging of clear-cell renal cell carcinoma: a prospective, open-label, multicentre, phase 3 trial. Lancet Oncol. 2024 Oct;25(10):1277-1287. doi: 10.1016/S1470-2045(24)00402-9. Epub 2024 Sep 10. PMID: 39270701.
- Muselaers CH, Boers-Sonderen MJ, van Oostenbrugge TJ, Boerman OC, Desar IM, Stillebroer AB, Mulder SF, van Herpen CM, Langenhuijsen JF, Oosterwijk E, Oyen WJ, Mulders PF. Phase 2 Study of Lutetium 177-Labeled Anti-Carbonic Anhydrase IX Monoclonal Antibody Girentuximab in Patients with Advanced Renal Cell Carcinoma. Eur Urol. 2016 May;69(5):767-70. doi: 10.1016/j.eururo.2015.11.033. Epub 2015 Dec 23. PMID: 26706103.