(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting, held in Chicago, IL, was host to a biomarkers in kidney cancer session. Dr. David McDermott discussed the ongoing search for kidney cancer biomarkers, highlighting the following key takeaway points that form the framework of this discussion:
- Integrated models are the future of biomarker discovery
- Hypothesis driven biomarker efforts can lead to novel therapies
- Translational research will lead to more cures

Discussing integrated models as the future of biomarker discovery, Dr. McDermott noted: “Given the complexity of the RCC, it is likely that numerous biomarkers will need to be integrated to have true utility as a predictive tool:
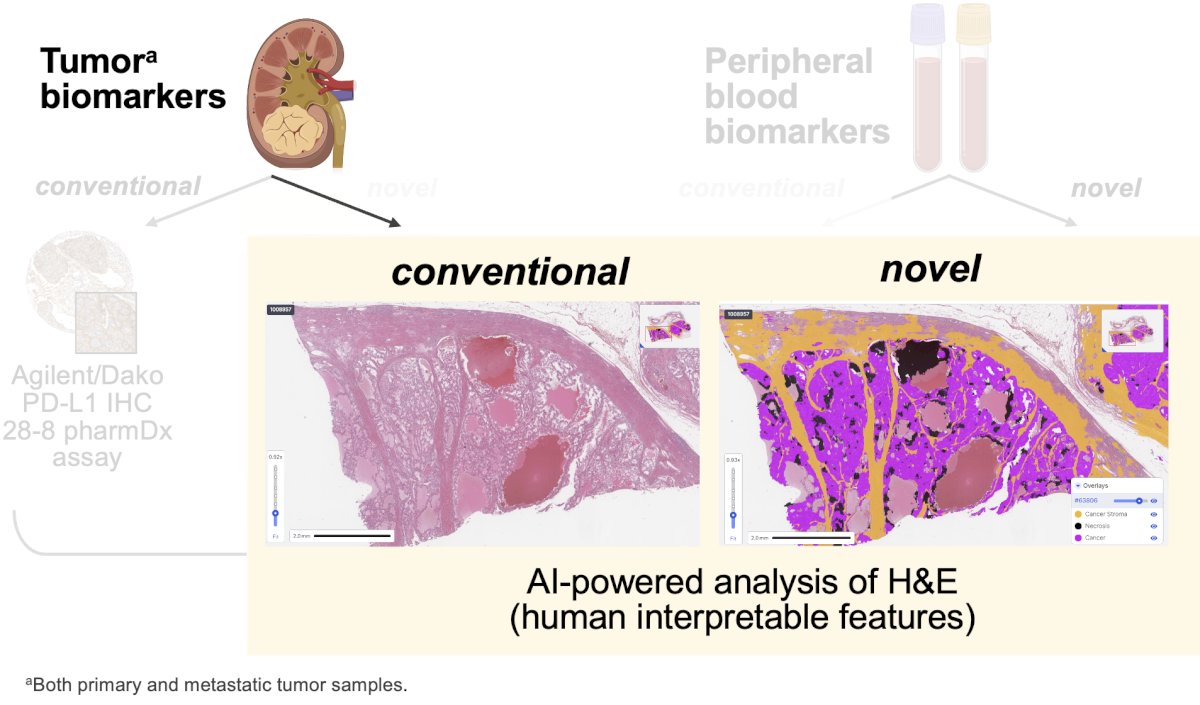
To this end, he highlighted the abstract presented earlier by Dr. Braun: “An integrative analysis of circulating and tumor microenvironment determinants of patient response in the Checkmate 9ER trial of nivolumab and cabozantinib in advanced renal cell carcinoma”. In this ad hoc analysis of the CheckMate-9ER trial, Dr. Braun and colleagues utilized tumor (primary and metastatic) and peripheral blood biomarkers in an integrated manner to predict clinical outcomes and treatment responses.

H&E-stained whole-slide images were analyzed using artificial intelligence (AI)-powered platforms (PathExplore, PathAI) to achieve single-cell resolution mapping of the tumor microenvironment (TME). Human interpretable features included cell type proportions, spatial architecture, and phenotypes, and were used to support biomarker discovery and patient stratification. The human interpretable features were integrated with clinical data to support exploratory analyses and outcome association studies.
What were the lessons learned from this study?
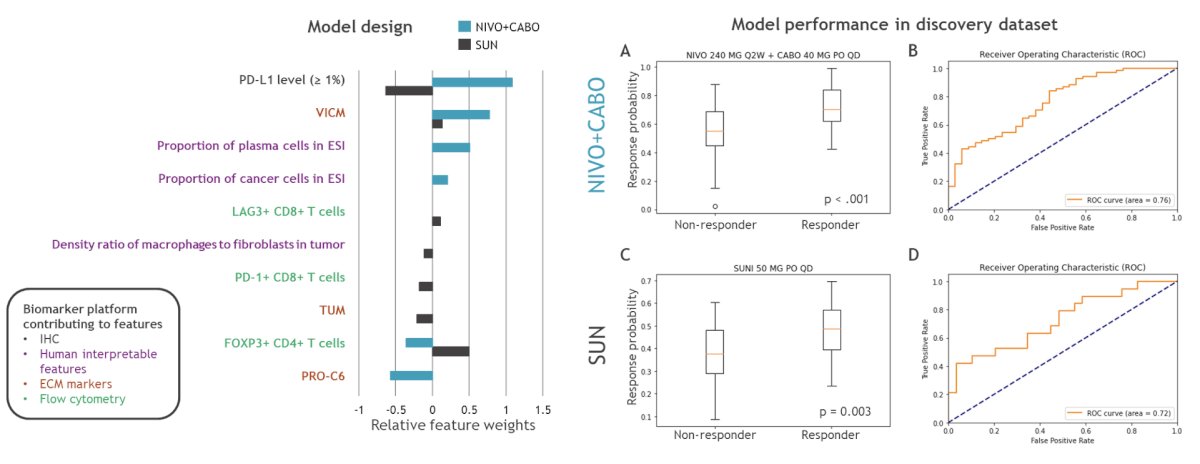
- This multi-source, multi-interpreter (Human + Machine Learning [ML]) model improves the clustering of patients who are more or less likely to benefit from treatment
- Incorporation of AI/ML into biomarker analysis has the potential to reveal what the human eye cannot see and uncover new biology
- Input from human RCC pathologists, however, remains a critical component of obtaining reproducible results
- Putative biomarkers identified included:
- Tissue-resident macrophages and low circulating T-regs were associated with superior outcomes
- Extracellular matrix (ECM) alterations were associated with inferior outcomes
- This study supports attempts to reverse immunosuppression (e.g., targeting TGFB1, T-regs) in RCC
- While this work uncovered new biology, the emerging model is not quite ready for validation
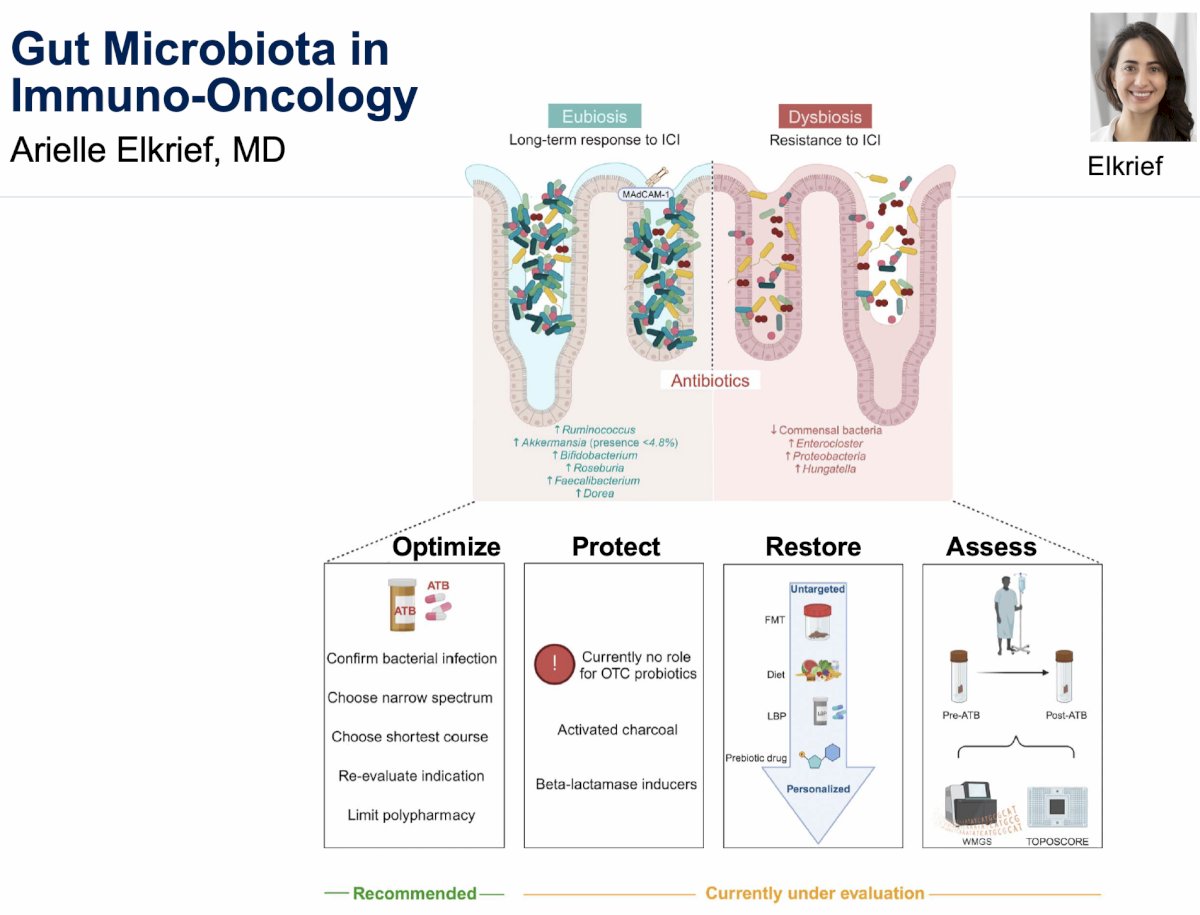
Next, Dr. McDermott discussed the prior presentation by Dr. Renee Saliby: “Gut-associated checkpoint as a prognostic biomarker in metastatic renal cell carcinoma (mRCC): Results from a randomized first-line clinical trial”. He first addressed the significant body of literature on the role of the gut microbiota in immune-oncology, highlighting the following:
- The gut microbiome may impact the efficacy and toxicity of ICIs
- Antibiotics produce gut dysbiosis and should be used sparingly with ICIs
- Gut microbiome interventions) may restore eubiosis and overcome primary and secondary ICI resistance
- Prospective trials are needed
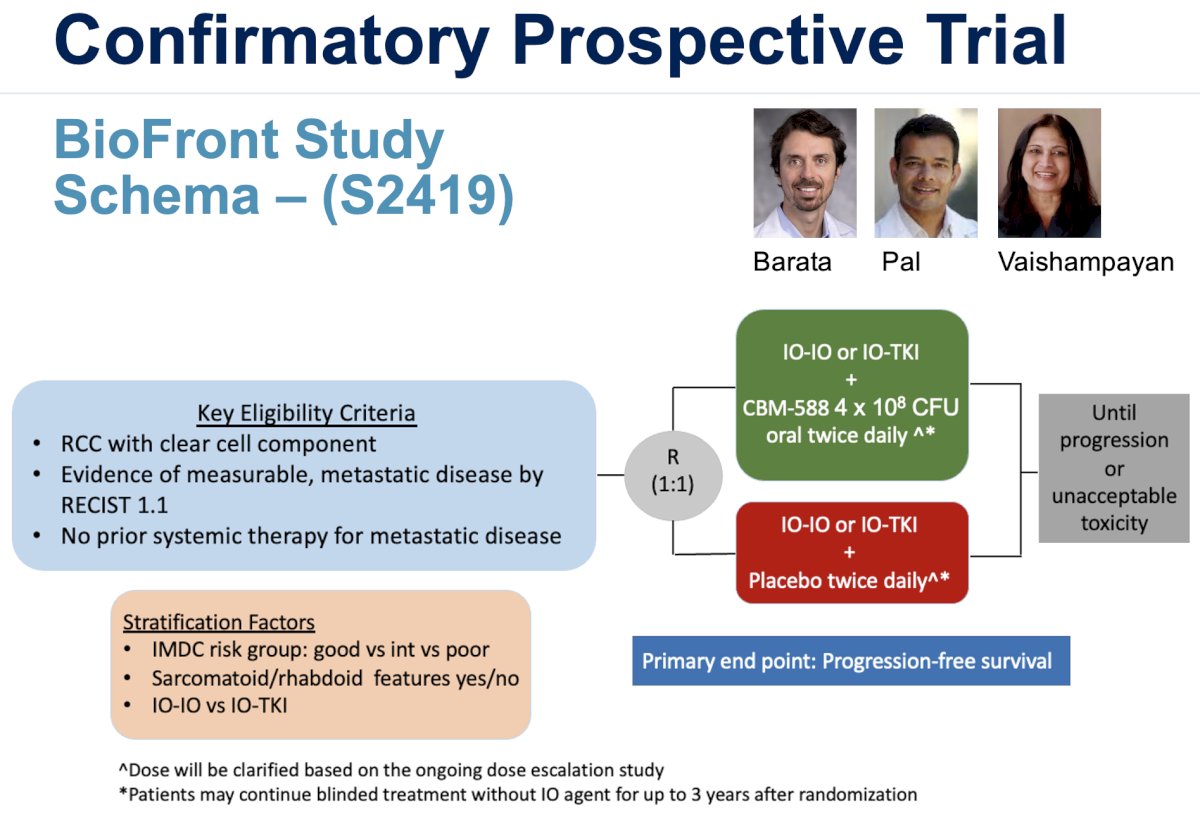
Numerous gut microbiome intervention trials are currently underway, all evaluating whether the addition of a liver bacterial product to ICI-based combination therapy influences treatment efficacy. These trials are of high potential significance given that a confirmed intervention from any trial would be translatable across ≥20 tumor types. One such trial is the BioFront study, which is evaluating ICI therapy (IO-IO or IO-TKI) +/- Clostridium butyricum (CBM-588) in metastatic clear cell RCC patients.
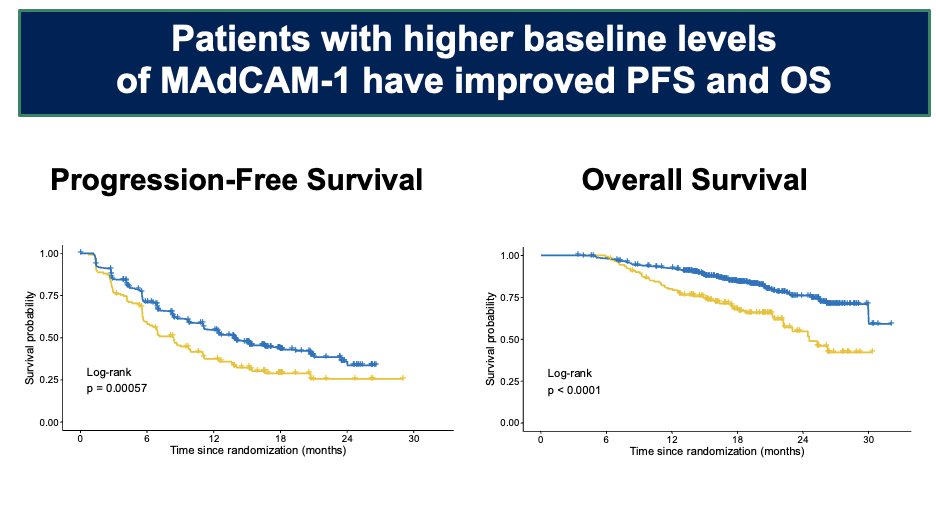
Discussing the abstract presentation by Saliby et al., he noted that this ad hoc analysis of the JAVELIN Renal 101 trial demonstrated that patients with higher baseline levels of MAdCAM-1 have improved progression-free and overall survival outcomes. Endothelial cell MAdCAM-1 expression keeps immunosuppressive T cells in the gut, and, thus, low serum MAdCAM-1 levels may reflect gut dysbiosis. In the current study, low serum MAdCAM-1 levels were associated with inferior survival outcomes in both study arms. This assay could potentially identify patients for gut microbiome interventions.
Next, Dr. McDermott discussed how hypothesis-driven biomarker efforts can lead to novel therapies. The NEOAVAX trial, presented by Dr. Axel Bex, was an open label, single arm, phase II trial investigating 12 weeks of neoadjuvant avelumab + axitinib prior to nephrectomy in patients with high-risk, non-metastatic clear cell RCC. This trial builds upon recent pivotal trials in other tumors (e.g., non-small cell lung cancer [NSCLC], melanoma) that have confirmed the impact of neoadjuvant PD-1 blockade on survival, with pre-surgical PD-1 blockade generating survival improvements by killing/controlling micrometastatic disease.
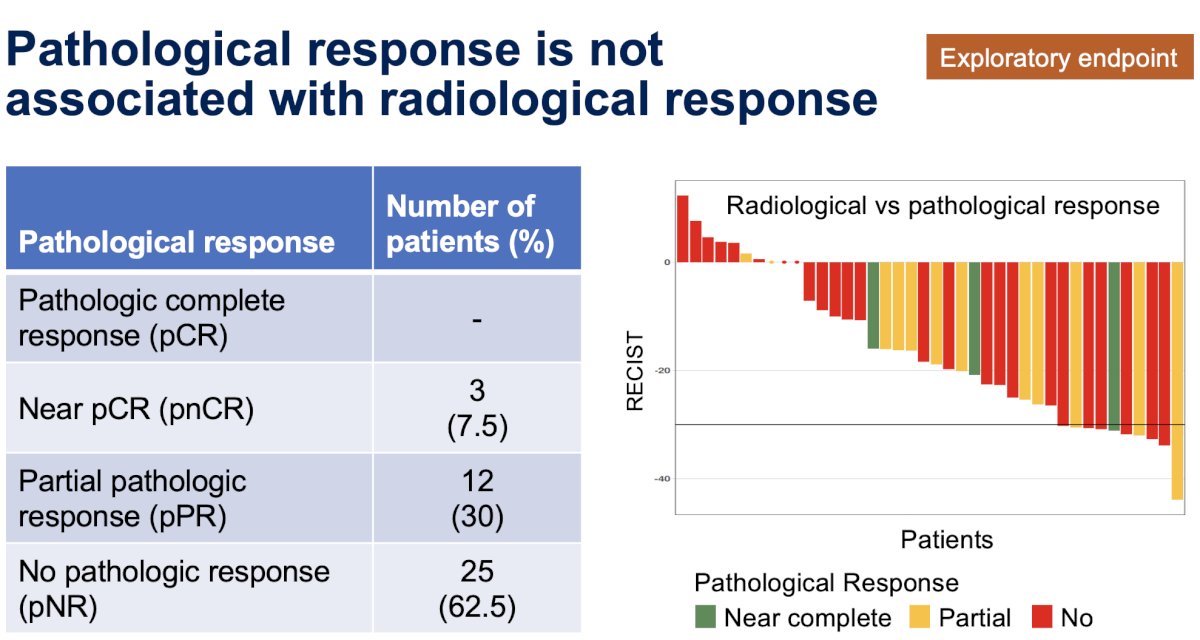
The hypothesis-driven primary endpoint, a radiographic partial response by RECIST 1.1 criteria in the primary tumor in ≥25%, was met and previously reported.1 Notably, however, pathologic response was not associated with radiologic response.
In contrast to adjuvant therapy, where the primary tumor has been extirpated, what are the potential benefits of activating tumor reactive immune cells in the primary lesion?
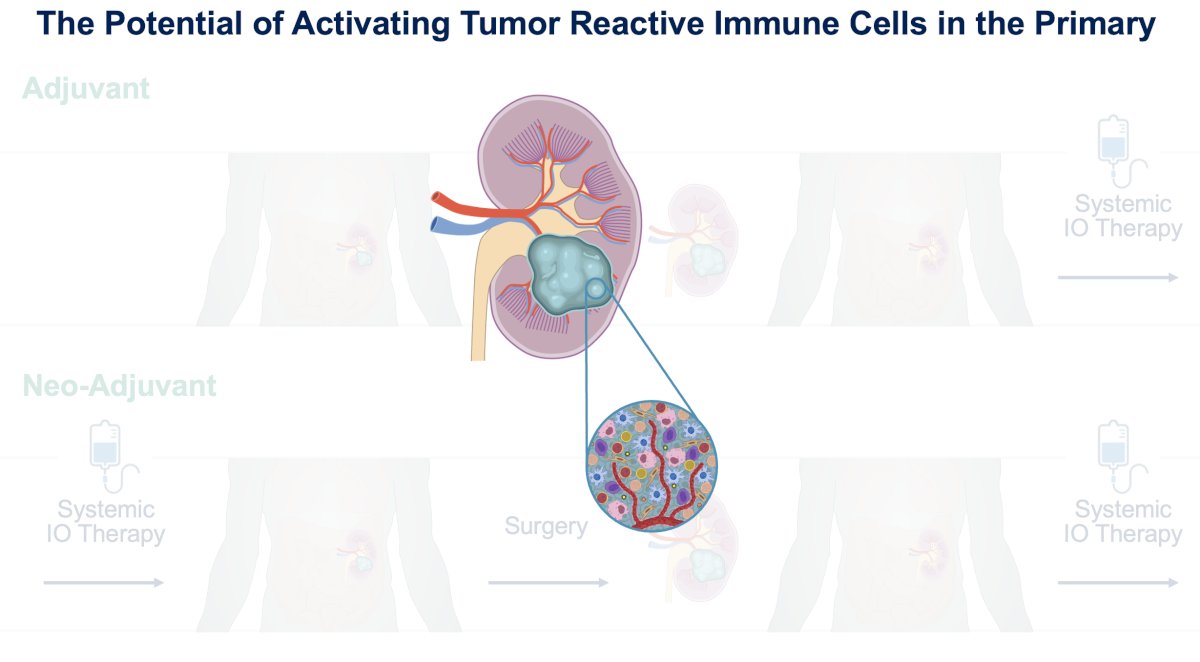
One potential benefit of a neoadjuvant approach is strengthening the anti-cancer immune response. The killing of cancer cells leads to cancer antigen presentation and immune cell priming and activation, creating an ‘immune desert’ phenotype. Subsequent immune cell trafficking to the tumors can lead to immune cell infiltration of the tumors themselves, now creating an ‘immune excluded’ phenotype. The recognition of cancer cells by T-cells and NK cells can reverse T cell exhaustion, creating an ‘immune inflamed’ state. Agents with potential enhanced benefits in these evolving phenotypes are as follows:
- Immune desert: Cytokines, anti-CTLA-4 inhibitors
- Immune excluded: VEGF inhibitors
- Immune inflamed: PD-1/L-1 inhibitors
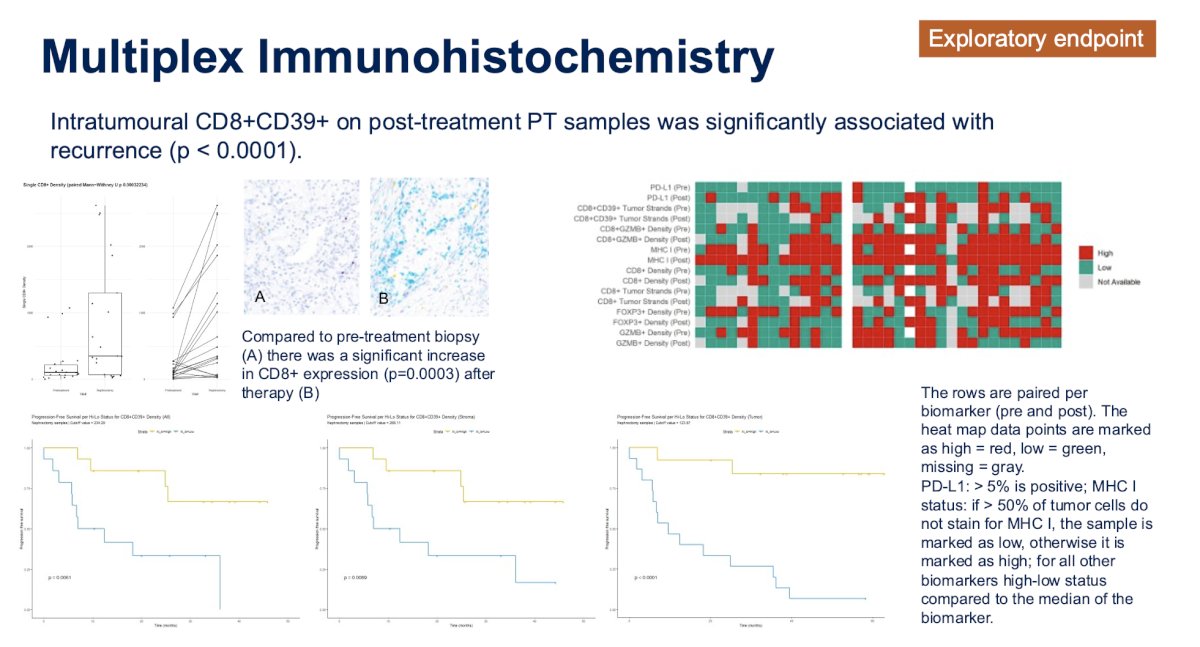
In correlative analyses of paired tumor samples from the NEOAVAX trial, Dr. Bex and colleagues demonstrated that post-PD-1 antibody presence of exposed tumor antigen, but exhausted, T-cells (CD8+,CD39+) associated with positive outcomes, may be a predictor of benefit.
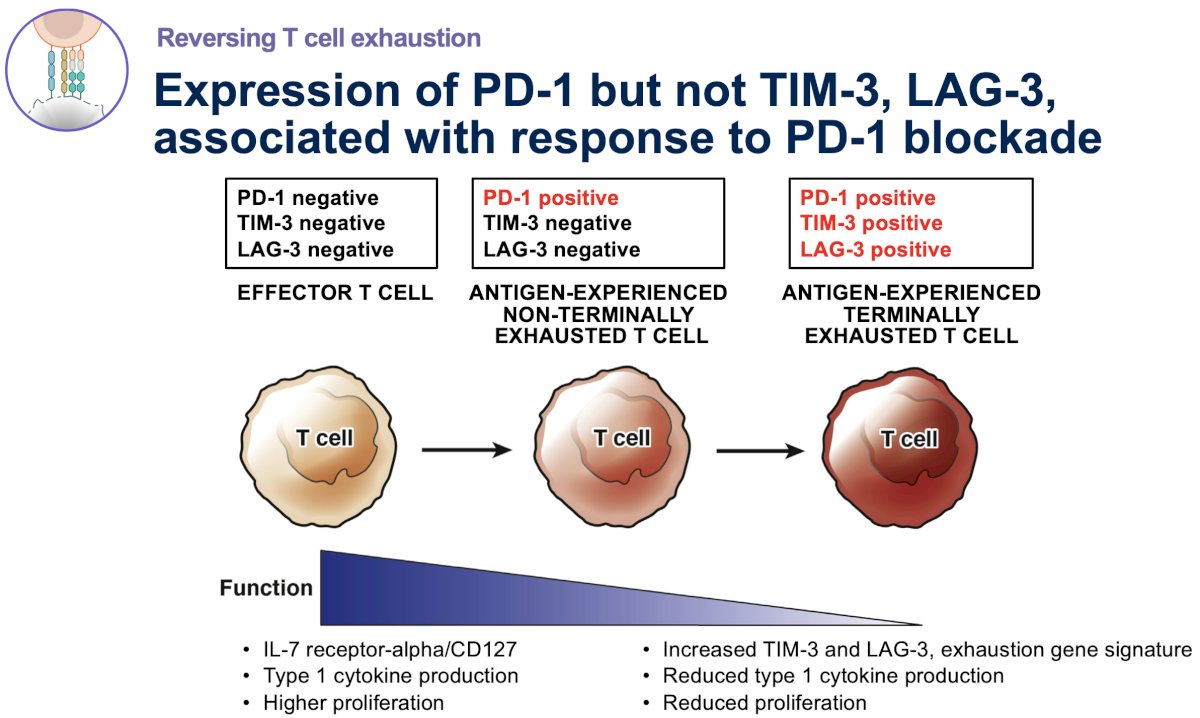
A similar paradigm has been previously shown by Pignon et al. in an ad hoc analysis of the CheckMate-010 trial, which showed that high percentages of CD8+ tumor-infiltrating cells that are PD-1+TIM-3-LAG-3- (i.e., antigen-expressed, non-terminally exhausted cells) were correlated with high levels of T-cell activation and longer median immune-related rPFS and ORR, but expression of TIM-3 and LAG-3 was not.2
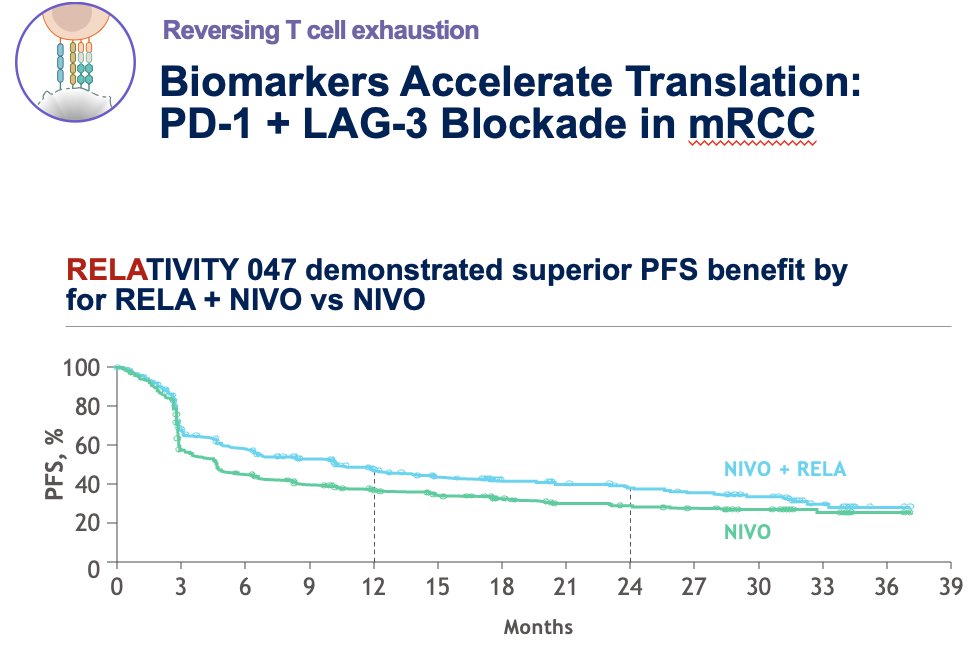
Given that both LAG-3 and PD-1 are immune checkpoints that contribute to T-cell exhaustion, trials of other disease sites have evaluated the blockade of both antigens in an effort to overcome this exhaustion. Tawbi et al. evaluated the combination of relatlimab, a LAG-3–blocking antibody, and nivolumab (anti-PD-1) in patients with previously treated melanoma and demonstrated that this combination was associated with survival benefits, compared to nivolumab monotherapy.3
Analogous trials for metastatic RCC are currently underway (e.g., Rela-RCC and MARIO trials).
Next, Dr. McDermott discussed how translational research can lead to more cures. He noted that the exploratory analysis of the IMmotion010 trial of adjuvant atezolizumab was the first exploration of its type in the adjuvant setting, with paired biopsies helping to address critical questions:
- What drives PD-1 resistance?
- Who should get adjuvant therapy?
This study demonstrated that pre-defined molecular subsets may be associated with outcomes, and that the serum marker Kidney Injury Molecule-1 (KIM-1) is the most robust predictor of benefit to adjuvant therapy.

While DNA is ‘fixed’, it does not express everything – histomes determine what is expressed or not.
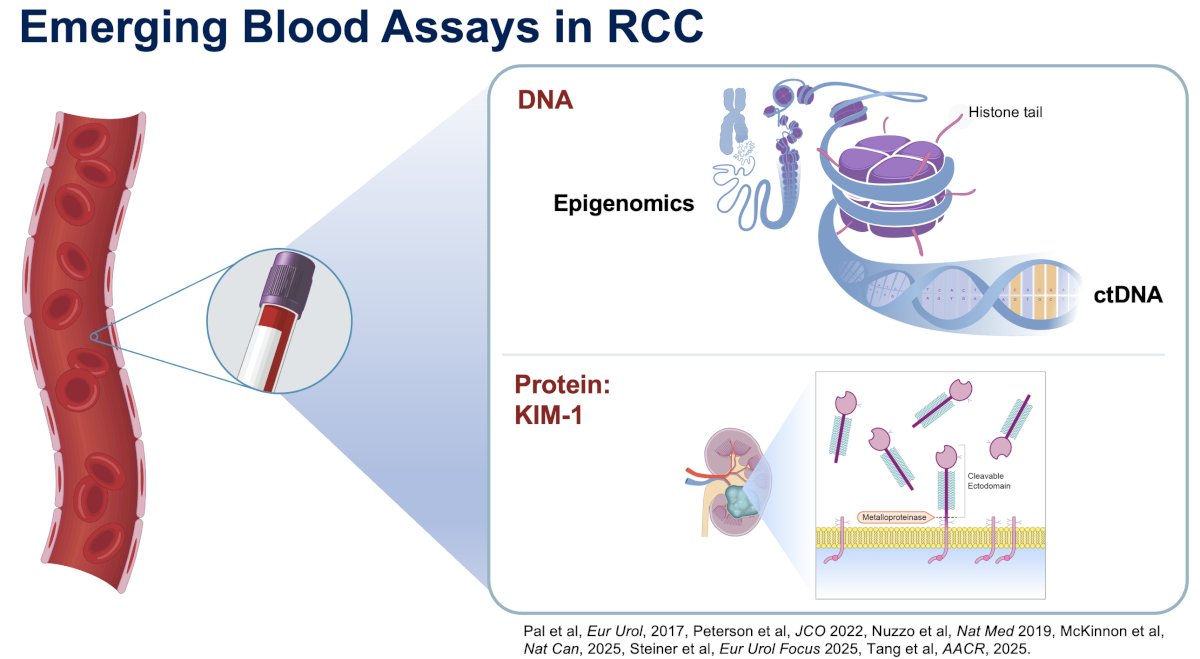
KIM-1 is a blood biomarker associated with RCC outcomes in multiple clinical settings. In the pre-nephrectomy setting:4-6
- Higher KIM-1 levels are associated with higher RCC risk
- Pre-nephrectomy KIM-1 is associated with metastasis-free and overall survival
- KIM-1 levels can be elevated up to 5 years prior to an RCC diagnosis
- KIM-1 can discriminate between benign and malignant tumors

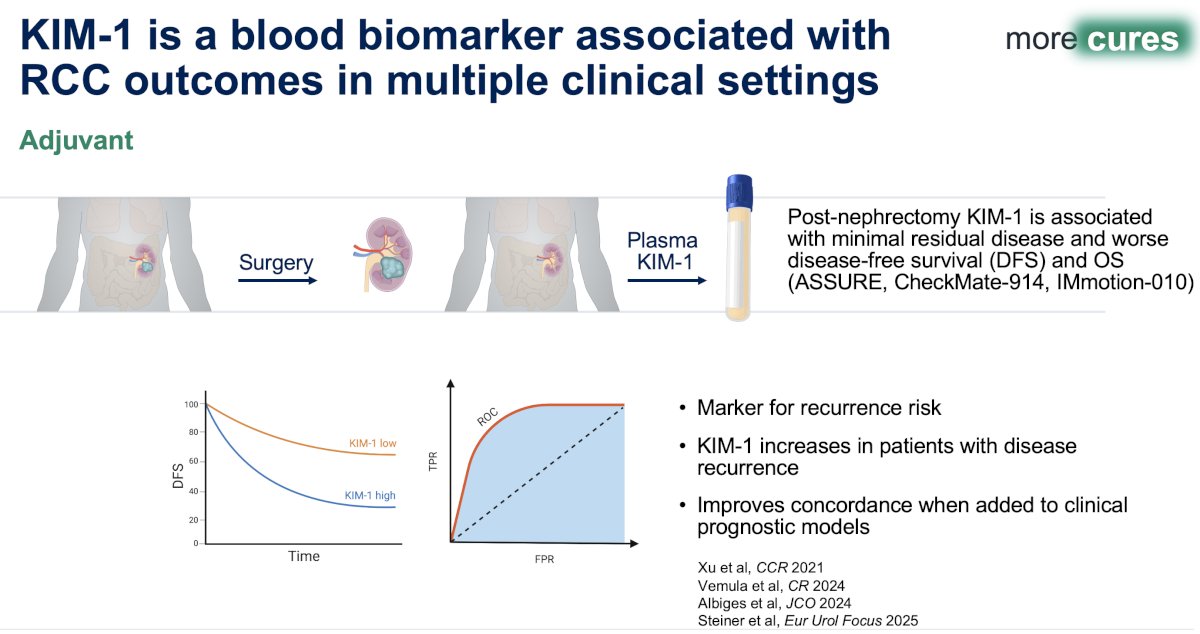
In the adjuvant setting, KIM-1:5-8
- Is associated with minimal residual disease and worse disease-free and overall survivals (ASSURE, CheckMate-914, IMmotion-010)
- Has been shown to be a marker of recurrence risk
- Increases in patients with disease recurrence
- Improves concordance when added to clinical prognostic models
Dr. McDermott concluded his presentation as follows:
- Integrated models are the future of biomarker discovery
- Multi-platform efforts uncover new biology
- Prospective validation in independent cohorts is essential and underway.
- Hypothesis-driven biomarker efforts can lead to novel therapies
- To accelerate translation, build on a strong biologic rationale
- Continue to explore pre-surgical PD-1 and target proteins that might reverse T-cell exhaustion
- Translational research will lead to more cures
- Validated blood-based biomarkers could dramatically improve outcomes
- RCC cooperative groups efforts can make them a reality
Presented by: David F. McDermott, MD, Professor, Chief of Medical Oncology, Department of Medicine, Beth Israel Deaconess Medical Center, Dana-Farber/Harvard Cancer Center, Boston, MA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
References:
- Bex A, Grünwald V, Albers P, et al. A phase II trial of neoadjuvant nivolumab and vaccine (NEO-NIVO-VAC) in high-risk localized renal cell carcinoma (NEOVAX). J Clin Oncol. 2022; 40(16_suppl):289.
- Pignon JC, Jegede O, Shukla SA, Braun DA, Horak CE, Wind-Rotolo M, et al. irRECIST for the evaluation of candidate biomarkers of response to nivolumab in metastatic clear cell renal cell carcinoma: analysis of a phase II prospective clinical trial. Clin Cancer Res. 2019; 25(7):2174–84.
- Tawbi HA, Schadendorf D, Lipson EJ, Ascierto PA, Matamala L, Castillo G, et al. Relatlimab and nivolumab versus nivolumab in untreated advanced melanoma. N Engl J Med. 2022; 386(1):24–34.
- Scelo G, Muller DC, Riboli E, et al. KIM-1 as a blood-based marker for early detection of kidney cancer: a prospective nested case-control study. Clin Cancer Res. 2018; 24(22):5594–5601.
- Xu W, Joyce A, Uzzo R, et al. Plasma kidney injury molecule-1 for preoperative prediction of malignancy and prognosis in patients with renal masses. J Clin Oncol. 2024; 42(16):4506.
- Steiner C, Lalani AA, Motzer RJ, et al. Circulating kidney injury molecule-1 (KIM-1) in association with kidney injury and oncological outcomes in patients with renal cell carcinoma. Eur Urol Focus. 2025.
- Vemula S, Shandilya J, Gong Y, et al. Circulating tumor DNA profiling for genomic characterization and risk stratification in advanced renal cell carcinoma. Cancer Res. 2024;84(8 Suppl):Abstract 2974.
- Albiges L, Ravaud A, Powles T, et al. Pembrolizumab as adjuvant therapy in renal cell carcinoma: subgroup analyses from KEYNOTE-564. J Clin Oncol. 2024;42(16 Suppl):4506.