(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL between May 30th and June 3rd, 2025, was host to a kidney and bladder cancers oral abstract session. Dr. Robert Motzer presented the final analysis from the phase III CheckMate 214 trial of nivolumab + ipilimumab (NIVO+IPI) versus sunitinib for the 1st line treatment of advanced renal cell carcinoma (RCC).
NIVO + IPI is approved for the first-line treatment of patients with IMDC intermediate/poor-risk advanced RCC, based on the results of the phase III CheckMate-214 trial that demonstrated improved overall survival (OS; median: not reached versus 26 months; HR: 0.63, p<0.001) and objective response rates (ORR; 42% versus 27%, p<0.001; complete response: 9% versus 1%) with NIVO + IPI versus sunitinib.1-3 In this report, Dr. Motzer presented the final efficacy and safety results of the CheckMate 214 trial with a long-term median follow-up of > 9 years (111 months).
The study design is illustrated below: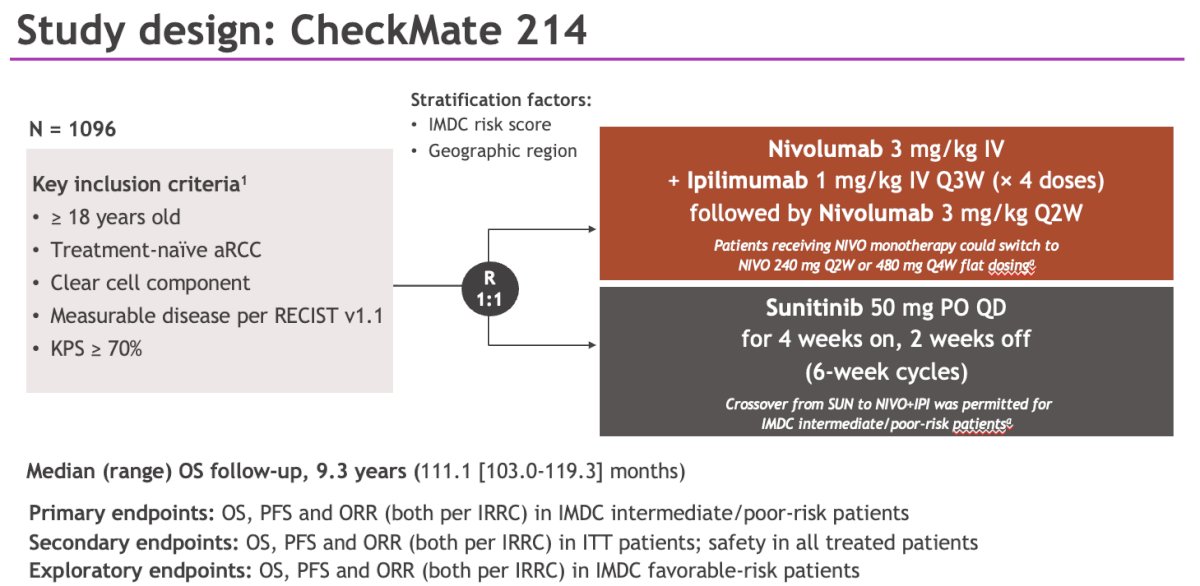
Select baseline characteristics are summarized in the table below. 77% of patients had IMDC intermediate or poor-risk disease. The most common sites of metastases were the lung (69%), followed by bone (21%) and liver (19%).

With a median follow-up of > 9 years, long-term benefits were sustained with NIVO + IPI versus sunitinib in patients with IMDC intermediate or poor risk disease, including improved OS (median: 46.7 vs 26 months; HR: 0.69, 95% CI: 0.59–0.81) and progression-free survival (PFS; median: 12.4 versus 8.5 months; HR: 0.73, 95% CI: 0.61–0.87), as well as more durable responses (median: 82.8 versus 19.8 months). 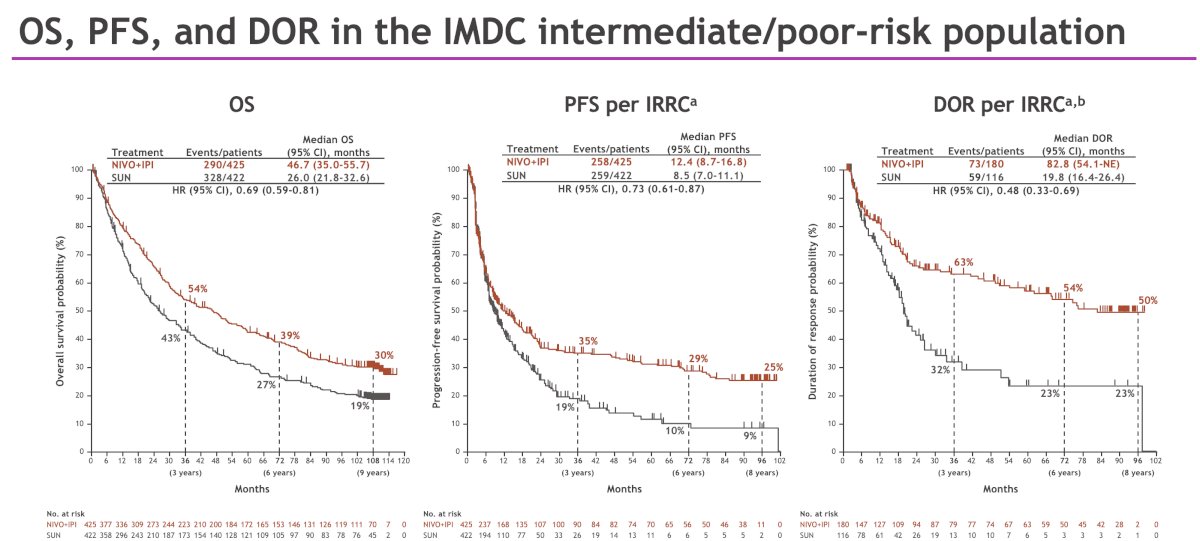
Long-term OS results in patients with IMDC favorable risk disease trended in favor of NIVO + IPI versus sunitinib (median: 77.9 vs 66.7 months), with more durable responses.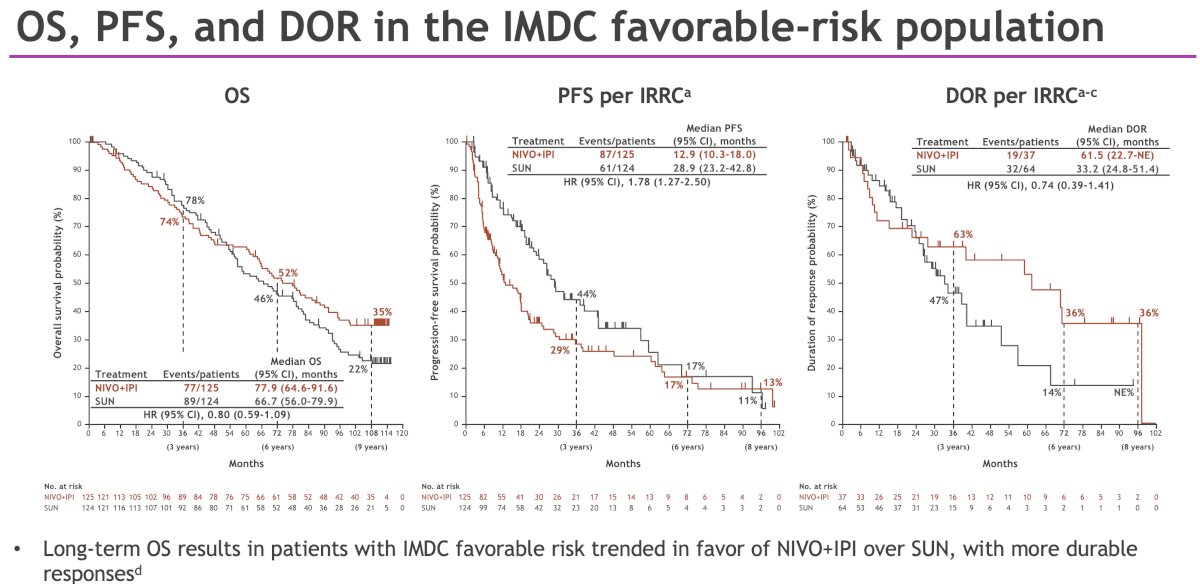
The hazard ratio for overall survival remained stable and in favor of NIVO + IPI versus sunitinib over > 9 years of median follow-up in the intent-to-treat (ITT) population (median: 52.7 vs 37.8 months; HR: 0.71, 95% CI: 0.62–0.82).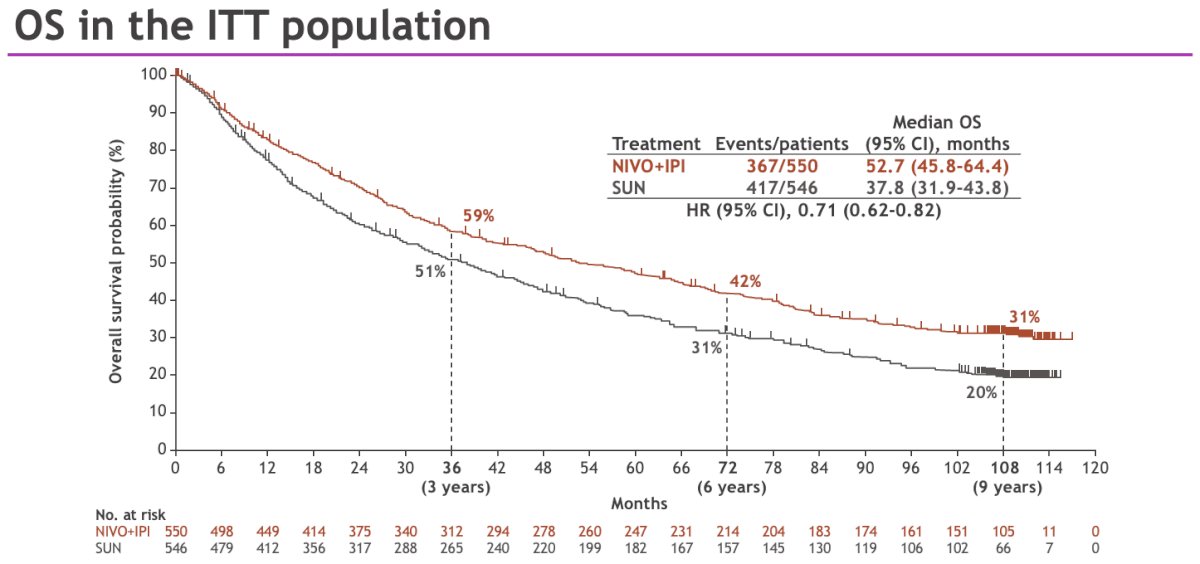
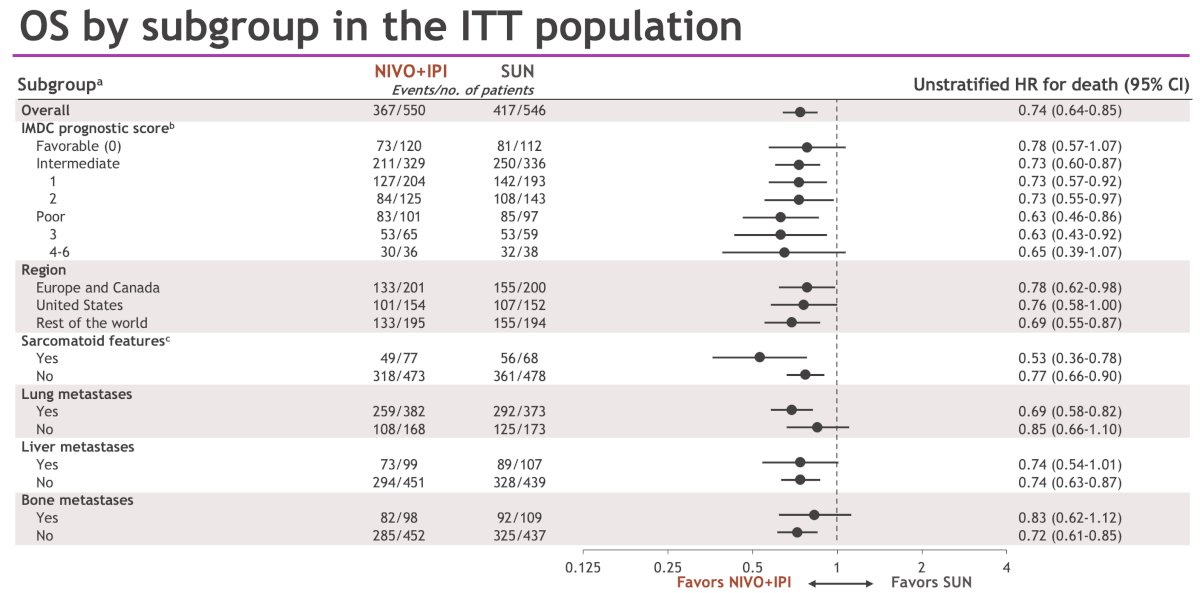
OS in the ITT population was consistently longer with NIVO + IPI versus sunitinib across different subgroups.
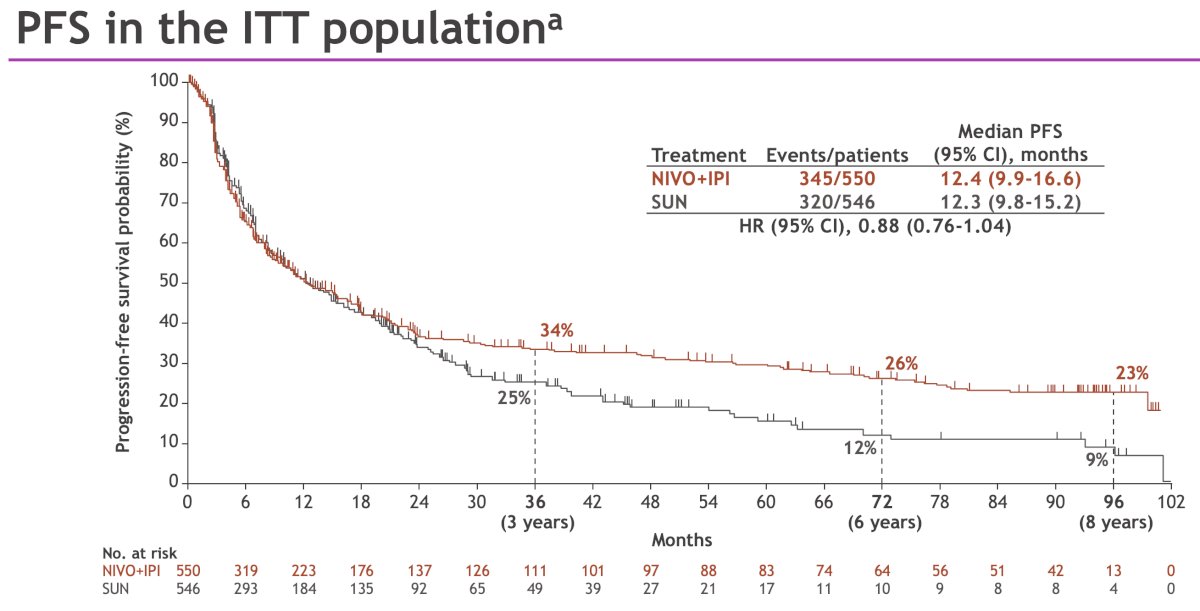
The difference in PFS probabilities between treatment arms remained consistently in favor of NIVO + IPI versus sunitinib from 24 months onwards.
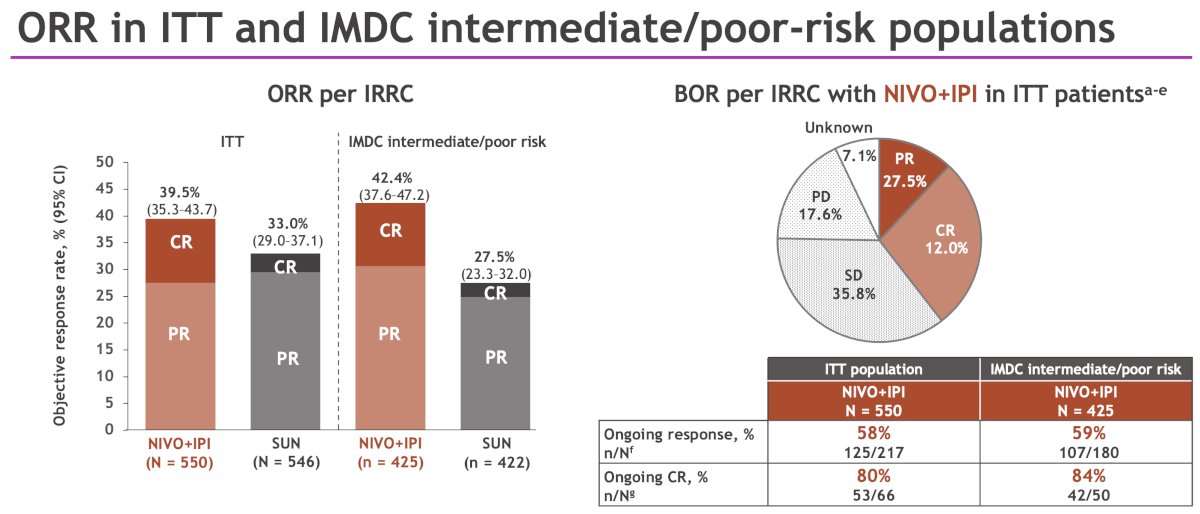
The ORR remained higher with NIVO + IPI versus sunitinib in both the ITT population and in patients with IMDC intermediate/poor risk disease, with NIVO + IPI achieving more complete responses.
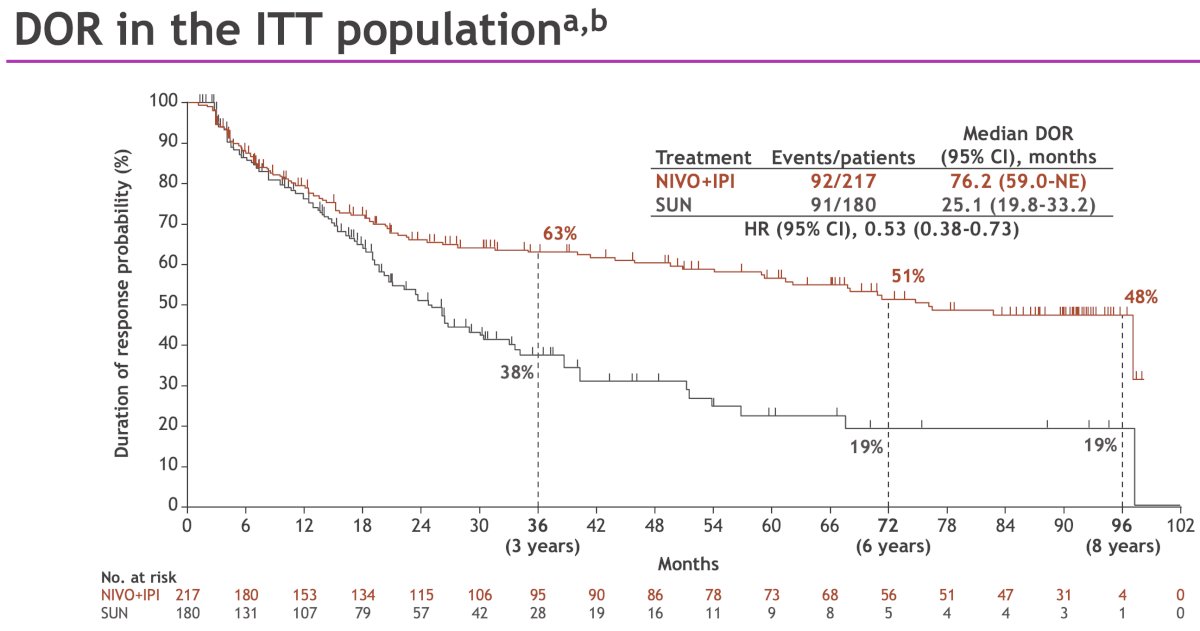
NIVO + IPI demonstrated a long-term duration or response advantage, compared with sunitinib, in the ITT population.
Overall, 31% of the NIVO + IPI treated patients received corticosteroids to manage any-grade immune-mediate adverse events; 21% and 11% received corticosteroids continuously for ≥ 14 days and ≥ 30 days, respectively.
Comparable overall rates of treatment-related adverse events occurred with NIVO + IPI versus sunitinib (94% vs 98%); however, fewer grade≥ 3 events were reported with NIVO + IPI (49% versus 64%). No new deaths due to study drug toxicity occurred since the previous follow-up.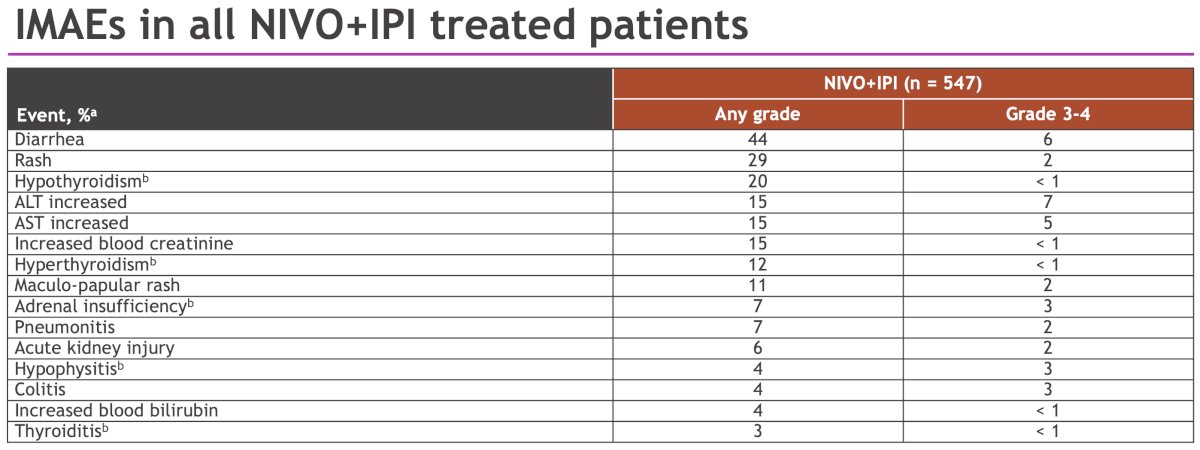
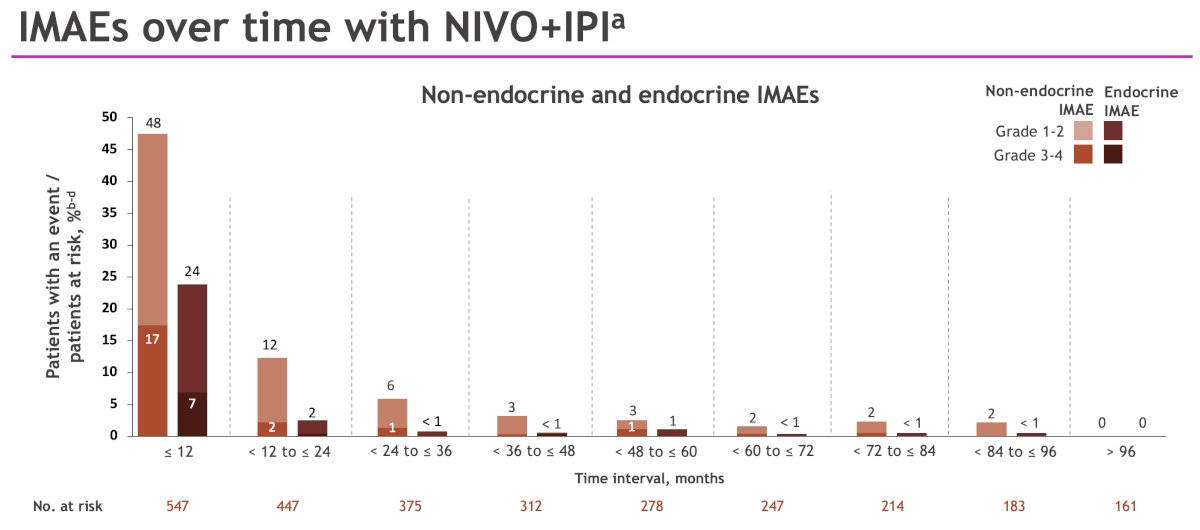
Most immune-mediated adverse events in the NIVO + IPI arm occurred early in the course of treatment.
Dr. Motzer concluded his presentation as follows:
- CheckMate 214 provides the longest reported follow-up to date of any immuno-oncology combination therapy for first-line clear cell RCC
- NIVO + IPI continued to demonstrate improved survival with complete and durable response benefits compared with sunitinib in the overall study population of patients with previously untreated advanced RCC
- Safety and tolerability with long-term follow-up were manageable and consistent with previous follow-ups
- These results continue to support NIVO + IPI as a standard of care for patients with previously untreated advanced RCC
- Subcutaneous NIVO has been shown to provide clinical equipoise to standard IV dosing3 and may provide an alternative for maintenance NIVO after NIVO+IPI in patients with advanced RCC4-6
Presented by: Robert Motzer, MD, Attending Physician, Medical Oncologist, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: CheckMate 214 Final Overall Survival Data: Long-Term Survival Benefits of Ipi/Nivo in Kidney Cancer - Michael Serzan
- Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med. 2018;378:1277–90.
- Tannir NM, Plimack ER, Grunwald V, et al. Efficacy and safety of nivolumab plus cabozantinib versus sunitinib in previously untreated advanced renal cell carcinoma: updated results from CheckMate 9ER. Ann Oncol. 2024;35:1026–38.
- Albigès L, Burotto M, Ravaud A, et al. Health-related quality of life and patient-reported outcomes with nivolumab plus cabozantinib vs sunitinib: CheckMate 9ER trial update. Ann Oncol. 2025;36:99–107.
- Bristol Myers Squibb. OPDIVO QVANTIG (nivolumab and hyaluronidase-nvhy). Princeton, NJ: Bristol Myers Squibb; 2024.
- Lonardi S, Tabernero J, Sobrero A, et al. Clinical activity of combination immunotherapy in advanced cancer. Poster presented at: American Society of Clinical Oncology (ASCO) 2021 Annual Meeting; 2021 Jun 4–8; Virtual. Poster 2575.
- Zhao Y, Kim JW, Patel MR, et al. Tumor microenvironment changes with dual immune checkpoint blockade in renal cancer. Poster presented at: Society for Immunotherapy of Cancer (SITC) 2024 Annual Meeting; 2024 Nov 6–10; Houston, TX. Poster 524.