(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting, held in Chicago, IL, was host to a kidney and bladder cancers oral abstract session. Dr. Tian Zhang discussed the four prior oral abstract presentations:
- Nivolumab plus ipilimumab vs sunitinib for first-line treatment of advanced renal cell carcinoma: Final analysis from the phase 3 CheckMate 214 trial
- Combination of casdatifan plus cabozantinib expansion cohort of phase 1 ARC-20 study in previously treated patients with clear cell renal cell carcinoma
- Hypoxia-inducible factor-2α (HIF-2α) inhibitor belzutifan in von Hippel-Lindau (VHL) disease–associated neoplasms: 5-year follow-up of the phase 2 LITESPARK-004 study
- ALLO-316 in advanced clear cell renal cell carcinoma (ccRCC): Updated results from the phase 1 TRAVERSE study
The key takeaway points from each of these abstracts were as follows:
- Immunotherapy doublets remain standard of care for metastatic RCC – longest follow up from Checkmate 214 with durable responses
- Long term follow-up of belzutifan in VHL syndrome
- The combination effect of casdatifan and cabozantinib shows activity in refractory clear cell RCC – sets up phase III trial
- Second allogeneic T-cell therapy in metastatic RCC – early cellular therapies for solid tumors
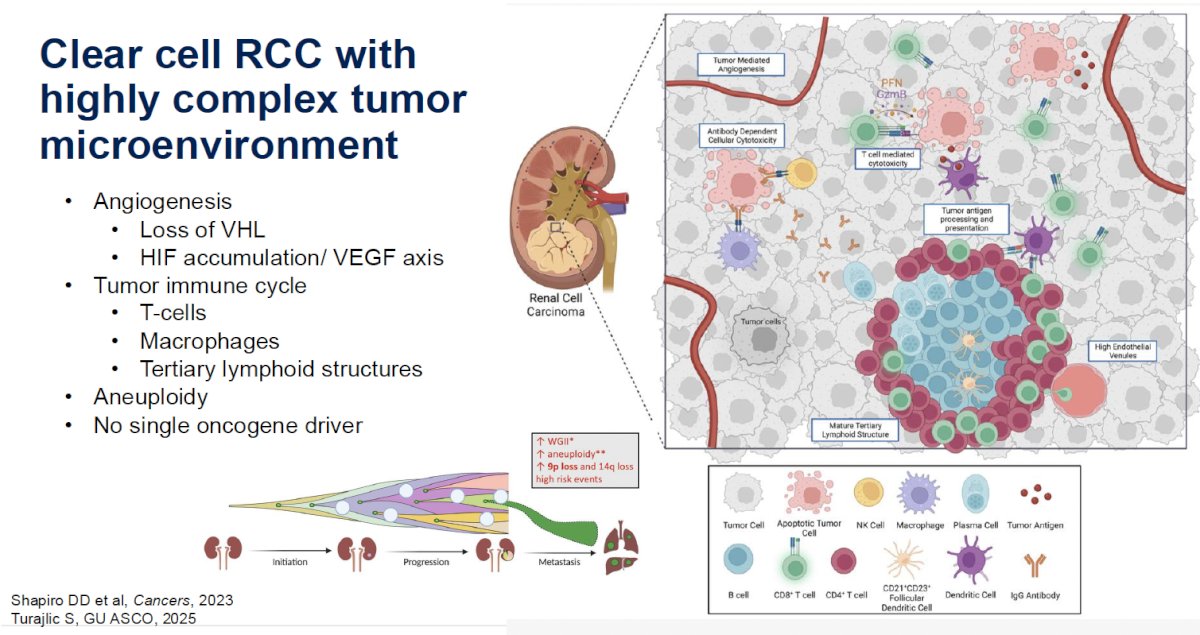
Clear cell RCC is underlined by a highly complex tumor microenvironment, with aberrant angiogenesis pathways involving VHL loss and HIF accumulation, tumor immune cycle derangements, involving T-cells, macrophages, and tertiary lymphoid structures, and aneuploidy. Notably, not a single oncogenic driver has been identified to date. This tumor microenvironment complexity thus often requires the targeting of numerous pathways to achieve tumoral cell death.
Despite these challenges, checkpoint inhibitors have clearly made a ‘remarkable’ difference in the outcomes of clear cell RCC patients. The reported 9-year follow-up from the CheckMate 214 trial by Motzer et al. represents the longest follow-up to date of immune checkpoint inhibitor therapy in a cohort of metastatic RCC patients. As highlighted in the blue circle below, 31% of patients in the nivolumab + ipilimumab arm remained alive at 9 years – a remarkable achievement in a cohort of metastatic RCC patients.
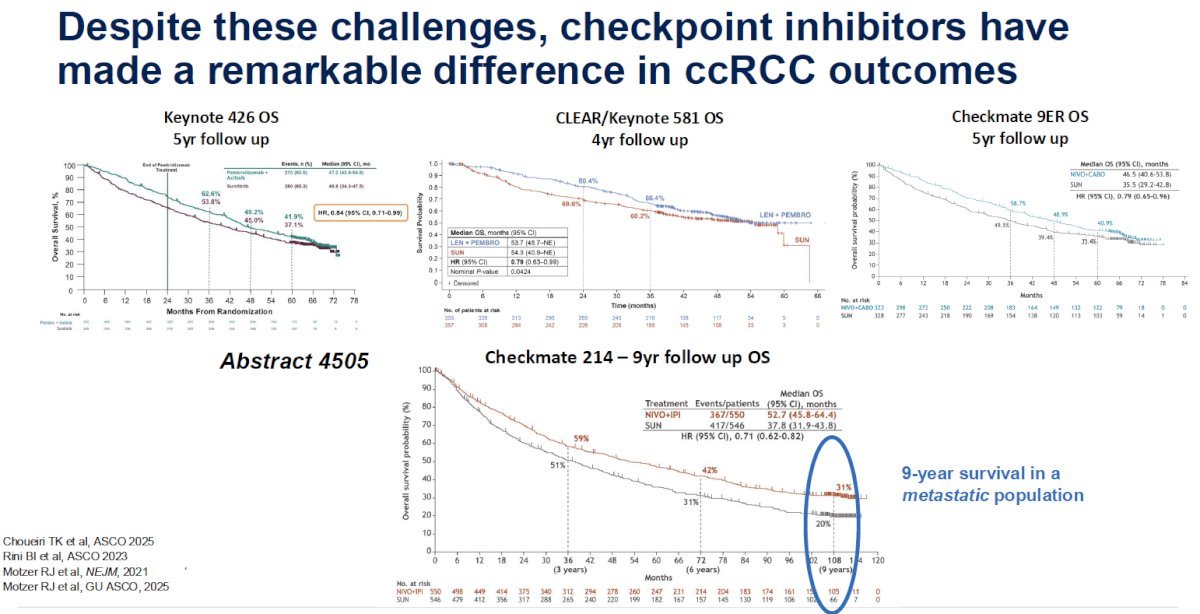
However, upon further review, Dr. Zhang noted that there were only 64 non-censored/alive patients who remained ‘at risk’ at the 6-year mark. As such, she argued that the 6-year rates are likely the last dependable data from this trial.

Summarized below are the next generation of 1st line RCC trials that include checkpoint inhibitor therapy as the foundational piece of the investigational treatment approach. These approaches include triplet systemic therapy regimens, adaptive/sequential, and multi-disciplinary treatments. She highlighted PROBE, which incorporates consolidative nephrectomy into the investigational treatment paradigm, and SOAR, SAMURAI, and CYTOSHRINK, which include SBRT to the oligometastases or primary disease site.

Trials in the 1st line setting are also incorporating biomarkers for treatment selection, with the CARE-1 trial comparing IO-IO to IO-TKI therapy in two separate cohorts of patients: PD-L1+ (~25%) and PD-L1- (~75%).

Next, Dr. Zhang discussed the VHL syndrome and the rationale behind targeting HIF-2α. The HIF-VHL pathway is critical to RCC pathogenesis. Under normal oxygen conditions, VHL causes ubiquitination of HIF and targets it for proteosomal degradation. However, when VHL is lost, HIF accumulates in the cell – the alpha and beta units dimerize, translocate into the nucleus, and bind to the hypoxia response elements, causing activation of downstream target genes. This leads to increased angiogenesis, cell survival, tumor growth, and all other hallmarks of RCC development.
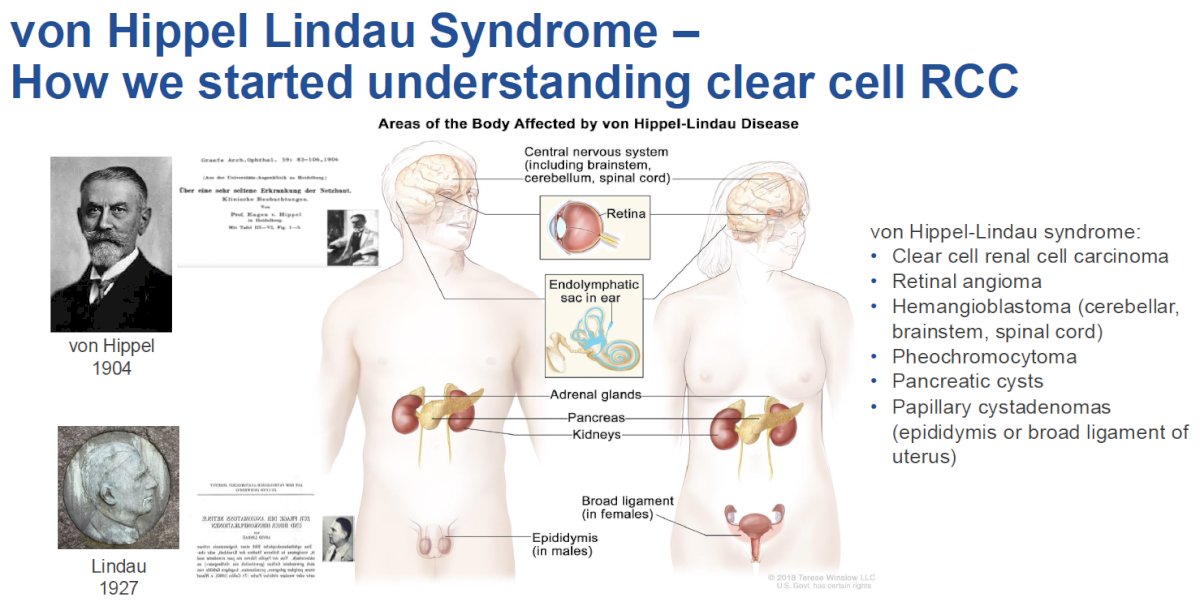
In 1904, Dr. Eugene von Hippel, a German ophthalmologist, 1st described angiomas in the eye. In 1927, Arvid Lindau, a Swedish pathologist, 1st described angiomas in the cerebellum and spine. In 1936, the term Von Hippel-Lindau disease was 1st used. VHL is an autosomal dominant syndrome, with 80% of patients having an affected parent, while 20% arise de novo. Nearly all patients will express the syndrome by age 65. The incidence of this syndrome is 1 in 36,000, and roughly two-thirds will develop an RCC.
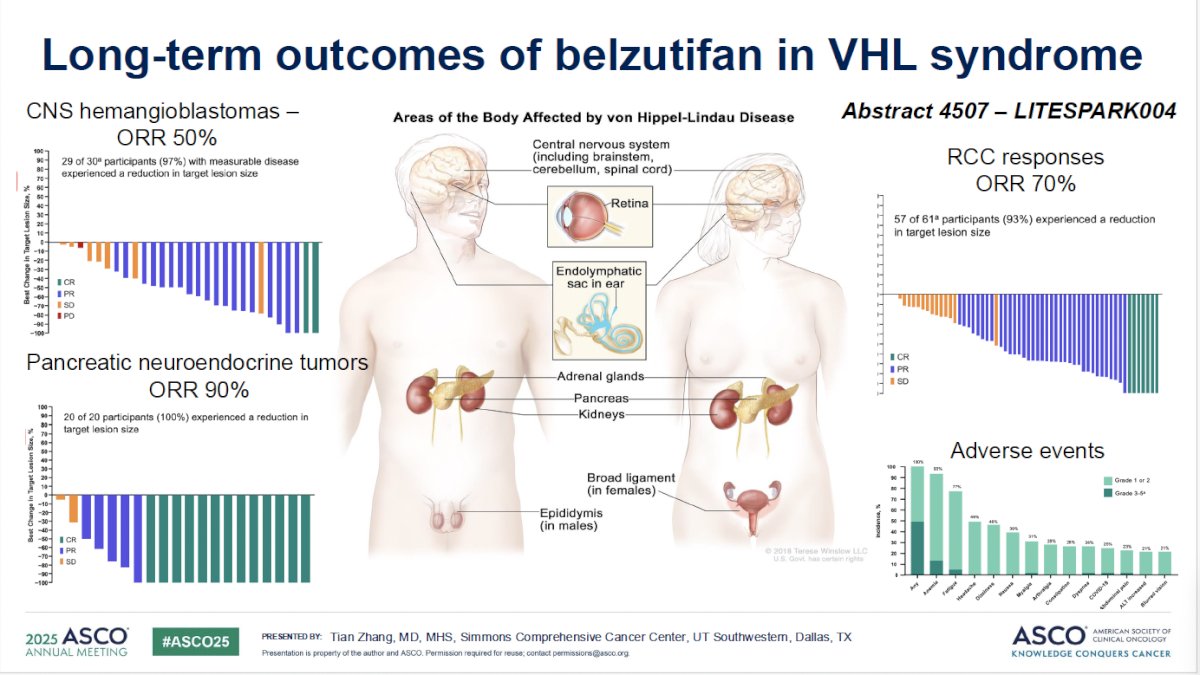
LITESPARK-004 is a phase II trial that included patients with a VHL syndrome diagnosis, ≥1 measurable RCC tumor, and no prior systemic therapy for RCC. The ORR was 70.5%. A complete response (CR) was observed in 7 (11%) patients and a partial response (PR) in 36 (59%). The ORRs in other tumors were as follows:
- CNS hemangioblastomas: 50%
- Pancreatic neuroendocrine tumors: 90%
- Retinal hemangioblastomas: 100%
All participants experienced ≥1 treatment-related adverse event (TRAE). There were no grade 4–5 TRAEs observed.
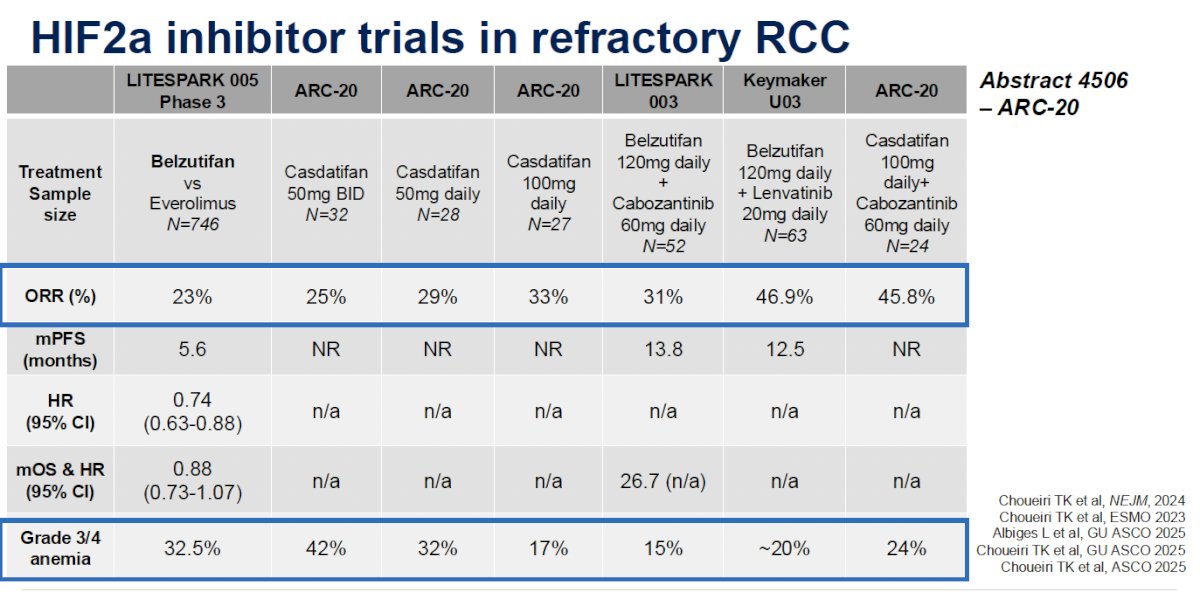
While LITESPARK-004 included treatment-naïve patients, how do trials of HIF-2α inhibitor therapy in refractory RCC compare?
- LITESPARK-005: Belzutifan versus everolimus
- ORR: 23%
- LITESPARK-003: Belzutifan + cabozantinib
- ORR: 31%
- Keymaker U03:Belzutifan + lenvatinib
- ORR: 47%
- ARC-20 is a phase I dose-escalation and dose-expansion study of casdatifan, a novel HIF-2α inhibitor
- Dose-escalation cohort: Casdatifan monotherapy doses from 20 mg once daily to 200 mg once daily are being evaluated
- ORRs: 25–33%
- Dose-expansion cohort: Casdatifan combination
- 46%
- Dose-escalation cohort: Casdatifan monotherapy doses from 20 mg once daily to 200 mg once daily are being evaluated
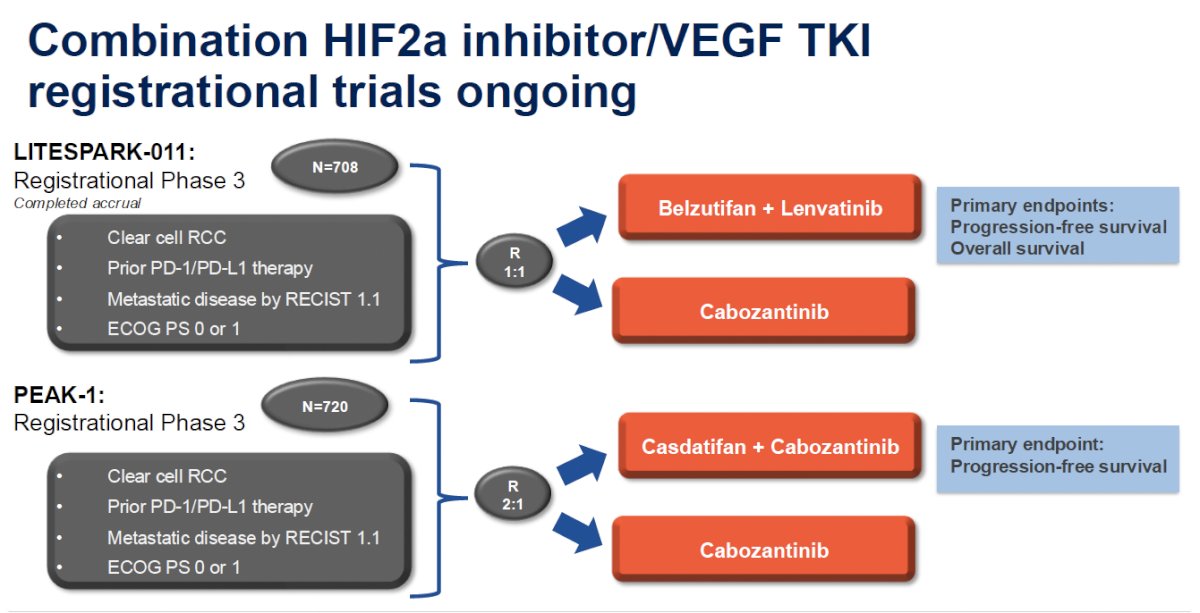
Ongoing registrational trials of combination HIF-2α inhibitor therapy + VEGF-TKIs include:
- LITESPARK-011: Belzutifan + lenvatinib versus cabozantinib
- PEAK-1: Casdatifan + cabozantinib versus cabozantinib
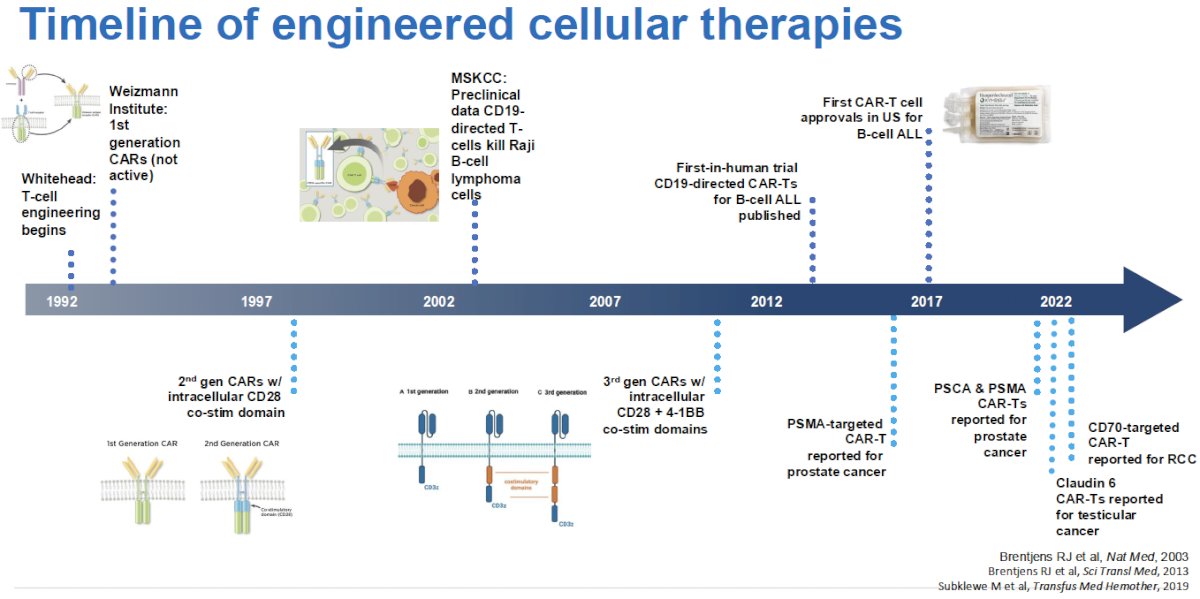
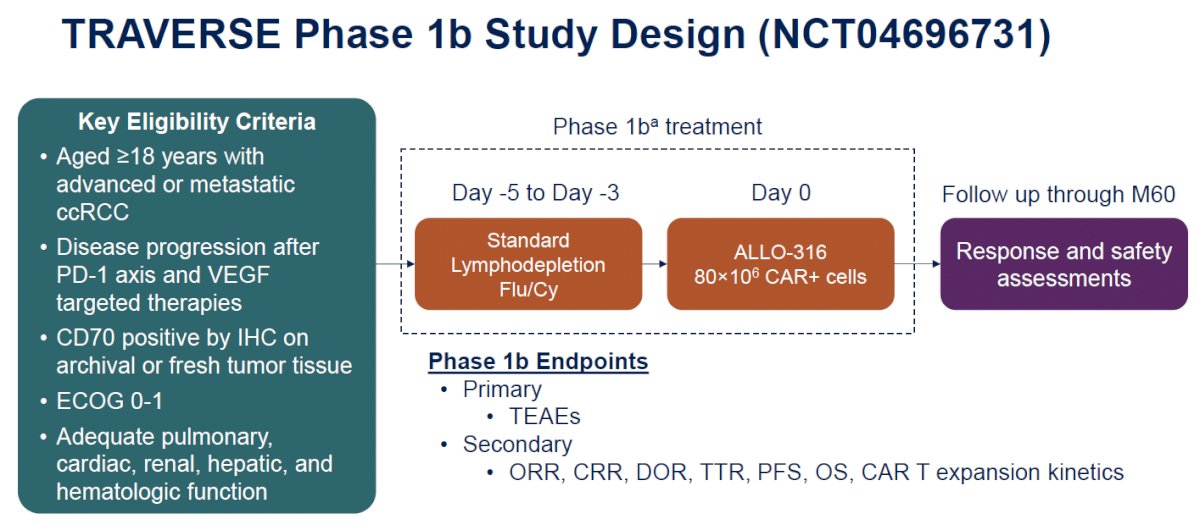
In the last portion of her discussion, Dr. Zhang discussed the oral abstract presentation of ALLO-316 in the phase I TRAVERSE study presented earlier by Dr. Srour. She noted that CAR T therapy has revolutionized the treatment of hematologic malignancies, but progress in solid tumors has been slow.1
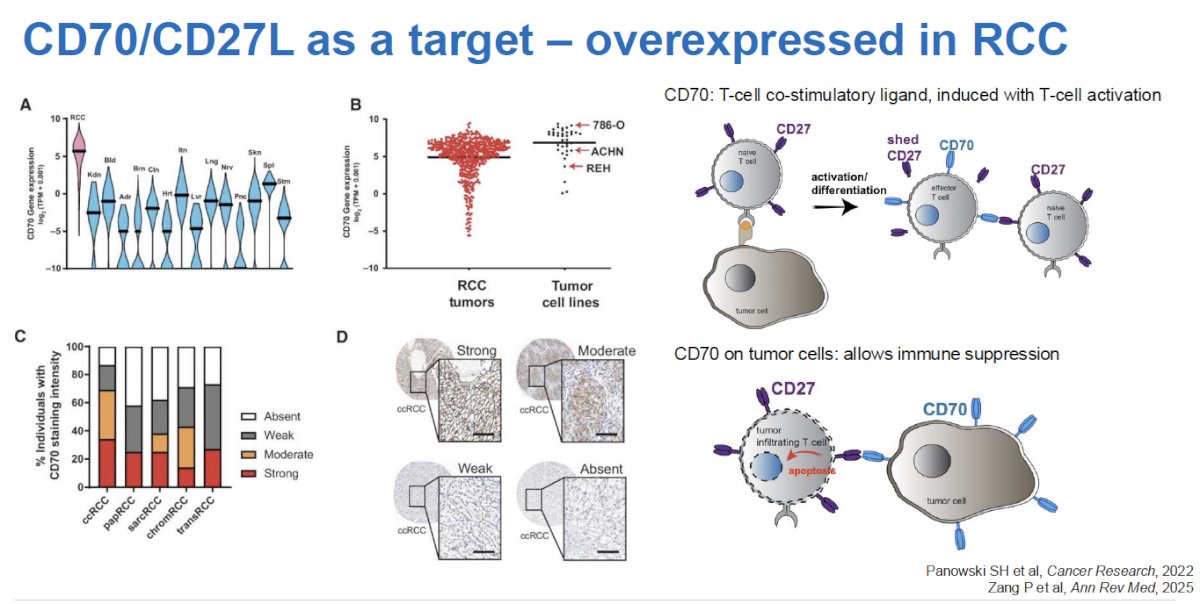
ALLO-316 is an off-the-shelf, HLA-unmatched allogeneic CD70 CAR T product designed to target both CD70+ tumors and alloreactive host T cells.
Phase Ia data from the TRAVERSE study of ALLO-316 in patients with clear cell RCC showed manageable safety with promising antitumor activity.2 The results from 20 heavily pre-treated, refractory patients in the phase Ib part of the study, treated with standard lymphodepletion and 80M CD70 CAR T cells, were reported by Dr. Srour earlier in this session. Dr. Zhang noted that this trial included a highly treatment refractory patient cohort – patients had received a median of 4 prior lines of therapy (32% were quadruple class refractory to inhibition of the CTLA-4, PD-(L)1, TKI, and HIF-2α pathways). The dose of 80 x 106 cells was the recommended dose for this phase Ib portion, with 2 prior dose-limiting toxicities experienced at higher doses (autoimmune hepatitis and cardiogenic shock/multi-organ failure; failure to thrive and sepsis led to 2 other grade 5 events).
The adverse event profile was consistent with that of lymphodepletion and an active CAR T therapy (i.e., cytokine release, infection, hemophagocytic syndrome). Any-grade TEAEs occurred in 100% of phase 1b patients, including:
- Majority of Grade ≥3 TEAEs were hematologic in nature
- No treatment-related Grade 5 AEs were observed

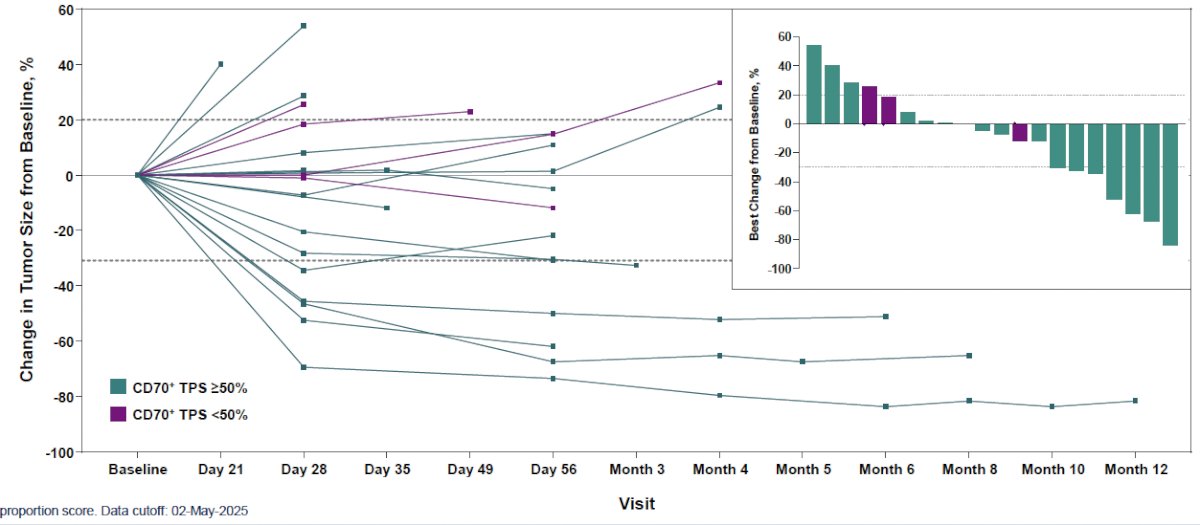
In the 20 patients from the phase 1b portion with evaluable efficacy data, an ORR was observed in 25% (5/20). All ORRs were observed in patients with a CD70+ tumor proportion score (TPS) ≥50%.

Tumor responses occurred early and were sustained following a single infusion of ALLO-316. Among CD70+ TPS ≥50% patients, 44% (7/16) had >30% reduction in the diameters of baseline target lesions.
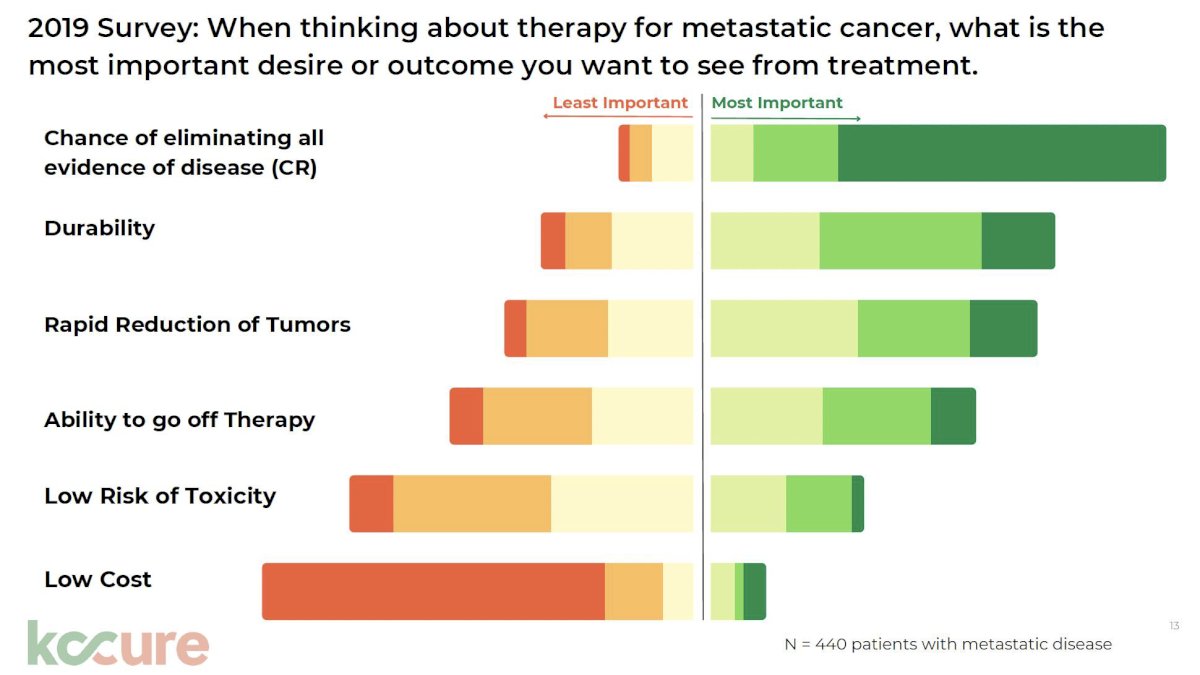
She emphasized that these prolonged responses are particularly relevant given that significant, consistent data from patient advocacy groups suggest that deep, durable responses are one of, if not the, main patient priority – ‘our patients want deep and durable responses’.
Dr. Zhang concluded this discussion with the following key takeaway points:
- Immunotherapy doublets remain standard of care for metastatic RCC
- Emerging treatments will improve multiprong treatment approaches in kidney cancer
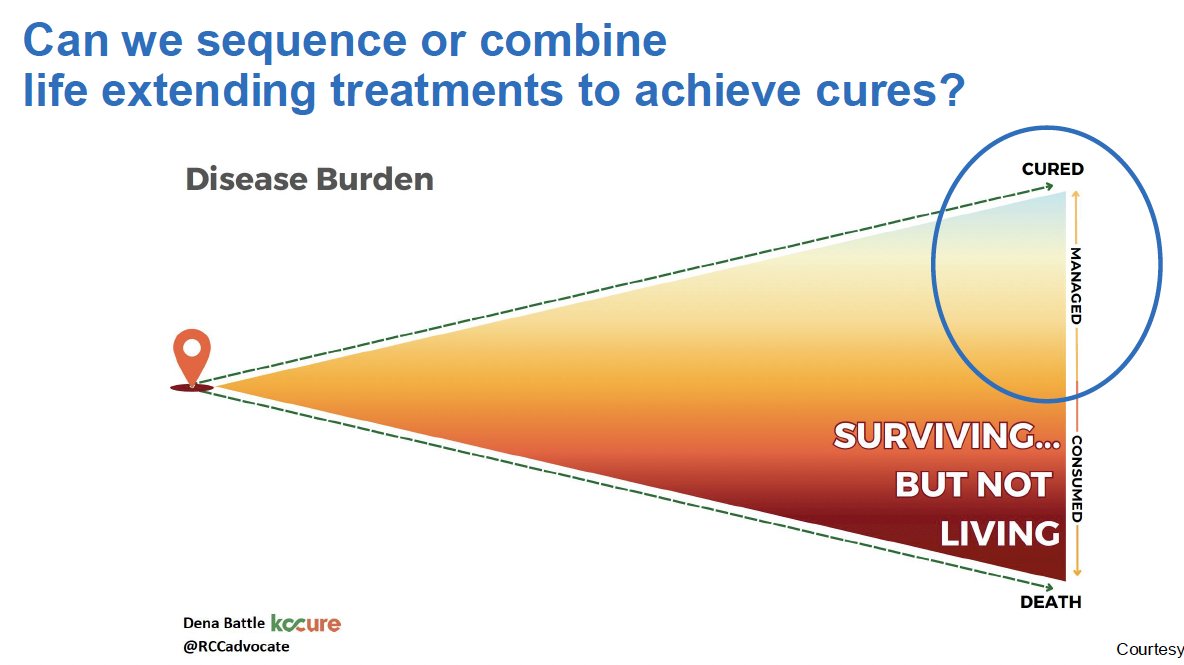
- We should aim for a future in RCC with more cures and deep, durable responses
Presented by: Tian Zhang, MD, MHS, Associate Professor, Department of Internal Medicine, UT Southwestern Medical Center, Dallas, TX
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:
- Albelda SM, June CH, Wherry EJ, et al. Immune resistance in cancer: strategies for clinical translation. Nat Rev Clin Oncol. 2024; 21:47–66.
- Srour SA, Smith L, Johnson K, et al. Emerging immunotherapy combinations in solid tumors: insights from preclinical models. J Immunother Cancer. 2024; 12(Suppl 2):A1–A1683.